Anemia in pregnancy
Reading File
Finding Sources
Searching PubMed
"anemia" AND "pregnancy"
Searching the Web
anemia in pregnancy causes diagnosis management guidelines 2024
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Anemia in Pregnancy
Definition & Diagnosis
Anemia in pregnancy is defined by hemoglobin thresholds that differ from the non-pregnant state due to physiologic hemodilution:
| Authority | Threshold |
|---|---|
| WHO | Hb < 11 g/dL (any trimester) |
| CDC | Hb < 5th percentile for gestational age |
| Practical | Hb < 11 g/dL (1st & 3rd trimester); < 10.5 g/dL (2nd trimester) |
Severity classification:
- Mild: 10–10.9 g/dL
- Moderate: 7–9.9 g/dL
- Severe: < 7 g/dL (transfusion threshold typically < 7 g/dL antepartum; < 8 g/dL postpartum)
Physiologic Changes Underlying "Dilutional Anemia"
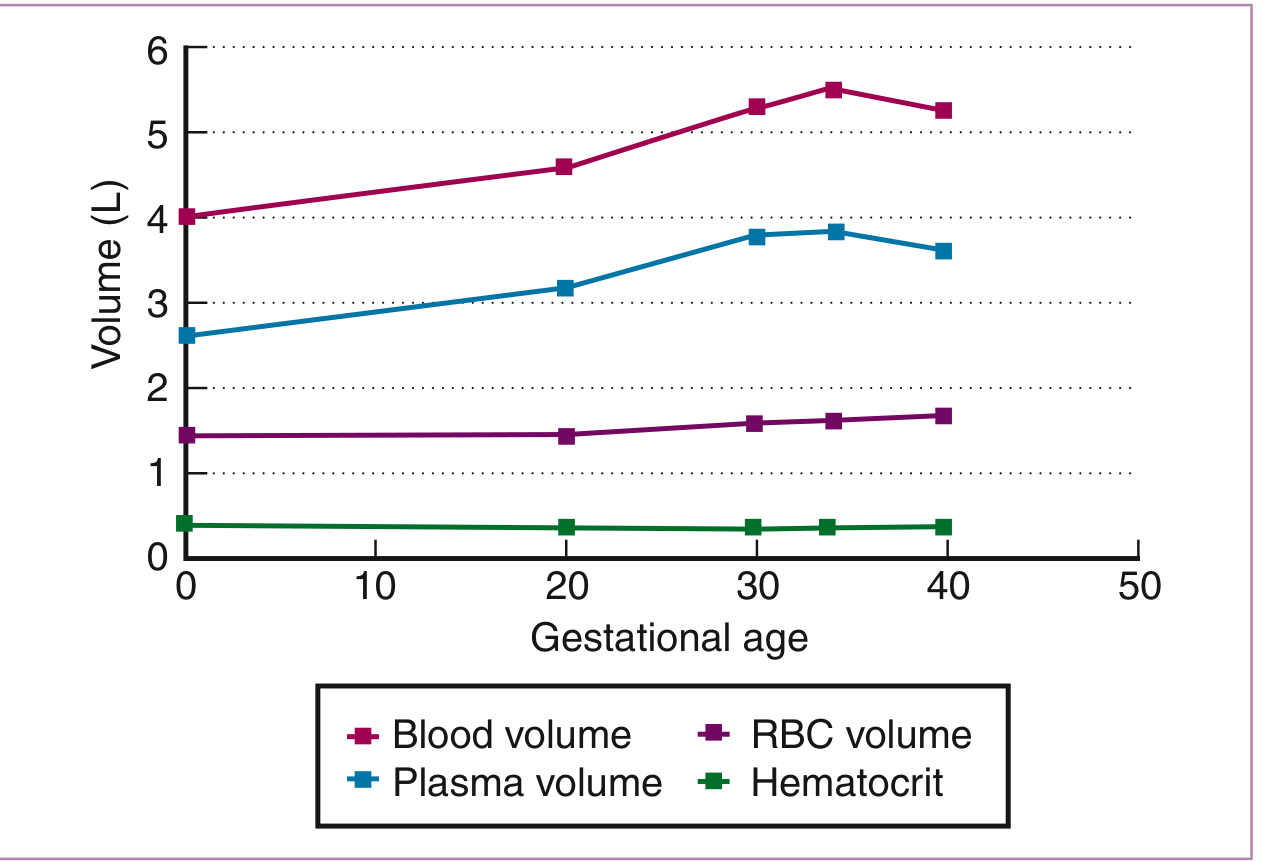
Figure: Blood volume, plasma volume, RBC volume, and hematocrit changes across gestational age. Plasma volume rises disproportionately, driving hemodilution that peaks at 28–34 weeks. — Creasy & Resnik's Maternal-Fetal Medicine
- Blood volume increases ~40–50% (maximum at ~34 weeks)
- Plasma volume increases ~47%
- RBC mass increases only ~17% (reaches maximum at term)
- This disparity causes physiologic (dilutional) anemia — normocytic, with Hb > 11 g/dL in uncomplicated pregnancy; MCV and MCHC remain unchanged
- Hb nadir typically at 26–28 weeks
- Paradoxically, Hb 13–15 g/dL in pregnancy may reflect inadequate plasma expansion and is associated with low birthweight and preterm birth
Causes of Anemia in Pregnancy
1. Iron Deficiency Anemia (IDA) — Most Common
- Prevalence: iron deficiency in ~18% of US pregnancies; frank IDA in ~5%
- Total iron requirement for a singleton pregnancy: ~1130 mg (range 580–1340 mg)
| Iron Requirement | Average (mg) |
|---|---|
| External iron loss | 170 |
| RBC mass expansion | 450 |
| Fetal iron | 270 |
| Placenta & cord | 90 |
| Blood loss at delivery | 150 |
| Total | ~1130 |
- Pregnancy demands exceed the iron saved by 9 months of amenorrhea
- ~2/3 of healthy women have minimal bone marrow iron stores before pregnancy
- Iron deficiency progresses through 3 stages:
- Prelatent — reduced marrow stores; ↓ serum ferritin; Hb normal
- Latent — ↓ serum iron, ↑ TIBC, ↓ % saturation; Hb still normal
- Overt IDA — ↓ Hb, ↓ MCV; microcytic hypochromic picture
Diagnosis: Ferritin is the most sensitive/specific marker for IDA in pregnancy — cutoff < 30 ng/mL (sensitivity 92%, specificity 98%). Ferritin < 12 µg/L = severe depletion. Note that MCV, TIBC, and transferrin are less reliable because normal pregnancy changes affect them. Ferritin is an acute-phase reactant and may be falsely normal with inflammation; measure in non-febrile patients.
2. Folate Deficiency — Second Most Common
- Folate requirements increase 5–10 fold in pregnancy
- Risk factors: multiple gestation, short interpregnancy intervals, hyperemesis, malabsorption, alcoholism, antiepileptic drugs (methotrexate, phenytoin, trimethoprim), diet lacking green leafy vegetables
- Causes megaloblastic anemia; also linked to neural tube defects, placental abruption, preterm birth, preeclampsia
- Distinguish from B12 deficiency: serum folate normalizes rapidly with diet; RBC folate better reflects stores; check methylmalonic acid (MMA) if B12 suspected
3. Vitamin B12 Deficiency
- Less common; seen with strict vegetarian/vegan diets, pernicious anemia, gastric surgery
- Megaloblastic picture; elevated MMA and homocysteine
- Anti-intrinsic factor antibodies specific for pernicious anemia (but only 60% sensitive)
4. Hemoglobinopathies
Sickle Cell Disease (SCD):
- Sixfold increased risk of maternal death vs controls
- Complications: more frequent vaso-occlusive crises, VTE (1.7–10× more frequent), preeclampsia, preterm labor, PROM, cesarean delivery, placental infarction
- Fetal effects: SGA, low birthweight, increased perinatal mortality
- Treatment: supportive; hydroxyurea contraindicated (teratogenic); NSAIDs avoided after 30 weeks; regional anesthesia preferred over GA; supplemental iron controversial (risk of iron overload); exchange transfusion may be needed for severe crises
- Prophylactic transfusion: controversial in SCD
Thalassemia:
- Alpha-thalassemia trait: microcytosis, normal/high RBC count, normal ferritin — distinguish from IDA
- Beta-thalassemia major: requires transfusion support; high-risk pregnancy
5. Aplastic Anemia
- Pancytopenia + hypocellular bone marrow; immune-mediated attack on hematopoietic stem cells
- Pregnancy-associated aplastic anemia may remit after delivery, but diagnosis is uncertain
- Goals: Hb > 8 g/dL, platelets > 20 × 10⁹/L; bone marrow transplant not feasible in pregnancy; immunosuppression (antithymocyte globulin, cyclosporine) used
- Complications: postpartum hemorrhage, abruption, preeclampsia, preterm delivery, fetal demise (especially with severe thrombocytopenia)
- Requires multidisciplinary team (MFM + hematology + anesthesia)
6. Other Causes
- Hemolytic anemias: autoimmune (direct Coombs +), microangiopathic (TTP/HUS/HELLP), PNH, G6PD deficiency
- Anemia of chronic disease/inflammation
- Renal anemia
Laboratory Evaluation
Reference ranges by trimester (Creasy & Resnik):
| Test | 1st Trimester | 2nd Trimester | 3rd Trimester |
|---|---|---|---|
| RBC count (×10¹²/L) | 3.42–4.55 | 2.81–4.49 | 2.72–4.43 |
| MCV (µm³) | 81–96 | 82–97 | 81–99 |
| MCHC (g/dL) | 32–35 | 32–35 | 32–35 |
| Reticulocyte count | 0.5–1.5% | — | — |
| LDH (U/L) | 78–433 | 80–447 | 82–524 |
| Serum haptoglobin (mg/dL) | 30–200 | — | — |
Diagnostic approach by MCV:
- Microcytic (↓ MCV): IDA, thalassemia, sideroblastic anemia → check ferritin, serum iron, TIBC, Hb HPLC
- Normocytic: dilutional anemia, early IDA, hemolytic anemia, aplastic anemia, anemia of chronic disease
- Macrocytic (↑ MCV): folate or B12 deficiency, hypothyroidism → check serum/RBC folate, B12, MMA
Key point: Iron studies (serum iron, ferritin) must be drawn 24–48 hours after stopping iron supplementation to avoid false results.
Maternal and Fetal Consequences
| Severity | Maternal Risks | Fetal/Neonatal Risks |
|---|---|---|
| Mild-moderate | Fatigue, reduced work capacity, PPH risk | Low birthweight, preterm birth |
| Severe (< 7 g/dL) | PPH, preeclampsia, maternal mortality, transfusion | IUGR, fetal hypoxia, PROM, gestational hypertension, oligohydramnios, perinatal mortality |
Management
Iron Deficiency Anemia
Oral iron:
- First-line for mild IDA (Hb 9–10.5 g/dL): non-enteric-coated ferrous iron (ferrous sulfate, fumarate, or gluconate)
- ACOG/WHO recommend ≥ 30 mg elemental ferrous iron daily for all pregnant women
- Single daily dose is as effective as multiple doses and reduces GI side effects (nausea, constipation, GERD — already heightened in pregnancy)
- Intermittent dosing (2–3×/week) provides similar maternal and fetal benefits with fewer side effects — 2024 Cochrane meta-analysis PMID 39145520 supports this approach
IV iron:
- Not used in the first trimester
- Treatment of choice for:
- All IDA in the third trimester
- Severe IDA (Hb < 9 g/dL) in the second trimester
- Oral iron intolerance or non-compliance
- Malabsorption syndromes
- Options: ferric carboxymaltose, iron sucrose, low-molecular-weight iron dextran
- Recombinant erythropoietin: limited role; a 2025 systematic review (PMID 39087437) found it is sometimes used for IDA unresponsive to iron alone but evidence is limited
Blood transfusion:
- Reserved for Hb < 7 g/dL antepartum or Hb < 8 g/dL postpartum, or hemodynamic compromise
Folate Deficiency
- All women: 0.4 mg folic acid daily preconception and throughout pregnancy
- Known folate deficiency: 1.0 mg/day
- High-risk (prior NTD pregnancy): 4 mg/day starting 1 month preconception through 12 weeks GA, continued throughout pregnancy
Vitamin B12 Deficiency
- Oral or IM cyanocobalamin; identify and treat underlying cause
Sickle Cell Disease
- Multidisciplinary care; avoid hydroxyurea; prophylactic antibiotics for asplenia; folic acid supplementation; pain management (avoid NSAIDs > 30 weeks); exchange transfusion for severe crises; regional anesthesia
Screening Recommendations
- First prenatal visit: CBC (all women)
- 26–28 weeks: repeat CBC (screen for late IDA and dilutional anemia)
- Ferritin should be checked if Hb < 11 g/dL or risk factors present
- Hemoglobin electrophoresis (HPLC): screen for hemoglobinopathies in at-risk populations
Recent Evidence (2024–2026)
| PMID | Study | Finding |
|---|---|---|
| 39145520 | Cochrane Meta-Analysis 2024 | Daily oral iron supplementation during pregnancy reduces IDA at term; intermittent dosing comparable with fewer side effects |
| 39087437 | Systematic Review 2025 | Recombinant EPO may have a role in IDA refractory to iron; evidence still limited |
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Goldman-Cecil Medicine; Rosen's Emergency Medicine; ACOG Practice Bulletin; Cochrane Database 2024.
This is a shared conversation. Sign in to Orris to start your own chat.