ACUTE EPIGLOTTITIS
A Comprehensive 20-Mark Answer for RGUHS Examinations
DEFINITION
Acute epiglottitis (also called supraglottitis) is an acute bacterial infection causing inflammation of the epiglottis and surrounding supraglottic structures - including the aryepiglottic folds, arytenoids, and vallecula - with the potential for sudden, fatal airway obstruction. It is a life-threatening ENT emergency.
- Scott-Brown's Otorhinolaryngology, Vol 2, p. 1048 - "Epiglottitis is an acute infection of the supraglottis characterized by inflammation of the supraglottic structures. It is usually due to a bacterial infection and should be considered to be an emergency condition due to the potential rapid and fatal airway obstruction."
- Cummings Otolaryngology, p. 1958 - The inflammation involves the epiglottis, aryepiglottic folds and arytenoids with edema encroaching on the vallecula.
EPIDEMIOLOGY
| Parameter | Details |
|---|
| Incidence | 1-2 per 100,000 population |
| Peak age (classic) | 2-7 years (children) |
| Changing demographics | Now more common in adults (mean age 40 years, male) |
| Seasonal variation | Increased prevalence in winter |
| Pre-vaccine era | Predominantly children aged 2-4 years |
| Post-vaccine era | Adults more commonly affected; Hib <20% of adult cases |
| Mortality | Up to 3%; majority of deaths now in adults |
- Scott-Brown's, Vol 2: "In a retrospective dataset study from the United States, Shah et al. found that the typical patient admitted with epiglottitis is a 40-year-old male and that the majority of mortalities from epiglottitis were in the adult population."
- Dhingra / Hazarika: Historically commonest in children aged 2-7 years with peak incidence in winter months.
ETIOLOGY AND MICROBIOLOGY
Primary Organism
- Haemophilus influenzae type b (Hib) - historically accounted for >90% of all cases; still the commonest in unvaccinated children
Post-Hib Vaccine Era Organisms
| Category | Organisms |
|---|
| Bacterial (common) | Beta-haemolytic Streptococcus, Streptococcus pneumoniae, Streptococcus milleri, Staphylococcus aureus (including MRSA), Neisseria meningitidis |
| Bacterial (less common) | Escherichia coli, Klebsiella pneumoniae, Haemophilus parainfluenzae |
| Immunocompromised hosts | Candida albicans, Pseudomonas aeruginosa, Herpes simplex type 1, Varicella zoster, Parainfluenza virus |
Non-Infectious Causes (Rare)
-
Thermal injury (hot liquids, steam inhalation)
-
Caustic ingestions
-
Allergic reactions / angioedema
-
Foreign body injury
-
Lymphoproliferative disorders
-
Recent: e-cigarette (vaping) induced epiglottitis - [Khorrami et al., 2023, PMID 37670242]
-
Scott-Brown's, Vol 2: "Fewer than 20% of cases of adult epiglottitis are due to Haemophilus influenzae. Candida albicans is an important cause to consider in immunocompromised patients."
-
Rosen's Emergency Medicine: "Additional causes include other H. influenzae types (A, F, nontypeable), streptococci, S. aureus (including methicillin-resistant strains), and Neisseria meningitidis."
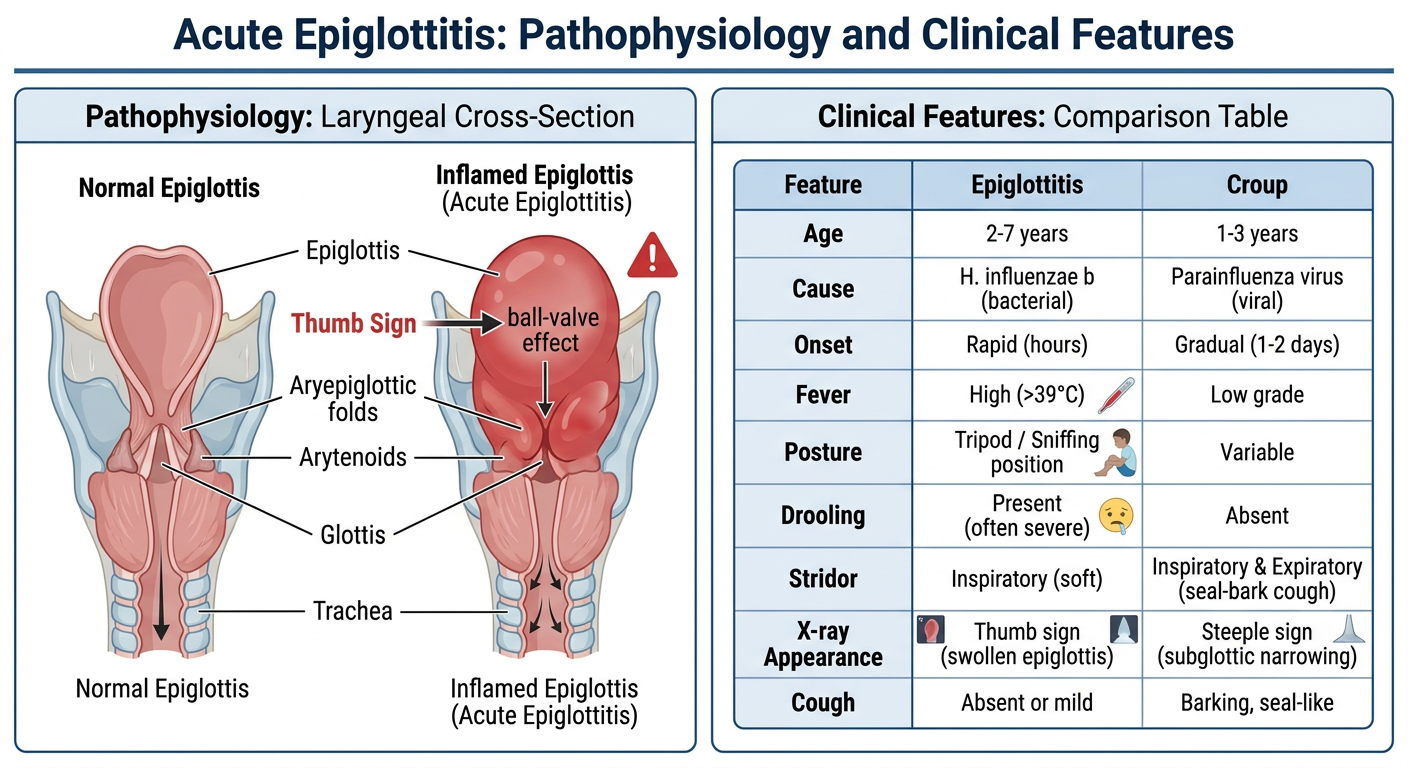
PATHOPHYSIOLOGY
The Hib organism (or other pathogen) gains entry via the nasopharynx and invades the loose areolar tissue of the supraglottis. The rich lymphatics and loose submucosal tissue of the epiglottis allow rapid edema formation.
Mechanism of airway obstruction (as described in Rosen's):
- Bacterial invasion → inflammatory edema of epiglottis and aryepiglottic folds
- Swollen structures protrude downward and over the glottic opening
- Supraglottic swelling reduces upper airway caliber → turbulent airflow → inspiratory stridor
- The edematous epiglottis acts as a ball valve - obstructing airflow during inspiration while permitting exhalation
- Progressive swelling → complete airway obstruction → asphyxiation
Diagram 1: Pathophysiology, anatomical changes, and comparison with croup
CLINICAL FEATURES
The "4 D's" of Epiglottitis (Classic Triad)
| Sign/Symptom | Notes |
|---|
| Drooling | Due to inability to swallow pooled saliva |
| Dysphagia + Dysphonia | Odynophagia; muffled "hot potato" voice |
| Distress (respiratory) | Tachypnoea, stridor, retractions |
In Children (Classic Presentation)
- Rapid onset - hours (unlike croup, which has 1-2 day prodrome)
- High fever >39°C, toxic appearance
- Tripod/sniffing position: child sits upright, neck extended, jaw jutted forward, arms propped on knees - to maximize airway patency
- Drooling (cannot swallow), inspiratory stridor
- Absence of cough (differentiating from croup)
- Pale, anxious, tachycardic
In Adults (Often Subtle)
-
Main complaint: sore throat out of proportion to pharyngeal findings
-
Odynophagia, anterior neck tenderness
-
Dyspnoea and drooling may or may not be present (larger airway caliber)
-
Features of upper airway obstruction may be absent until late
-
Significant comorbidities (diabetes, hypertension, cardiac disease) worsen prognosis
-
Scott-Brown's, Vol 2: "In adults, the main complaint is of a painful throat with associated odynophagia. As the calibre of the airway is larger in adults than children, features of upper airway obstruction may not always be present."
-
Rosen's Emergency Medicine: "Toxicity, altered mental status, dyspnoea, stridor, retractions, and fever are common initial symptoms."
DIAGNOSIS
CRITICAL RULE: DO NOT EXAMINE THE THROAT
Attempting pharyngeal examination or using a tongue depressor in a suspected epiglottitis patient can precipitate acute complete airway obstruction. This is an absolute contraindication.
Investigations (after securing airway)
1. Lateral Soft Tissue X-Ray of Neck
- Best diagnostic radiograph
- Shows "Thumb Sign" / "thumbprint sign" - the edematous epiglottis appears as a rounded, thumb-like soft tissue density (normally thin and finger-nail shaped)
- Thickened aryepiglottic folds
- Hypopharyngeal distension
- Should not delay airway management
Fig. 1: Lateral neck X-ray - "Thumb Sign" of acute epiglottitis (arrowed). Source: Scott-Brown's Otorhinolaryngology, Vol 2, Fig 29.4
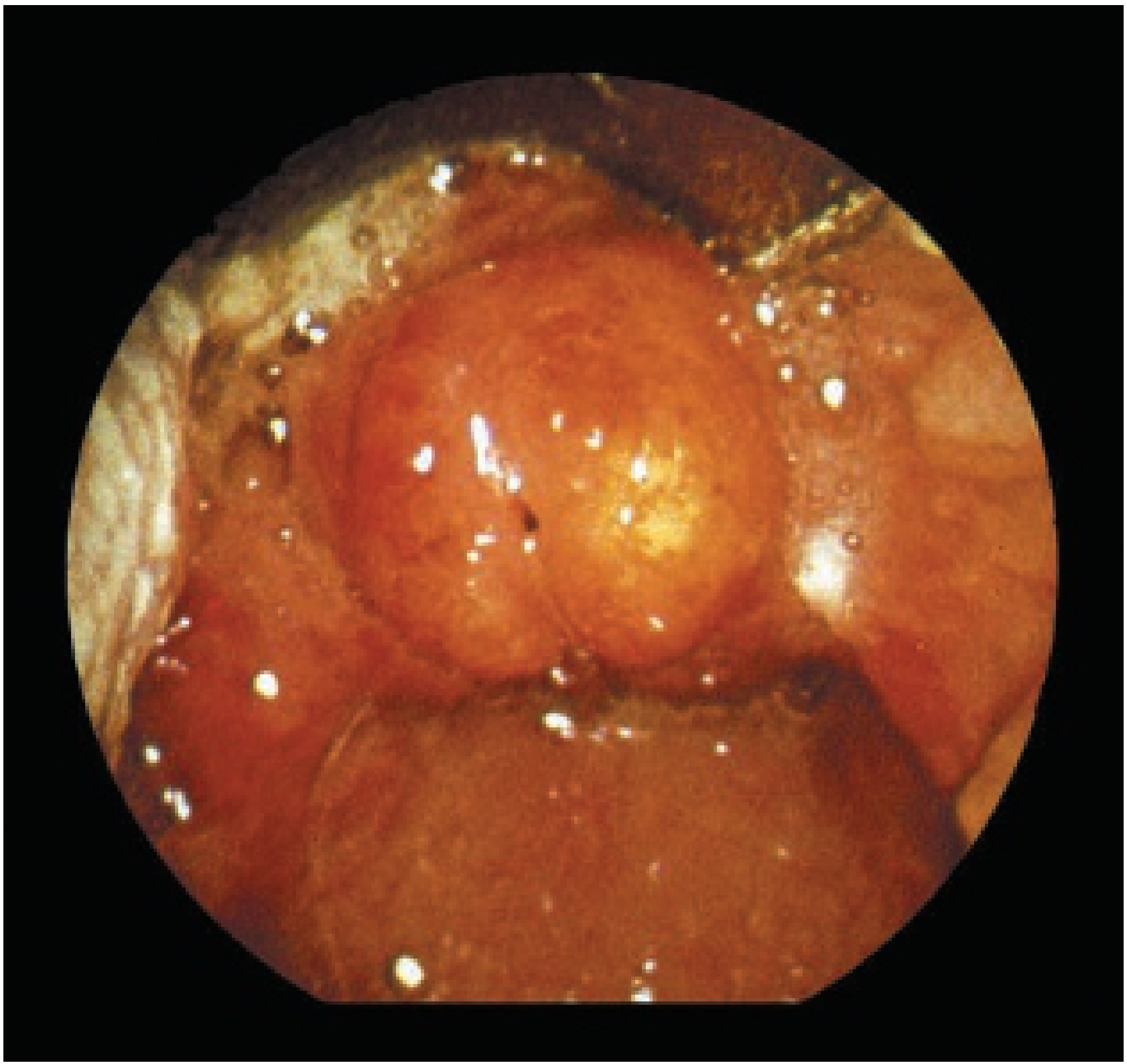
2. Trans-nasal Fibre-optic Laryngoscopy (TNFL)
- Gold standard for confirmation
- In adults with atypical presentation, can be done to confirm diagnosis
- Reveals: erythematous, congested, cherry-red, swollen epiglottis with supraglottic edema
- NOT to be done without airway backup in children
Fig. 2: Endoscopic appearance - cherry-red, edematous epiglottis. Source: Scott-Brown's Otorhinolaryngology, Vol 2, Fig 29.3
3. Microbiological
- Nasopharyngeal swabs, laryngeal swabs, blood cultures - only after securing airway
- Hib antigen detection in concentrated urine specimens (useful in partially treated cases)
- Blood culture positive in ~25% of cases
4. CT Scan of Neck
- Indicated only if associated epiglottic abscess is suspected
- Epiglottic abscess occurs in 4-27% of cases, mostly on lingual surface of epiglottis
5. Lab Tests
-
CBC: leukocytosis with neutrophilia
-
ESR, CRP elevated
-
Blood cultures
-
Cummings Otolaryngology: "On radiography, these normally well-defined thin structures become edematous, enlarged, and unsharp, resulting in a rounded thumb-like density in place of the normal epiglottis."
DIFFERENTIAL DIAGNOSIS
| Condition | Key Differentiating Features |
|---|
| Viral Croup (LTB) | 1-3 years, seal-bark cough, steeple sign on X-ray, gradual onset |
| Bacterial Tracheitis | "Pseudomembranous croup", toxic, steeple sign + subglottic narrowing |
| Retropharyngeal Abscess | Neck stiff, comfortable supine with neck extended, bulge on posterior pharyngeal wall |
| Peritonsillar Abscess | Muffled voice, trismus, peritonsillar bulge, uvula displaced |
| Foreign Body | Sudden onset, no fever, witnessed choking |
| Angioedema | No fever, history of allergy, responds to adrenaline |
| Diphtheria | Pseudomembrane in throat, bull-neck appearance, serosanguinous discharge |
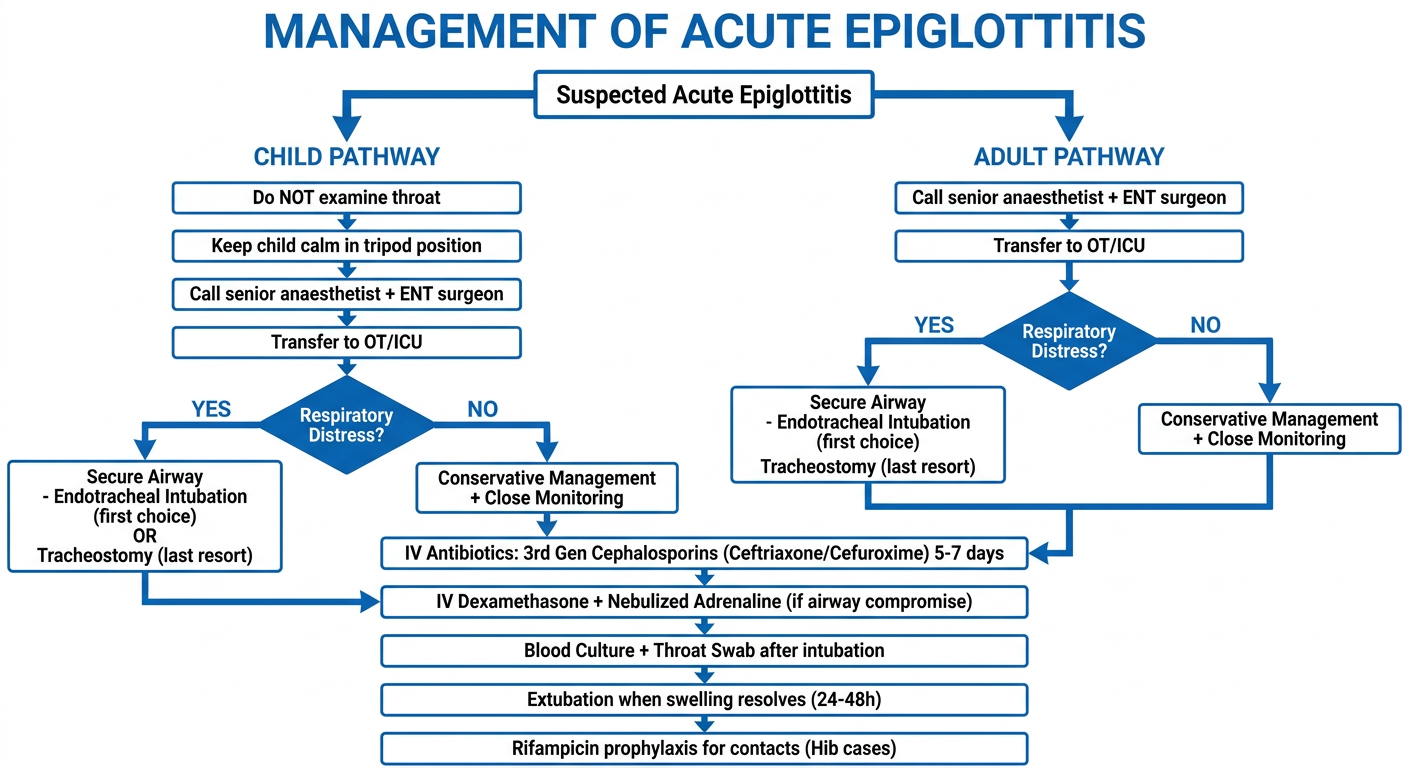
MANAGEMENT
Principles (RGUHS focus areas)
The management is a multidisciplinary team (MDT) approach involving ENT surgeon, anaesthetist, intensivist/paediatrician.
Diagram 2: Management flowchart for Acute Epiglottitis
Step-by-Step Management
Step 1: Immediate Emergency Measures
- Keep child calm and comfortable - do NOT agitate (agitation can precipitate obstruction)
- Allow child to maintain own position (tripod)
- Do NOT attempt direct laryngoscopy or throat examination
- Administer humidified oxygen in a non-threatening manner (flow-by)
- Do NOT take blood or X-rays if child appears severely distressed
- Call senior anaesthetist + ENT surgeon simultaneously
- Transfer to Operating Theatre (OT) or PICU immediately
Step 2: Airway Securing
- Inhalational anaesthesia (halothane/sevoflurane) used to induce anaesthesia while maintaining spontaneous ventilation
- Endotracheal intubation - first-line; usually requires 1-2 sizes smaller tube than expected
- If intubation fails: rigid bronchoscopy to pass tube / tracheostomy
- Tracheostomy - only in dire emergencies when intubation absolutely not possible (used in ~3% of cases); required only in very urgent cases where patient presents late
- Typical intubation duration: 24-48 hours until swelling resolves
Step 3: Antibiotic Therapy
| Antibiotic | Dose/Route | Comments |
|---|
| Ceftriaxone (first-line) | 80-100 mg/kg/day IV | 3rd gen cephalosporin; covers >50% ampicillin-resistant Hib |
| Cefuroxime | IV | Alternative 2nd gen |
| Chloramphenicol | IV | Used if cephalosporin allergy |
| Clindamycin | IV | Alternative for allergy |
| + Metronidazole | IV | Add if anaerobic organisms suspected |
| Duration | 5-7 days | Transition to oral when able to swallow |
- Scott-Brown's, Vol 2: "Ampicillin resistance due to beta-lactamase production is now over 50% in Haemophilus influenzae, so empirical treatment with third-generation cephalosporins for 5-7 days is advised."
Step 4: Corticosteroids
- IV Dexamethasone 0.15-0.6 mg/kg - reduces supraglottic edema, may decrease need for intubation
- Nebulized adrenaline (1:1000, 0.5 ml/kg up to 5 ml) - for acute airway compromise
- Note: evidence base is limited (extrapolated largely from croup studies)
- Scott-Brown's, Vol 2: "A short course of steroids may help to decrease the airway inflammation, possibly decreasing the need for intubation. However careful consideration should be given to this rather than using corticosteroids as a matter of routine, as the evidence on the role of corticosteroids is lacking."
Step 5: Supportive Care
- IV fluids (NPO initially)
- Humidified oxygen
- Monitoring: pulse oximetry, ECG, BP
- ICU/HDU nursing with regular TNFL assessment
Step 6: Post-Extubation Care
- Monitor for 24-48 hours after extubation
- Extubate when fever resolves, systemic symptoms improve, and TNFL shows resolving supraglottitis
- Transition to oral antibiotics
- Discharge with follow-up
Step 7: Prophylaxis (Hib cases)
- Rifampicin prophylaxis for:
- Index case (to eradicate carrier state)
- All household contacts
- School contacts
- Dose: 20 mg/kg/day for 4 days (max 600 mg/day)
- Scott-Brown's, Vol 2: "Since the introduction of Hib immunization, rifampicin prophylaxis has been recommended to eradicate the carrier state for the index case as well as household and school contacts."
CROUP vs EPIGLOTTITIS: COMPARATIVE TABLE
| Feature | Croup (LTB) | Acute Epiglottitis |
|---|
| Age | 1-3 years | 2-7 years (children); adults |
| Causative agent | Parainfluenza virus type 1 | Hib (children); Mixed in adults |
| Onset | Gradual, 1-2 day prodrome | Rapid, within hours |
| Fever | Low grade (<38.5°C) | High (>39°C) |
| Cough | Barking/seal-like cough | Absent |
| Voice | Hoarse | Muffled "hot potato" |
| Stridor | Inspiratory ± biphasic | Inspiratory |
| Drooling | Absent | Present |
| Posture | Normal | Tripod/sniffing position |
| Toxicity | Not toxic | Toxic appearance |
| X-ray | Steeple sign (subglottic) | Thumb sign (supraglottic) |
| Throat exam | Safe | Contraindicated |
| Treatment | Steroids + neb. adrenaline | Intubation + IV antibiotics |
(Based on Scott-Brown's Vol 1, Table 34.4)
COMPLICATIONS
| Complication | Notes |
|---|
| Acute airway obstruction | Main cause of death; can be sudden |
| Epiglottic abscess | 4-27% of cases; lingual surface; requires surgical drainage |
| Septicaemia/bacteraemia | H. influenzae bacteraemia in up to 80% of childhood cases |
| Meningitis | Major concern with Hib |
| Pulmonary oedema | Post-obstructive pulmonary oedema |
| Pneumonia, Septic arthritis, Osteomyelitis | Metastatic Hib spread |
| Death | ~3% mortality; mostly in adults |
PREVENTION
- Hib Conjugate Vaccine - introduced in UK in 1992, India in Universal Immunisation Programme
- Given at 6, 10, 14 weeks (as pentavalent vaccine - DPT+HepB+Hib)
- Has reduced childhood epiglottitis by >95%
- Rifampicin prophylaxis for contacts (as above)
- Scott-Brown's, Vol 2: "Despite the declining incidence of this disease and the changing bacteriology, there has been no change in its clinical presentation over time. It is critically important that reduced clinical experience is not accompanied by a sharp rise in mortality for affected children."
RECENT ADVANCES (2021-2026)
-
Changing Microbiology: COVID-19-associated epiglottitis is now documented. A 2023 systematic review (
Meng X et al., PMID 36946336) found that SARS-CoV-2 can directly cause acute epiglottitis, distinct from secondary bacterial superinfection.
-
E-cigarette (Vaping) Induced Epiglottitis: Thermal and chemical injury from e-cigarette vapour is an emerging non-infectious cause (
Khorrami et al., 2023, PMID 37670242). The heated aerosol induces local inflammatory edema of the supraglottis.
-
Airway Management Meta-Analysis: A 2024 systematic review and meta-analysis (
Booth et al., BJA Open, PMID 38230383) found that:
- Most adult epiglottitis can be managed without intubation (conservative management in ~75%)
- Predictors of airway intervention: stridor at rest, drooling, respiratory distress, and epiglottis-to-C3 vertebra ratio on lateral X-ray
- Video laryngoscopy preferred over direct laryngoscopy for intubation
-
Non-Infectious Epiglottitis in Adults: A 2025 systematic review (
Safia et al., PLoS One, PMID 39928631) found that age does not reliably predict outcomes in non-infectious (thermal/chemical/allergic) epiglottitis - management decisions should be based on clinical signs alone.
-
Risk Stratification Scores: The "KLASS score" (TNFL-based scoring) has been proposed in several centers to stratify adult epiglottitis patients into conservative vs. intubation groups, reducing unnecessary ICU admissions.
-
Pediatric Update (2025): A 2025 review (
Shlomovich et al., Pediatr Rev, PMID 40588280) emphasized that in the post-Hib era, non-Hib epiglottitis in children often has a more insidious course, making early recognition more difficult.
-
MRSA Epiglottitis: Methicillin-resistant S. aureus (MRSA) is an increasingly recognized cause; vancomycin or linezolid should be considered in ICU patients with no response to cephalosporins.
-
Point-of-Care Ultrasound (POCUS): Emerging evidence supports ultrasound visualization of the epiglottis via trans-tracheal approach as a rapid bedside tool - epiglottis thickness >8 mm suggests epiglottitis.
SUMMARY TABLE: KEY POINTS FOR EXAM
| Aspect | Key Fact |
|---|
| Most common cause | Hib (pre-vaccine); post-vaccine: adults, mixed organisms |
| Classic age | 2-7 years |
| Classic triad | Drooling, Dysphagia, Distress (4 D's + Dysphonia) |
| Pathognomonic posture | Tripod/sniffing position |
| X-ray finding | Thumb sign on lateral neck X-ray |
| Contraindicated | Throat examination/tongue depressor |
| First-line antibiotic | IV Ceftriaxone (3rd gen cephalosporin) x 5-7 days |
| Airway management | Inhalational induction → ET intubation (OT setting) |
| Tracheostomy | Only when intubation fails (~3%) |
| Prophylaxis | Rifampicin for household/school contacts |
| Steroid role | IV Dexamethasone (evidence limited but used) |
| Vaccine | Hib conjugate (pentavalent) - given at 6, 10, 14 wks |
| Complication | Epiglottic abscess 4-27%, septicaemia, meningitis |
| Intubation duration | 24-48 hours typically |
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed, Vol 1 & Vol 2 - Epiglottitis (Supraglottitis), pp. 1048-1049; Acute Epiglottitis (Paediatric chapter); Medico-legal aspects, p. 373
- Cummings Otolaryngology Head & Neck Surgery, 7th Ed - Imaging of Epiglottitis, p. 1958 (Radiological diagnosis, thumb sign, aryepiglottic folds)
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 9th Ed - Epiglottitis, pp. 3717-3745 (Full emergency management)
- Dhingra PL - Diseases of Ear, Nose and Throat - Acute Epiglottitis (Supraglottitis)
- Hazarika P - Textbook of Ear, Nose and Throat and Head & Neck Surgery - Acute Laryngeal Infections
- Stell and Maran's Head and Neck Surgery - Epiglottitis, Airway emergencies
- Zakir Hussain - ENT - Acute Epiglottitis, differentials, management
- Meng X, Han C, Wang Y. Acute epiglottitis caused by COVID-19: A systematic review. Biomol Biomed. 2023.
- Booth AWG et al. Airway management of adult epiglottitis: a systematic review and meta-analysis. BJA Open. 2024.
- Safia A et al. Does patients' age predict their clinical outcomes following non-infectious epiglottitis? PLoS One. 2025.
- Shlomovich M, Hyatt S, Cassel-Choudhury GN. Croup and Epiglottitis. Pediatr Rev. 2025.
- Bridwell RE, Koyfman A, Long B. High risk and low prevalence diseases: Adult epiglottitis. Am J Emerg Med. 2022.
RGUHS Exam Tip: For 20-mark questions on epiglottitis, the expected structure is: Definition → Etiology → Pathophysiology → Clinical Features → Diagnosis (including thumb sign X-ray) → Differential diagnosis (croup table) → Management (airway priority, MDT, antibiotics, steroids, prophylaxis) → Complications → Recent advances → Prevention. Always emphasize "do NOT examine the throat" and "tripod position" - these are commonly asked single-liner questions too.