Give me 10 common heart disease ECG changes and ECG image of those
Reading File
Finding Sources
Searching the Web
ECG changes heart disease STEMI LBBB atrial fibrillation VT LVH example images
Finding Sources
Searching the Web
STEMI ECG ST elevation myocardial infarction example ECG image site:litfl.com OR site:ecgwaves.com
Finding Sources
Searching the Web
atrial fibrillation ventricular tachycardia LVH prolonged QT bundle branch block ECG images litfl.com
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
LVH left ventricular hypertrophy ECG prolonged QT RBBB right bundle branch block pathological Q waves ECG strip image
Loading Image
Loading Image
Searching the Web
T wave inversion ECG ischemia first degree AV block complete heart block Wolff-Parkinson-White ECG strip images site:litfl.com
Loading Image
I now have all the images and content needed. Here is the complete guide:
10 Common Heart Disease ECG Changes
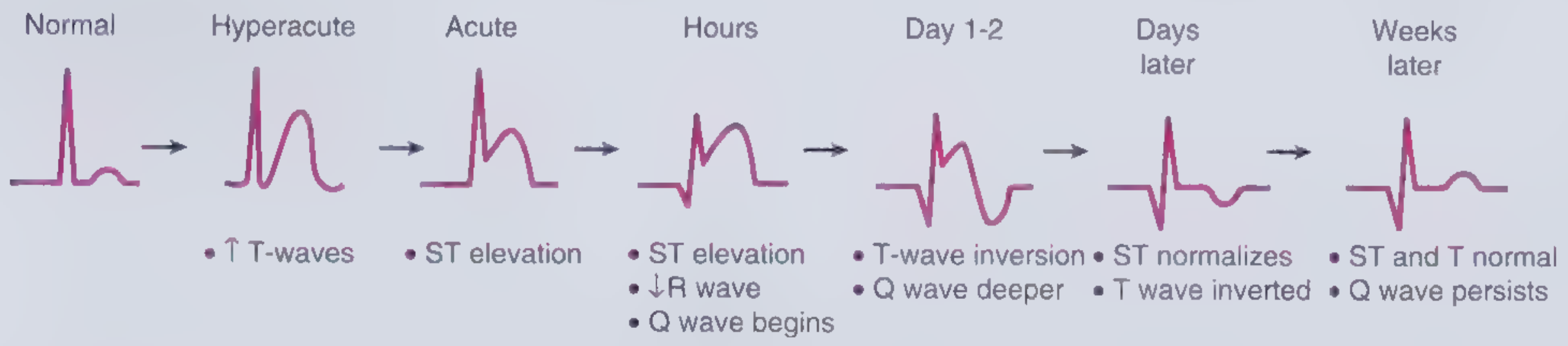
1. ST-Segment Elevation (STEMI)
Condition: Acute ST-Elevation Myocardial Infarction
ECG Features:
- ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads
- Reciprocal ST depression in mirror-image leads
- Hyperacute (tall, peaked) T waves in the very early phase
- Q waves develop within hours and persist as a scar marker
- New LBBB in the context of chest pain is treated as a STEMI-equivalent
Evolution of ECG changes from Normal → Hyperacute → Acute → Hours → Days → Weeks:
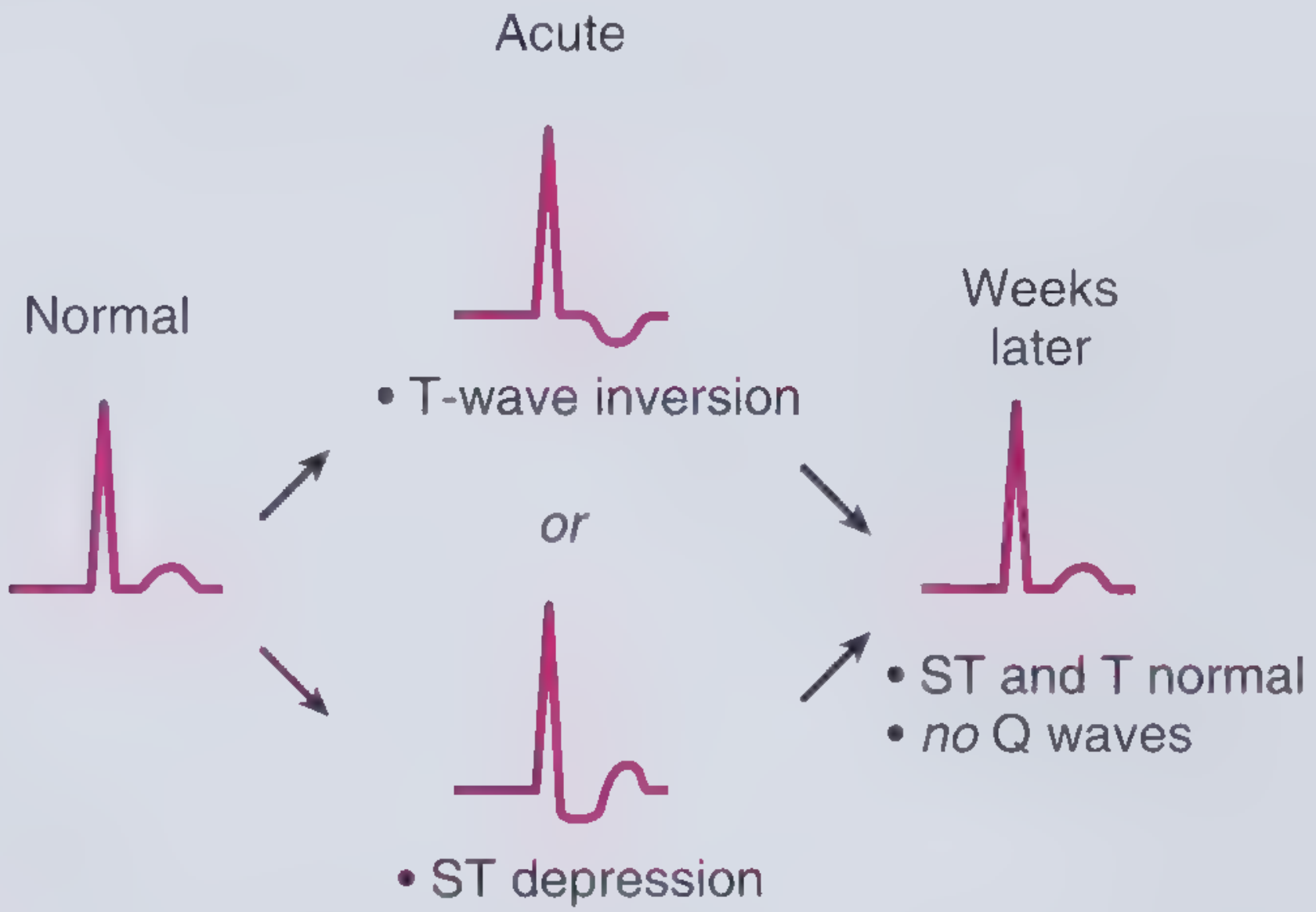
2. ST-Segment Depression / T-Wave Inversion (NSTEMI / UA)
Condition: Non-ST Elevation Myocardial Infarction / Unstable Angina / Subendocardial Ischemia
ECG Features:
- New horizontal or downsloping ST depression ≥0.05 mV in ≥2 contiguous leads
- T-wave inversion ≥0.1 mV in ≥2 contiguous leads with prominent R wave or R/S >1
- No Q waves (non-transmural injury)
- ECG may be normal in UA
3. Pathological Q Waves (Old / Completed MI)
Condition: Prior (completed) myocardial infarction
ECG Features:
- Q wave duration ≥0.04 sec (≥1 small square)
- Q wave depth ≥25% of the following R wave height
- Present in the territory of infarction (inferior: II, III, aVF; anterior: V1-V4; lateral: I, aVL, V5-V6)
- Q waves persist as a permanent scar marker weeks to years after MI
(See the "Weeks later" panel in Figure 2-2 above - Q wave persists with normalized ST and T)
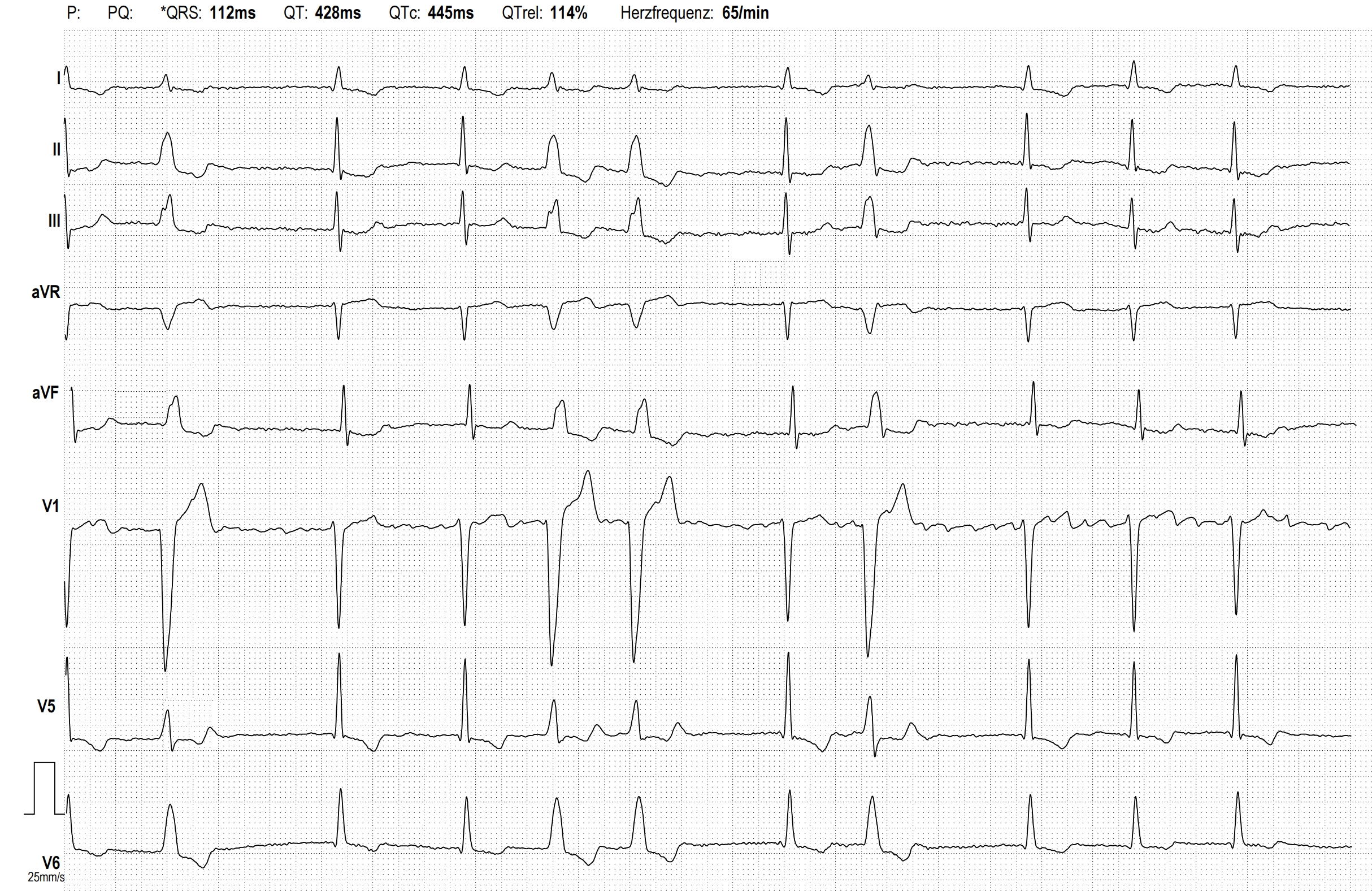
4. Atrial Fibrillation (AF)
Condition: Most common sustained arrhythmia; associated with hypertensive heart disease, valvular disease, heart failure, ischemic heart disease
ECG Features:
- Absent P waves - replaced by chaotic fibrillatory baseline (f-waves)
- Irregularly irregular ventricular rate
- Narrow QRS complexes (unless aberrant conduction/BBB)
- Ventricular rate 100-160 bpm if uncontrolled
5. Left Bundle Branch Block (LBBB)
Condition: Ischemic heart disease, cardiomyopathy, valvular disease, hypertension; new LBBB in chest pain = STEMI-equivalent
ECG Features:
- QRS duration ≥120 ms (≥3 small squares)
- V1: 'M'-shaped (RSR') or broad monophasic S wave
- V6: 'W' pattern - broad notched R wave
- Absent septal Q waves in lateral leads (I, aVL, V5-V6)
- Secondary ST/T wave changes opposite to main QRS deflection (discordance)

The LBBB signature pattern - V1 = 'M' shape, V6 = 'W' shape (opposite of RBBB):
(V1 'M' and V6 'W' are the hallmark - see the diagnostic diagram below for RBBB comparison)
6. Right Bundle Branch Block (RBBB)
Condition: Right heart strain (PE, pulmonary hypertension), ischemic heart disease, congenital heart disease; can be a normal variant
ECG Features:
- QRS duration ≥120 ms
- V1: RSR' ('rabbit ears') - broad 'M'-shaped complex
- V6: Wide slurred S wave ('W' pattern)
- T-wave inversion in V1-V3 (appropriate discordance)
- Anterior ST depression may accompany
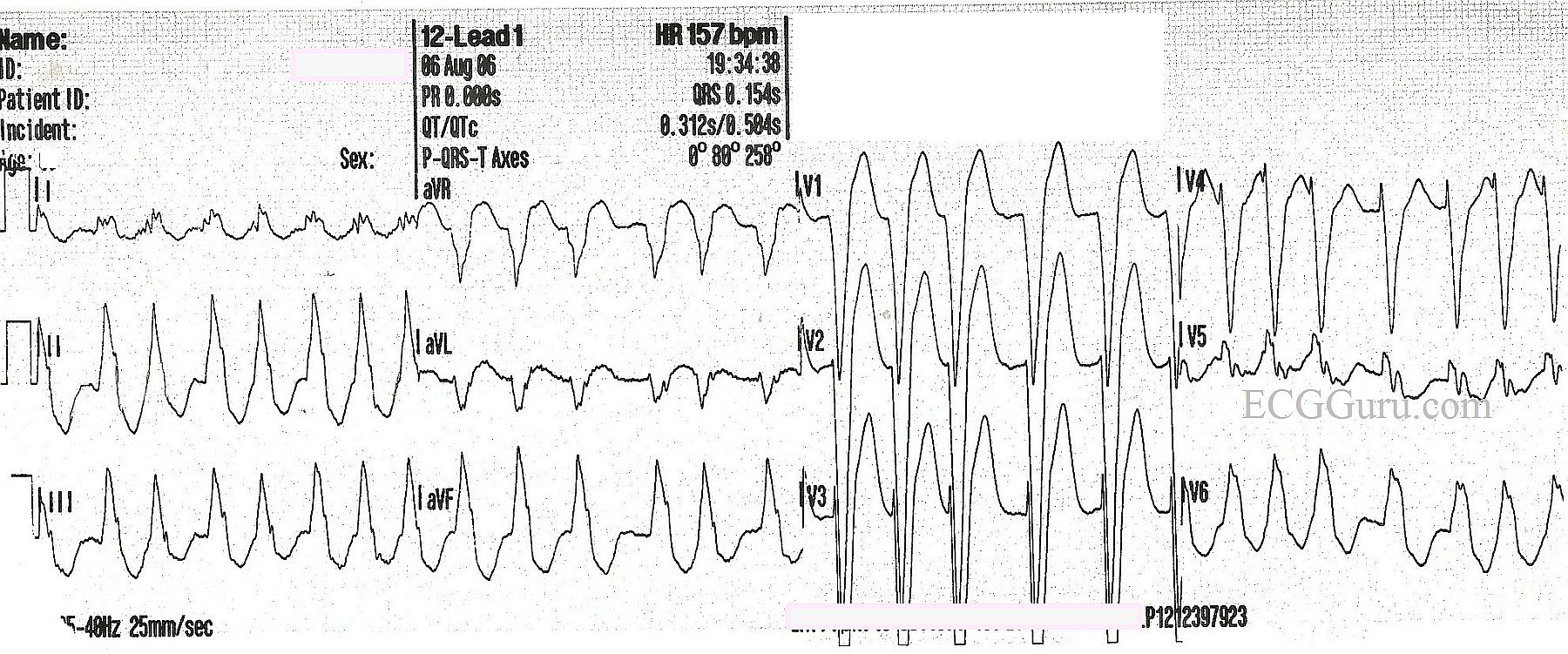
7. Ventricular Tachycardia (VT)
Condition: Ischemic cardiomyopathy, dilated cardiomyopathy, post-MI scar, channelopathies (e.g., Brugada, Long QT)
ECG Features:
- Rate >100 bpm (typically 120-250 bpm)
- Wide QRS complexes ≥120 ms with bizarre morphology
- AV dissociation (P waves independent of QRS) - pathognomonic
- Fusion beats and capture beats (if present, confirm VT diagnosis)
- Concordance in precordial leads (all positive or all negative V1-V6)
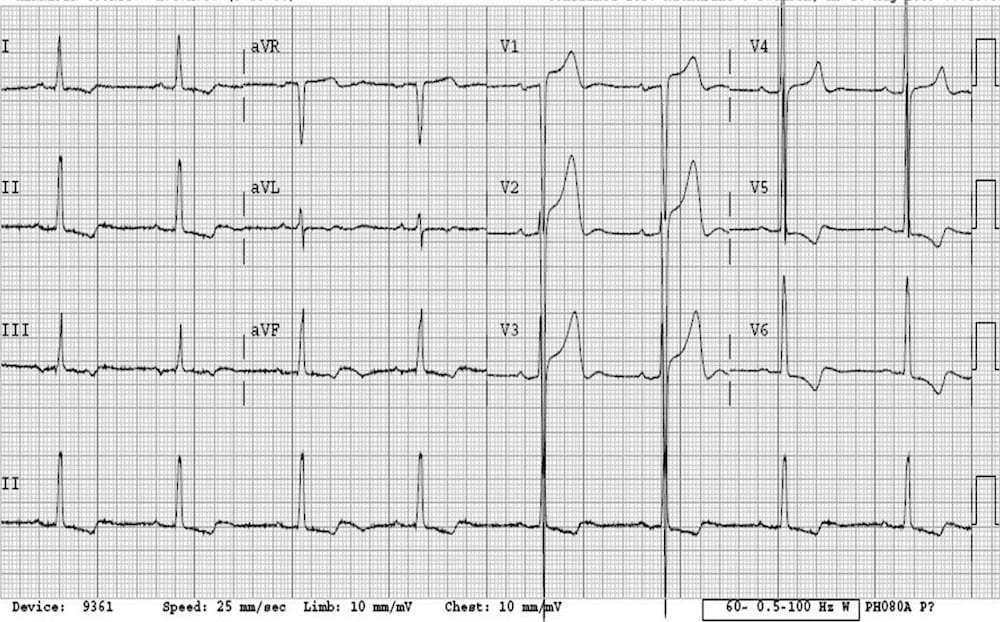
8. Left Ventricular Hypertrophy (LVH)
Condition: Hypertensive heart disease, aortic stenosis, hypertrophic cardiomyopathy
ECG Features:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- Tall R waves in lateral leads (I, aVL, V5-V6)
- Deep S waves in right precordial leads (V1-V2)
- Secondary ST depression and T-wave inversion in lateral leads ("strain pattern")
- Left axis deviation
9. Prolonged QT Interval
Condition: Congenital Long QT syndrome, drug-induced (antiarrhythmics, antipsychotics, antibiotics), electrolyte disturbances (hypokalemia, hypomagnesemia, hypocalcemia), myocarditis
ECG Features:
- Corrected QT interval (QTc) >440 ms in men, >460 ms in women
- Risk of Torsades de Pointes (polymorphic VT) when QTc >500 ms
- Broad, notched T waves; U waves may be prominent
- Measured from start of QRS to end of T wave
(Refer to the Atrial Fibrillation ECG above - note the measured QTc 445 ms shown at top of that tracing, just above borderline prolonged)
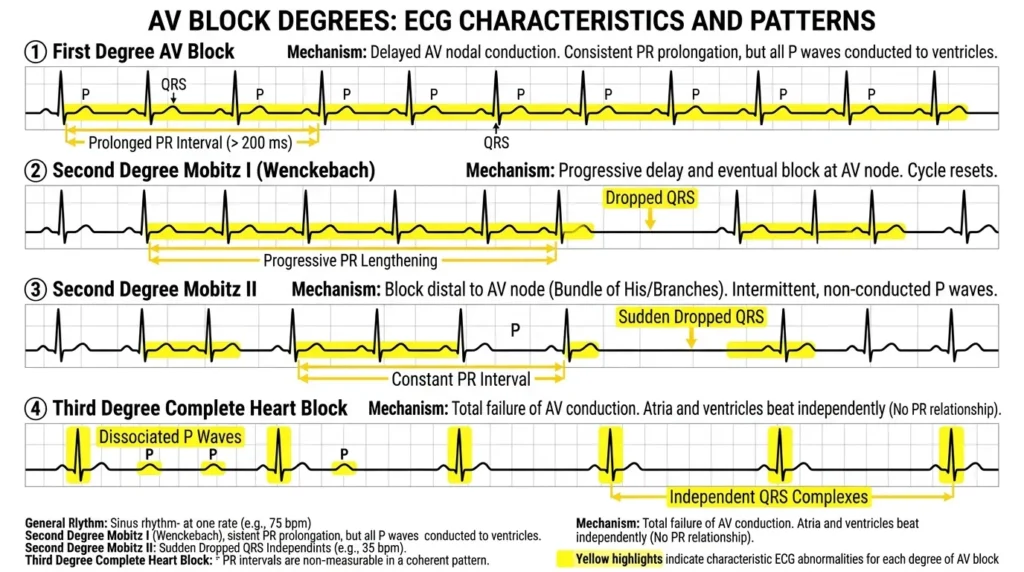
10. AV Blocks (First, Second, and Complete/Third Degree)
Condition: Ischemic heart disease (inferior MI often causes AV block via right coronary artery involvement), drugs (digoxin, beta-blockers, calcium channel blockers), infiltrative diseases (sarcoidosis, amyloidosis), Lyme disease
ECG Features by Degree:
| Degree | PR Interval | QRS Dropped? | Key Finding |
|---|---|---|---|
| 1st degree | >200 ms (>5 small squares) | No | Every P conducts, just slowly |
| 2nd degree Mobitz I (Wenckebach) | Progressively lengthens | Yes, cyclically | Progressive PR lengthening then dropped beat |
| 2nd degree Mobitz II | Constant | Yes, suddenly | Fixed PR then sudden dropped QRS - more dangerous |
| 3rd degree (complete) | No relationship | Every QRS is escape | AV dissociation - P and QRS completely independent |
Quick Reference Summary
| # | Finding | Key Feature | Associated Condition |
|---|---|---|---|
| 1 | ST elevation | ≥1-2 mm elevation in contiguous leads | STEMI, acute MI |
| 2 | ST depression / T inversion | Horizontal/downsloping depression | NSTEMI, ischemia |
| 3 | Pathological Q waves | ≥0.04 s wide, ≥25% of R | Prior MI (scar) |
| 4 | Atrial fibrillation | Irregular rhythm, no P waves | HTN, valvular, HF |
| 5 | LBBB | QRS ≥120 ms, V1='M', V6='W' | IHD, cardiomyopathy |
| 6 | RBBB | QRS ≥120 ms, V1 RSR', wide S in V6 | PE, IHD, normal variant |
| 7 | Ventricular tachycardia | Wide QRS >100 bpm, AV dissociation | Cardiomyopathy, post-MI |
| 8 | LVH | S(V1) + R(V5/V6) ≥35 mm, strain pattern | Hypertension, AS |
| 9 | Prolonged QT | QTc >440/460 ms | Drugs, electrolytes, congenital |
| 10 | AV block | PR prolonged / dropped QRS / AV dissociation | IHD, drugs, infiltrative |
Sources: Frameworks for Internal Medicine (Wolters Kluwer), Harrison's Principles of Internal Medicine 22E, LITFL ECG Library, ECGGuru
This is a shared conversation. Sign in to Orris to start your own chat.