Basal cell carcinoma Treatment
Reading File
Finding Sources
Searching PubMed
"basal cell carcinoma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer.
Basal Cell Carcinoma (BCC) - Treatment
BCC is the most common human malignancy (~2-3 million cases/year in the US). It rarely metastasizes but causes significant local destruction. The goal of treatment is complete tumor removal with the highest cure rate and best cosmetic outcome. Treatment choice depends on tumor subtype, size, location, and whether it is primary or recurrent.
Management Algorithm
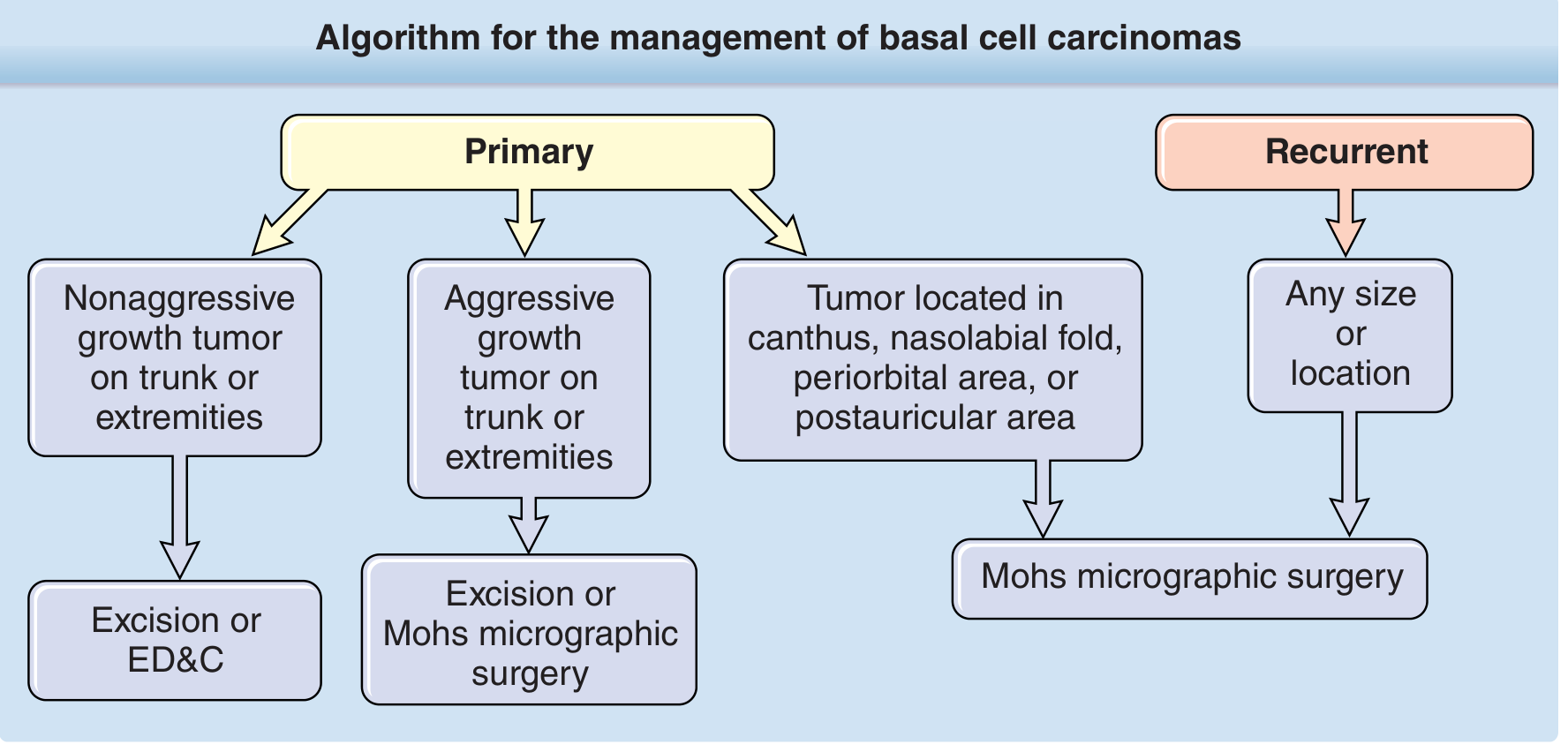
1. Mohs Micrographic Surgery (MMS) - Treatment of Choice for High-Risk BCC
MMS offers the lowest recurrence rates of all modalities. It excises tumor in sequential layers, mapping 100% of the surgical margins using frozen sections before proceeding.
Cure rates:
- Primary BCC: ~1% recurrence at 5 years
- Recurrent BCC: ~4-5.6% recurrence at 5 years
- Compare to: standard excision (10%), C&D (7.7%), radiation (8.7%), cryotherapy (7.5%)
Indications (NCCN Guidelines):
- High-risk anatomic locations: nose, eyelids, ears, lips, periorbital area, nasolabial fold, temples (the "H-zone")
- Morpheaform / infiltrative / micronodular histologic subtypes
- Poorly defined clinical margins
- Diameter >2 cm
- Any recurrent BCC regardless of size or location
- Where tissue conservation is important
Margins for Mohs:
- Nodular BCC: typically 4 mm margins adequate
- Infiltrative/micronodular: may require 5-10 mm; may need excision of muscle, cartilage, or periosteum
- Fitzpatrick's Dermatology, p. 3794-3795
2. Standard Surgical Excision
- Appropriate for most low- to intermediate-risk BCCs
- Nodular BCC on trunk/extremities: excise with 3-5 mm margins
- Provides histologic evaluation of specimen
- Breadloaf sectioning may miss positive margins - inferior to MMS margin control
- 5-year recurrence rate for primary BCC: ~10%
- Fitzpatrick's Dermatology, p. 1918; Textbook of Family Medicine 9e, p. 957
3. Electrodesiccation and Curettage (ED&C)
- One of the most commonly used modalities
- Operator-dependent: cure rates range 81-99% depending on skill
- Cure rates by size (primary, non-fibrosing BCC):
- <1 cm: 98.8%
- 1-2 cm: 95.5%
-
2 cm: 84%
- Not recommended for: large BCCs, morpheaform subtype, recurrent BCCs, face (except low-risk sites)
- Best for: small, well-defined, superficial/nodular BCCs on trunk and extremities
- Fitzpatrick's Dermatology, p. 1918
4. Cryosurgery
- Requires two freeze-thaw cycles with tissue temperature reaching -50°C
- Normal margin tissue must also be frozen to eradicate subclinical extension
- 5-year recurrence: 4-17% in systematic reviews; some series report up to 99% cure
- Complications: hypertrophic scarring, post-inflammatory pigmentary changes
- Cosmetic results inferior to surgical excision
- Infrequently used; poor wound healing in some patients
- Fitzpatrick's Dermatology, p. 3825; Textbook of Family Medicine 9e
5. Topical Treatments (Superficial BCC only)
Imiquimod 5% cream
- FDA-approved for biopsy-confirmed, small (<2 cm) superficial BCC
- Toll-like receptor 7 agonist - induces IFN-α, TNF-α, boosts Th1 immunity
- Dose: 5 days/week for 6 weeks
- Clearance rates: 73-75% (clinical and histologic); ~80% clear at 2 years
- Nodular BCC: ~53% clearance (not optimal)
- Side effects: local skin reactions (erythema, erosion); severity correlates with efficacy
5-Fluorouracil (5-FU) cream
- For superficial BCC on trunk/limbs: twice daily for up to 12 weeks
- Histologic cure rate: ~90%; mean time to clinical cure: 10.5 weeks
- Well tolerated; good cosmetic outcome; mostly mild erythema, no scarring
- Fitzpatrick's Dermatology, p. 1918; Textbook of Family Medicine 9e, p. 957
6. Radiation Therapy (RT)
- Used for patients who cannot undergo surgery, or to achieve a better cosmetic result in certain sites
- 5-year recurrence rate: ~8.7% for primary BCC
- Surgery generally preferred over RT when possible, as long-term recurrence in irradiated fields is harder to detect and manage
- Useful in elderly patients not fit for surgery
7. Photodynamic Therapy (PDT)
- Good cosmetic outcomes reported
- Long-term follow-up data still limited
- Best suited for superficial BCCs
- Not considered first-line due to limited comparative data vs. surgery
- Fitzpatrick's Dermatology, p. 1917
8. Hedgehog Pathway Inhibitors (Systemic - Advanced/Metastatic BCC)
For locally advanced or metastatic BCC not amenable to surgery or radiation, two FDA-approved oral SMO (smoothened) inhibitors exist:
| Drug | Brand | Dose | Indication |
|---|---|---|---|
| Vismodegib | Erivedge | 150 mg PO daily | Metastatic BCC; locally advanced BCC |
| Sonidegib | Odomzo | 200 mg PO daily | Locally advanced BCC |
Mechanism: The hedgehog (HH) pathway is disrupted in ~90% of sporadic BCCs via loss-of-function mutations in PTCH1 (tumor suppressor) or activating mutations in SMO. These drugs block SMO, silencing unregulated HH signaling.
Efficacy: Highly effective, particularly in patients with basal cell nevus (Gorlin-Goltz) syndrome.
Common adverse effects:
- Dysgeusia / ageusia (taste loss)
- Alopecia
- Fatigue
- Muscle spasms / myopathy
Monitoring: Baseline serum creatine kinase (CK) and creatinine before starting; monitor for musculoskeletal symptoms.
Critical warning - Embryofetal toxicity (Boxed warning):
- Both drugs are teratogenic and embryotoxic
- Confirm negative pregnancy test within 7 days before starting
- Contraception required during and after treatment
- Exposure possible through seminal fluid
- Fitzpatrick's Dermatology, p. 3828; Katzung's Basic & Clinical Pharmacology 16e, p. 1691
For Gorlin-Goltz syndrome: A 2024 systematic review (PMID 38867459) confirms vismodegib as the standard systemic option, and a 2025 systematic review (PMID 40522768) identified genetic alterations (secondary SMO mutations, SUFU mutations) underlying resistance to hedgehog inhibitors.
9. Chemotherapy (Metastatic BCC - Rare)
- Platinum-based chemotherapy is used for metastatic BCC when hedgehog inhibitors have failed or are not tolerated
- BCC metastasis is extremely rare (<0.1% of cases)
Summary Table: Treatment by BCC Type
| BCC Type / Scenario | Preferred Treatment | Alternatives |
|---|---|---|
| Superficial BCC, trunk/extremities | Excision or ED&C | Imiquimod, 5-FU, PDT |
| Nodular BCC, low-risk site | Excision (3-5 mm margins) or ED&C | Cryotherapy |
| Aggressive subtype (morpheaform, infiltrative) | MMS | Standard excision with wider margins |
| High-risk anatomic site (H-zone face) | MMS | Standard excision, RT |
| Recurrent BCC (any size/location) | MMS | RT |
| BCC >2 cm | MMS | Standard excision |
| Locally advanced / unresectable BCC | Vismodegib or Sonidegib | Platinum-based chemo |
| Metastatic BCC | Vismodegib | Platinum-based chemo |
Follow-Up
Patients with BCC have approximately a 30% higher risk than the general population of developing another BCC. Recommended surveillance:
- Full-body skin examination at least twice yearly for the first 2 years
- Then yearly if no new lesions appear
- Sun protection counseling at every visit
- Textbook of Family Medicine 9e, p. 957
This is a shared conversation. Sign in to Orris to start your own chat.