Can you make notes on hydatid cyst of liver
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for comprehensive notes. Here are the complete notes on Hydatid Cyst of the Liver:
Hydatid Cyst of the Liver (Hepatic Echinococcosis)
1. Aetiology & Causative Organisms
Hydatid disease (echinococcosis) is a zoonosis caused by the larval stage of the tapeworm Echinococcus. Three species are clinically relevant:
| Species | Disease | Features |
|---|---|---|
| E. granulosus | Cystic echinococcosis | Most common; well-defined fluid-filled cysts |
| E. multilocularis | Alveolar echinococcosis | Highly invasive; solid masses mimicking carcinoma; mortality ~90% if untreated |
| E. vogeli | Polycystic echinococcosis | Intermediate aggressiveness; polycystic lesions |
2. Epidemiology
- Endemic in sheep-raising regions: Mediterranean Europe, Middle East, Africa, Far East, South America, Australia, New Zealand
- Dogs are the definitive host; sheep are the major intermediate host (also yaks, goats, camels)
- Humans are accidental intermediate hosts — no human-to-human transmission
- Diagnosed equally in males and females; average age ~45 years
3. Life Cycle & Pathogenesis
Dog (definitive host)
↓ eggs shed in feces
Contaminated food/water/vegetables
↓ ingested by humans
Small intestine → eggs hatch → oncospheres released
↓ penetrate intestinal mucosa
↓ enter bloodstream/lymphatics
Liver (70%) > Lungs (20%) > Kidney, Spleen, Brain, Bone
↓ vesiculation
Hydatid cyst develops
Cyst wall structure (3 layers):
- Outer adventitial (pericyst) — host-derived fibrous capsule; can calcify
- Middle ectocyst (laminated layer) — acellular, gelatinous outer worm-derived membrane
- Inner endocyst (germinal layer) — inner worm-derived germinal membrane; produces brood capsules and daughter cysts
Key contents:
- Brood capsules — small intracystic masses in which scoleces (future worm heads) develop
- Daughter cysts — true replicas of the mother cyst
- Hydatid sand — freed brood capsules + scoleces floating in hydatid fluid
- Scolex contains a rostellum with 20–50 hooklets and 4 suckers
4. Clinical Features
Symptoms (largely asymptomatic until complications occur)
- Abdominal pain (most common)
- Dyspepsia, vomiting
- Urticarial rash, pruritus (hypersensitivity)
Signs
- Hepatomegaly (most frequent sign; usually right lobe)
- Palpable mass
- Jaundice (~8%) — biliary obstruction
- Fever (~8%) — secondary infection
Complications
| Complication | Details |
|---|---|
| Rupture into biliary tree | Most common rupture site; → cholangitis, biliary obstruction, jaundice |
| Bacterial superinfection | Mimics pyogenic abscess (up to 20% of hepatic cases) |
| Free rupture into peritoneum | → disseminated echinococcosis, anaphylaxis |
| Rupture into pleura/bronchi | → dyspnea, hemoptysis |
| Rupture into pericardium | Rare but life-threatening |
| Portal hypertension | Rare |
| Budd-Chiari syndrome | Rare |
| Pancreatitis | Rare |
Eosinophilia is not a feature unless the cyst ruptures
5. Imaging
Ultrasound (first-line — most widely used)
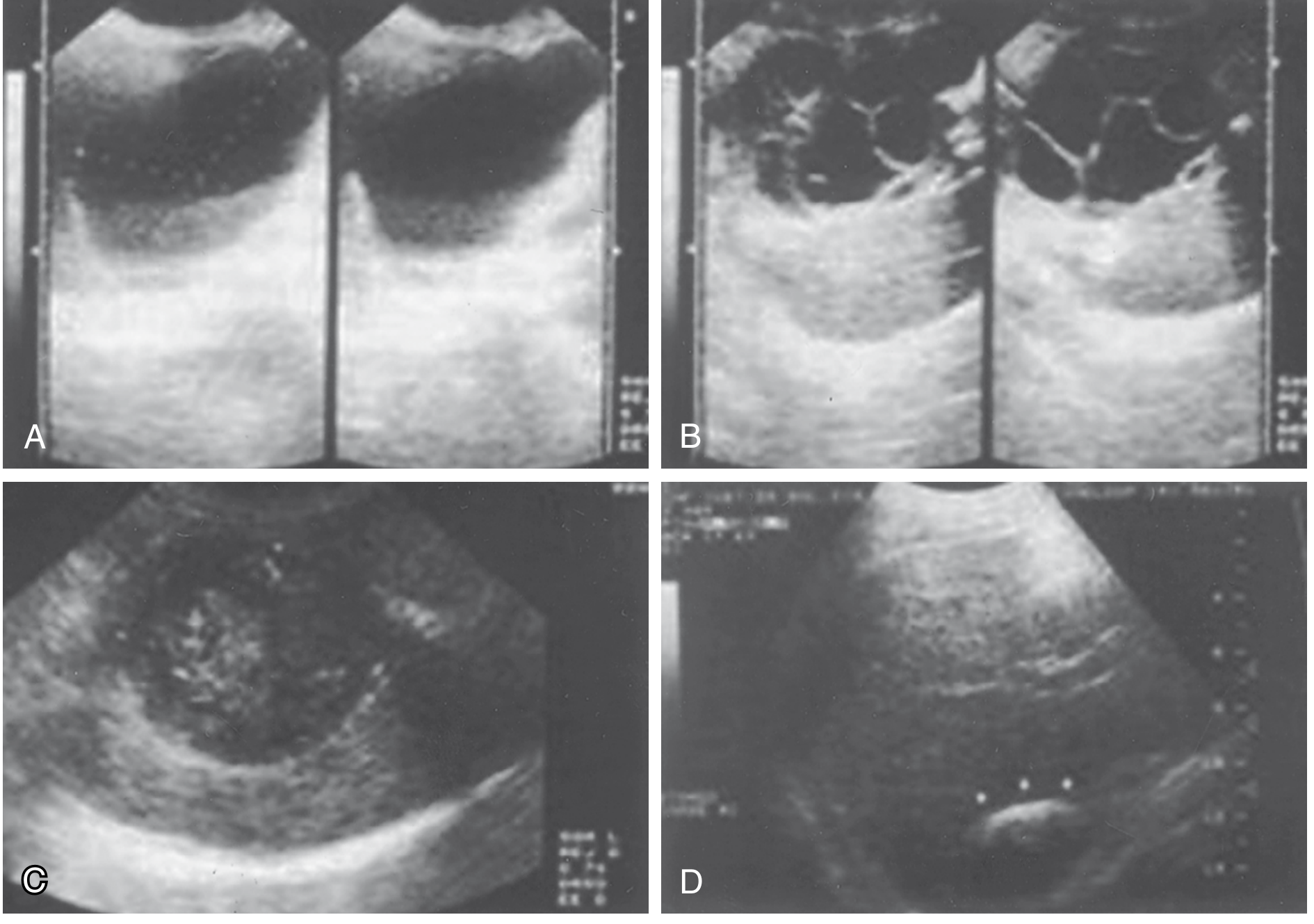
Gharbi classification (also WHO-IWGE classification) stages cysts from simple unilocular to calcified.
Diagnostic US features:
- Well-circumscribed cyst with budding signs on the membrane
- Free-floating hyperechoic hydatid sand
- Rosette pattern — daughter cysts present
- Eggshell calcification — highly suggestive
CT / MRI
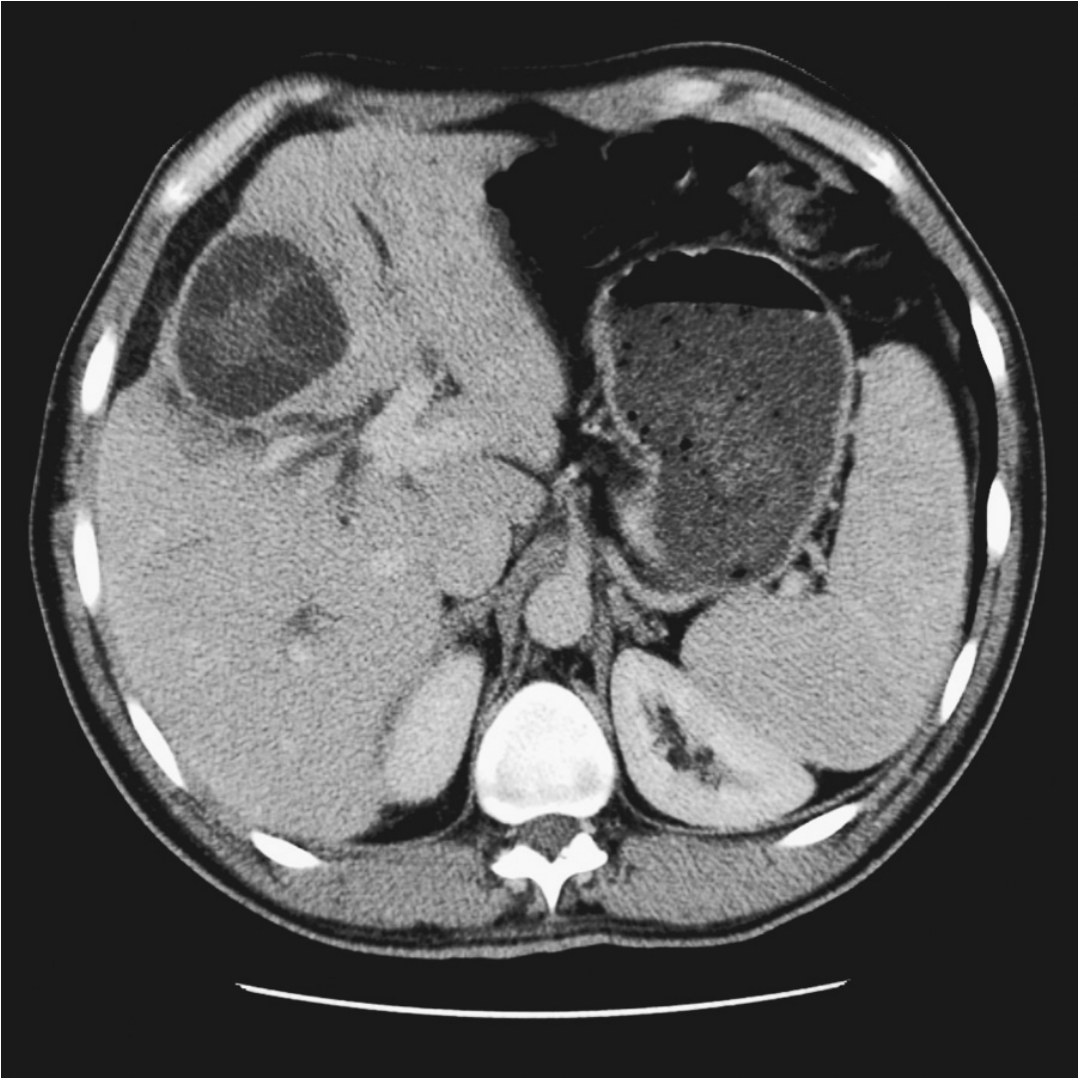
- Avascular cysts with ring enhancement
- Multiple daughter cysts with intracystic septations
- Peripheral focal calcifications
- Fluid density varies with proteinaceous debris
- Better than US for extrahepatic disease and hepatic anatomic relationships
ERCP / PTC
- Indicated when biliary involvement is suspected
Plain X-ray
- Ring-like calcifications visible in up to one-fourth of hepatic cysts (E. granulosus)
6. Laboratory / Serology
| Test | Details |
|---|---|
| ELISA | Best serologic test; sensitivity 84–90% |
| Weinberg reaction | Older complement fixation test; up to 38% false-negative rate |
| Eosinophilia | Only present if cyst ruptures; otherwise absent |
| Routine bloods | Usually normal LFTs; leukocytosis if infected |
| Casoni skin test | Nonspecific; no longer recommended |
| Cyst fluid analysis | Detection of protoscolices or acid-fast hooklets confirms diagnosis |
All serologic tests are plagued by low sensitivity and specificity; imaging is more reliable
7. Gross Pathology

- ~75% located in the right lobe of the liver
- ~75% are solitary
- Slow, spherical growth pattern
- Degenerating cysts: vacuolation of membranes → calcification of wall (calcification does not always imply the cyst is dead)
8. Treatment
General Principles
- Most cysts should be treated
- Conservative management is appropriate for small, asymptomatic, densely calcified cysts in elderly patients
- Preoperative albendazole is recommended to reduce spillage risk; steroids and epinephrine should be on standby for anaphylaxis
A. Surgery (Gold Standard)
Preparation:
- Pack off the abdomen to prevent spillage (anaphylaxis + dissemination risk)
- Aspirate through a closed suction system
- Flush with scolicidal agent (hypertonic saline is standard)
Surgical options:
| Approach | Procedure |
|---|---|
| Conservative | Unroofing → drainage/evacuation, marsupialization, omentoplasty |
| Radical | Total pericystectomy, partial hepatectomy (formal resection without entering cyst) |
| Laparoscopic | Drainage and unroofing; encouraging results in selected cases |
| Biliary involvement | Suture closure of bile duct communication; major biliary repair; postoperative ERCP |
- Radical and conservative approaches are equally effective
- Recurrence rate: 1–20% (generally ≤5% at experienced centres)
- Calcified cysts need not be removed
B. PAIR (Percutaneous Minimally Invasive)
Puncture → Aspiration → Injection (scolicidal agent) → Re-aspiration
- Previously contraindicated; now accepted in highly selected patients
- Two small RCTs show similar success rates to surgery (both limited by small sample sizes)
- Best for uncomplicated cysts; requires concomitant antihelminthic cover
C. Medical Therapy (Antihelminthics)
| Drug | Dose |
|---|---|
| Albendazole (preferred) | 10 mg/kg/day in 2 divided doses × 28 days; repeat 3–4 cycles with 2-week breaks between cycles |
| Mebendazole | Alternative; higher doses required |
- Effective at shrinking cysts in E. granulosus; complete disappearance in <50%
- Used preoperatively to reduce spillage risk
- Monotherapy (without drainage/resection) reserved for:
- Widely disseminated disease
- Poor surgical candidates
9. E. multilocularis vs E. granulosus — Key Differences
| Feature | E. granulosus (Cystic) | E. multilocularis (Alveolar) |
|---|---|---|
| Cyst type | Well-defined fluid-filled cysts | Solid invasive masses |
| Appearance | Unilocular/multilocular cysts | Alveoli-like microvesicles |
| Growth pattern | Expansile | Infiltrative ("invasion" of parenchyma) |
| CT | Calcified cysts, daughter cysts | Scattered calcified necrotic tissue |
| Mimics | Simple hepatic cyst, abscess | Cirrhosis, hepatocellular carcinoma |
| Prognosis | Good with treatment | Poor; mortality ~90% without treatment |
| Surgery | Usually curative | Curative in only ~1/3; often inoperable at diagnosis |
| Medical | Albendazole effective | Long-term albendazole indefinitely (if inoperable) |
10. Key Points Summary
- Caused by E. granulosus (most common), a tapeworm whose definitive host is the dog
- Humans are accidental intermediate hosts infected via fecally contaminated food
- Liver is most commonly affected (70%), followed by lungs (20%)
- Cyst wall: pericyst (host) / ectocyst (outer worm) / endocyst (germinal, inner worm)
- Largely asymptomatic until complications develop
- Most dangerous complication: free rupture → anaphylaxis
- Most common rupture site: biliary tree → cholangitis
- Ultrasound is the primary imaging tool; rosette sign and eggshell calcification are pathognomonic
- ELISA is best serology (84–90% sensitive); Casoni test is obsolete
- Treatment: Surgery ± preoperative albendazole is the mainstay; PAIR for selected cases
- Hypertonic saline is the standard scolicidal agent used intraoperatively
Sources: Sabiston Textbook of Surgery, p. 1891–1892 | Sleisenger & Fordtran's GI and Liver Disease, p. 1589 | Goldman-Cecil Medicine, p. 1599–1600 | Jawetz Melnick & Adelberg's Medical Microbiology
This is a shared conversation. Sign in to Orris to start your own chat.