How to approach pancytopenia , and proceed with history and physical exams to make differential diagnosis
Reading File
How to approach pancytopenia , and proceed with history and physical exams to make differential diagnosis..especially in wards , and also for my mrcp and fcps part 2 exam
Finding Sources
Finding Sources
Searching the Web
pancytopenia approach history physical examination differential diagnosis MRCP FCPS
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11399640
Reading File
Loading Image
Reading File
Reading File
Loading Image
Searching PubMed
pancytopenia approach diagnosis evaluation
I now have comprehensive material from Harrison's, Frameworks for Internal Medicine, Family Medicine textbook, and current literature. Let me compile the complete, exam-level answer.
Approach to Pancytopenia - Ward & Exam (MRCP/FCPS Part 2)
Definition
Pancytopenia = simultaneous reduction in all three cell lines:
- Haemoglobin < 13 g/dL (men) / < 12 g/dL (women)
- WBC < 4,000/µL (or ANC < 1,500/µL)
- Platelets < 150,000/µL
The Pathophysiological Framework (Memorise This First)
This is the single most important conceptual map for MRCP/FCPS:
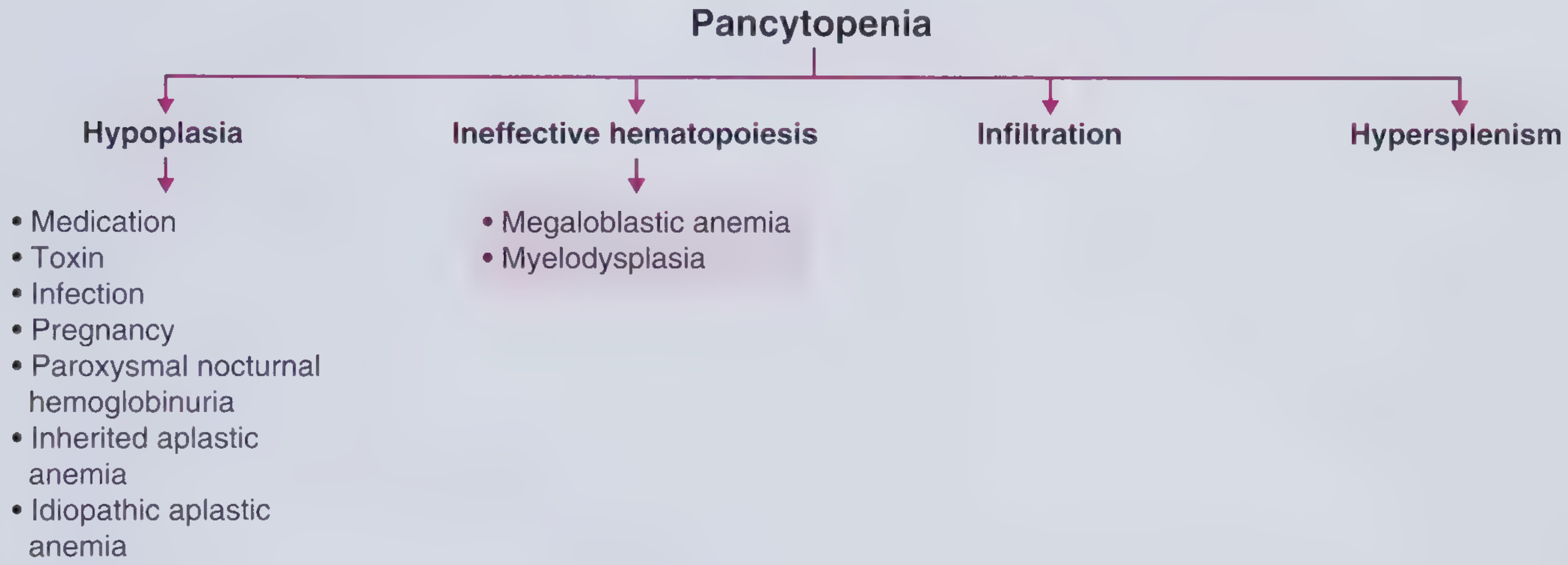
Every cause of pancytopenia falls into one of four mechanisms:
| Mechanism | Bone Marrow | Reticulocytes | Key Causes |
|---|---|---|---|
| Hypoplasia (↓ production) | Hypocellular | Low | Aplastic anaemia, drugs, radiation, PNH, Fanconi |
| Ineffective haematopoiesis | Normo/Hypercellular | Low | Megaloblastic anaemia (B12/folate), MDS |
| Infiltration (myelophthisis) | Infiltrated | Low/variable | Leukaemia, lymphoma, myelofibrosis, metastatic carcinoma, TB, Gaucher's |
| Hypersplenism | Normal/Hypercellular | Normal/High | Cirrhosis, portal hypertension, lymphoma, leishmaniasis, Felty syndrome |
Frameworks for Internal Medicine - p. 361-366; Harrison's 22e - Chapter 107
History Taking - Systematic Approach
1. Symptoms of Pancytopenia Itself
Anaemia symptoms (ask about):
- Fatigue, exertional dyspnoea, reduced exercise tolerance
- Palpitations, chest pain (cardiovascular compromise in severe anaemia)
- Pallor noticed by patient/family
Neutropenia symptoms:
- Recurrent/severe infections, fevers, rigors
- Oral ulcers, mucositis
- Specific infective symptoms (chest, urinary, skin)
Thrombocytopenia symptoms:
- Easy bruising, petechiae, purpura
- Prolonged bleeding from cuts
- Epistaxis, gum bleeding
- Heavy menstrual periods (women)
- Haematuria, melaena (more severe)
2. Aetiology-Directed History
Drug and Toxin History (CRITICAL - often missed)
Ask specifically about:
- Chemotherapy or radiation - most obvious
- Antibiotics: chloramphenicol (bone marrow toxicity, unique vacuoles on BM biopsy), linezolid, cotrimoxazole
- Antithyroid drugs: methimazole, propylthiouracil (agranulocytosis + aplasia)
- NSAIDs: indomethacin, phenylbutazone
- Anti-epileptics: carbamazepine, phenytoin
- Methotrexate, azathioprine, mycophenolate
- Alcohol: direct marrow toxin, associated folate deficiency, causes reversible pancytopenia or selective thrombocytopenia
- Arsenic/heavy metals: ask about recurrent GI symptoms, peripheral neuropathy, hair loss - a classic MRCP/FCPS vignette (arsenic poisoning by spouse!)
Nutritional History
- Dietary habits - strict vegan/vegetarian diet → B12 deficiency
- Alcohol use → folate deficiency + direct toxicity
- Malabsorption symptoms: diarrhoea, steatorrhoea, weight loss → coeliac disease, Crohn's
Infective History
- HIV risk factors (sexual history, IV drug use, transfusions)
- TB contacts, travel to endemic areas, night sweats, weight loss
- Viral infections: recent EBV (infectious mononucleosis), CMV, parvovirus B19
- Leishmaniasis: months of fever, weight loss, splenomegaly in a traveller from endemic region (Mediterranean, South Asia, East Africa) - classic MRCP vignette
Travel History
- Tropical travel raises suspicion for leishmaniasis, malaria, brucellosis, enteric fever
Past Medical History
- Autoimmune conditions: SLE (pancytopenia is a diagnostic criterion!), rheumatoid arthritis
- Known liver disease → cirrhosis + hypersplenism
- Prior haematological conditions
- HIV status
- Pregnancy (ask in all women of reproductive age)
- Thyroid disease and treatment
Family History
- Inherited bone marrow failure syndromes in children/young adults:
- Fanconi anaemia: short stature, radial ray defects, café-au-lait spots
- Dyskeratosis congenita: nail dystrophy, oral leucoplakia, skin pigmentation
- Shwachman-Diamond syndrome: pancreatic exocrine insufficiency
Constitutional/B-symptoms
- Fever > 38°C, drenching night sweats, weight loss > 10% in 6 months → lymphoma, leukaemia, TB
Social History
- Occupational exposures: benzene, pesticides, radiation (industrial)
- Alcohol intake (quantify)
Physical Examination - System by System
General Inspection
- Pallor (conjunctival, palmar)
- Jaundice → haemolysis, liver disease, megaloblastic anaemia
- Petechiae, purpura, bruising
- Weight (cachexia → malignancy, TB)
- Nutritional status
Skin and Nails
| Finding | Suggests |
|---|---|
| Petechiae/purpura | Thrombocytopenia |
| Jaundice | Megaloblastic, haemolysis, liver disease |
| Café-au-lait spots | Fanconi anaemia |
| Nail dystrophy + oral leucoplakia + hyperpigmentation | Dyskeratosis congenita |
| Butterfly rash, discoid rash | SLE |
| Spider naevi, palmar erythema, leukonychia | Chronic liver disease → cirrhosis |
| Alopecia | SLE, arsenic poisoning, chemotherapy |
Mouth and Oropharynx
- Oral ulcers → neutropenia
- Angular stomatitis, glossitis → B12/folate deficiency
- Oral leucoplakia → dyskeratosis congenita
- Thrush → immunosuppression
Lymph Nodes
- Lymphadenopathy is NOT a feature of aplastic anaemia - its presence should prompt you to think infection or lymphoma/leukaemia instead
- Generalised lymphadenopathy + elevated LDH → lymphoma
- Cervical nodes + tonsillar enlargement + splenomegaly → EBV/infectious mononucleosis
Abdomen
- Splenomegaly - most important finding
- Massive spleen: leishmaniasis, myelofibrosis, CML
- Moderate: lymphoma, portal hypertension, storage disorders (Gaucher's)
- Signs of portal hypertension (ascites, caput medusae) + splenomegaly → cirrhosis with hypersplenism
- Hepatomegaly: liver disease, lymphoma, leukaemia, infiltrative disorders
- Hepatosplenomegaly: lymphoma, leukaemia, leishmaniasis, sarcoidosis, myelofibrosis
Neurological
- Peripheral neuropathy + subacute combined degeneration (dorsal column + corticospinal tract) → B12 deficiency
- Peripheral neuropathy + GI symptoms + alopecia → arsenic poisoning
Musculoskeletal
- Symmetrical polyarthritis + splenomegaly + neutropenia → Felty syndrome (RA triad)
- Radial ray defects (absent thumbs) → Fanconi anaemia
Eyes
- Fundoscopy: flame haemorrhages, Roth spots → severe anaemia, infective endocarditis
- Uveitis → sarcoidosis, lymphoma
Putting It Together: Clue Clusters for Differentials
| Clinical Cluster | Most Likely Diagnosis |
|---|---|
| Young patient + no organomegaly + no lymphadenopathy + insidious onset | Aplastic anaemia |
| Vegan diet / elderly / glossitis / subacute combined degeneration | B12 deficiency megaloblastic anaemia |
| Elderly + macrocytosis + dysplastic features on blood film | Myelodysplastic syndrome (MDS) |
| Fever + night sweats + weight loss + lymphadenopathy | Lymphoma / leukaemia / TB |
| Chronic liver disease signs + massive splenomegaly | Cirrhosis + hypersplenism |
| Traveller from tropics + massive splenomegaly + months of fever | Visceral leishmaniasis (kala-azar) |
| RA + splenomegaly + neutropenia | Felty syndrome |
| Young woman + malar rash + arthralgia + serositis | SLE |
| PNH triad: pancytopenia + haemolysis + thrombosis (especially portal/hepatic) | Paroxysmal nocturnal haemoglobinuria (PNH) |
| Methimazole use + hyperthyroid symptoms | Antithyroid drug-induced aplasia |
| Hair loss + peripheral neuropathy + recurrent GI symptoms in spouse | Arsenic poisoning |
| Blasts on blood film | Acute leukaemia - urgent haematology referral |
| Child + short stature + radial ray defects + café-au-lait | Fanconi anaemia |
| Child + pancreatic exocrine insufficiency + short stature | Shwachman-Diamond syndrome |
Initial Investigations (Ward-Level)
Tier 1 - Order Immediately
- CBC with differential - repeat to confirm
- Peripheral blood film - single most important bedside investigation
- Blasts → leukaemia (urgent)
- Hypersegmented neutrophils + oval macrocytes → megaloblastic
- Teardrop cells (dacrocytes) + nucleated RBCs → myelofibrosis
- Abnormal lymphocytes → lymphoma/viral
- Microangiopathic changes → TTP/HUS
- Reticulocyte count
- Low → production defect (aplasia, megaloblastic, MDS, infiltration)
- High/normal → peripheral destruction (hypersplenism, haemolysis)
- LFTs, renal function, LDH, uric acid
- B12 and folate levels
- Coagulation screen (PT, APTT) - DIC, liver disease
- HIV serology
- Viral serology: EBV, CMV, hepatitis B and C
- ANA, dsDNA, complement → SLE screen
- Abdominal ultrasound - spleen size (>10 cm = splenomegaly), liver morphology, portal hypertension
Tier 2 - Guided by Clinical Context
- TSH (thyroid disease)
- Haematinics: iron studies, copper level (copper deficiency can mimic MDS)
- Blood cultures if febrile
- Bone marrow aspirate and trephine biopsy (BMAT) - indicated in most cases where cause is not obvious
- Flow cytometry (PNH screen, leukaemia/lymphoma immunophenotyping)
- Cytogenetics (MDS, leukaemia)
- Vitamin B12 absorption tests / intrinsic factor antibodies → pernicious anaemia
- Ferritin, serum iron (haemophagocytic lymphohistiocytosis - very elevated ferritin)
- Leishmaniasis serology / bone marrow for Leishman-Donovan bodies if travel history
When to Call Haematology Urgently
- Blasts on blood film (acute leukaemia)
- Severe aplastic anaemia (ANC < 200/µL, platelets < 20,000, reticulocytes < 20,000)
- Suspected PNH
- Lymphoma/myelofibrosis on blood film
- Haemophagocytic lymphohistiocytosis (fever + massive splenomegaly + very high ferritin + cytopenias)
MRCP/FCPS Exam High-Yield Points
- Aplastic anaemia: no organomegaly, no lymphadenopathy, hypocellular bone marrow - diagnosis by exclusion after thorough workup
- PNH: pancytopenia + Coombs-negative haemolytic anaemia + venous thrombosis at unusual sites (Budd-Chiari, portal vein) - diagnosed by flow cytometry (absent CD55/CD59)
- Megaloblastic anaemia: most common cause in developing world; macrocytosis + hypersegmented neutrophils + neurological symptoms; B12 is associated with subacute combined degeneration of the cord (NOT folate)
- MDS: elderly patient, macrocytic anaemia, dysplastic cells on film, may evolve to AML
- Felty syndrome: RA + splenomegaly + neutropenia (not full pancytopenia typically, but can be)
- Hairy cell leukaemia: middle-aged man, massive splenomegaly, no lymphadenopathy, "fried egg" cells on film, TRAP-positive; classic MRCP topic
- Leishmaniasis: do not miss in a traveller - bone marrow biopsy shows Leishman-Donovan bodies (amastigotes within macrophages)
- Bone marrow biopsy is usually indicated unless the cause is obvious (e.g., clear portal hypertension with cirrhosis)
- Lymphadenopathy in pancytopenia = infection or malignancy, NOT aplastic anaemia
- Reticulocyte count is your first branch point - low = production failure; high = destruction/sequestration
Sources: Harrison's Principles of Internal Medicine 22e (2025), Ch. 107 | Frameworks for Internal Medicine, pp. 361-366 | PMC review: "Approach to pancytopenia: From blood tests to the bedside" | "Practical Approach to Pancytopenia"
How to approach to a case of pancytopenia in fcps part 2 , short or long case ,, what questions can be asked in exam by professors .. and tricky concepts to remember , give relevant and medically fit mnemonics to remember the information
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
I have all the content I need from the textbooks. Now let me write the comprehensive, exam-focused answer with mnemonics.
Pancytopenia - FCPS Part 2 Short/Long Case Master Guide
The Examiner's Mental Model
Professors in FCPS/MRCP vivas are testing two things:
- Can you safely assess a sick patient (structured, systematic)
- Can you distinguish common from rare, benign from malignant
Your job in the case is to anchor on three branch points that guide everything:
MASTER MNEMONIC: "HIIH" - The 4 Mechanisms
Hypoplasia - Ineffective hematopoiesis - Infiltration - Hypersplenism
Every cause of pancytopenia lives in one of these four boxes. Internalize this framework - the examiner will push you there every time.
The SHORT CASE Approach (10-15 min)
Step 1 - Opening Statement (30 seconds)
"This is a middle-aged / elderly / young patient who appears pale / cachectic / jaundiced / well..."
Then immediately scan for:
- Pallor (anaemia)
- Petechiae / purpura / bruising (thrombocytopenia)
- Jaundice (megaloblastic, haemolysis, liver disease)
- Lymphadenopathy (malignancy, infection)
- Splenomegaly (the single most informative finding)
Step 2 - The Spleen is Your Pivot
| Spleen Size | Think First |
|---|---|
| No splenomegaly | Aplastic anaemia, megaloblastic, MDS |
| Mild-moderate splenomegaly | Lymphoma, portal hypertension, viral infections |
| Massive splenomegaly | Leishmaniasis, myelofibrosis, CML, hairy cell leukaemia |
The LONG CASE Approach
History Structure - Mnemonic: "PAID FACTS"
P - Presenting symptoms (anaemia / bleeding / infection features) A - Associated symptoms (B-symptoms, jaundice, joint pains) I - Iatrogenic / drugs (chemotherapy, chloramphenicol, MTX, antithyroids, carbamazepine) D - Dietary & nutritional (vegan diet, alcohol, malabsorption) F - Family history (inherited bone marrow failure in young patients) A - Autoimmune history (SLE, RA) C - Constitutional symptoms (fever, night sweats, weight loss → B-symptoms) T - Travel history (tropics → leishmaniasis, malaria, brucellosis) S - Social history (alcohol, occupational benzene/radiation exposure)
Physical Examination Structure - Mnemonic: "SCALP-N"
S - Skin/Mucous membranes (pallor, petechiae, jaundice, butterfly rash, café-au-lait, spider naevi) C - Cervical/Axillary/Inguinal nodes (lymphadenopathy → malignancy/infection; ABSENCE → aplastic anaemia) A - Abdomen (liver size, spleen size, ascites, caput medusae) L - Limbs (peripheral neuropathy, radial ray defects, nail dystrophy) P - Peripheral blood smear findings to correlate N - Neurological (subacute combined degeneration → B12)
Classic Examination Clue Clusters - Exam Favourites
Mnemonic for Causes by Age: "YVAM"
Young patient → aplastic anaemia, inherited marrow failure, PNH, ALL Vegan / elderly → B12 megaloblastic Aged (>60) → MDS, AML, lymphoma, myeloma Middle-aged traveller → leishmaniasis, brucellosis, viral
Questions Professors WILL Ask in FCPS Part 2
Tier 1 - They Will Always Ask These
- "What is your single most important bedside investigation?"
- Answer: Peripheral blood film - it costs nothing and tells you everything
- "You see no lymphadenopathy and no splenomegaly - what is your top diagnosis?"
- Answer: Aplastic anaemia (lymphadenopathy in pancytopenia = NOT aplastic)
- "What is the single most discriminating investigation you'd order first?"
- Answer: Reticulocyte count - it splits production failure from destruction/sequestration
- "How do you classify severity of aplastic anaemia?"
- Severe AA (SAA): BM cellularity < 25% + any 2 of: (neutrophils < 0.5 × 10⁹/L, platelets < 20 × 10⁹/L, reticulocytes < 20 × 10⁹/L)
- Very severe AA (VSAA): same as SAA but neutrophils < 0.2 × 10⁹/L
- "What is the triad of PNH?"
- Pancytopenia + Haemolysis (Coombs-negative) + Venous thrombosis at unusual sites
- "How do you diagnose PNH?"
- Flow cytometry - absent CD55 and CD59 on RBCs and granulocytes
- "What organism do you look for in the bone marrow of a patient with massive splenomegaly returning from South Asia?"
- Leishman-Donovan bodies (amastigotes of Leishmania donovani within macrophages)
- "What blood film finding tells you this patient needs urgent haematology?"
- Blast cells → acute leukaemia, do not delay
Tier 2 - Tricky Professor Traps
- "A patient has B12 deficiency. Should you give folate?"
- NOT before replacing B12 - giving folate alone in B12 deficiency can precipitate or worsen subacute combined degeneration of the cord (SCD)
- "Hairy cell leukaemia - what is specific on the blood film?"
- Dry tap on aspirate (fibrosis), cells with "fried egg" / hairy cytoplasmic projections, TRAP stain positive, CD103+
- "Your patient has pancytopenia and is COOMBS NEGATIVE with haemolysis - what does that tell you?"
- Think PNH (complement-mediated, not antibody-mediated, hence Coombs-negative)
- "What is Felty syndrome?"
- RA + splenomegaly + neutropenia (the triad) - can give pancytopenia
- "What is the most common cause of pancytopenia in the developing world?"
- Megaloblastic anaemia (B12/folate deficiency)
- "What is the relationship between PNH and aplastic anaemia?"
- They overlap - PNH clones can emerge from aplastic anaemia; both share immune-mediated stem cell destruction. 5-10% of aplastic patients develop PNH over time
- "Name an infection that causes pancytopenia via haemophagocytosis"
- EBV, CMV, parvovirus B19, TB - all can trigger Haemophagocytic Lymphohistiocytosis (HLH)
TRICKY CONCEPTS TO REMEMBER
1. The "No Lymphadenopathy" Rule
- Aplastic anaemia = NO lymphadenopathy, NO splenomegaly
- If you see either → reconsider (lymphoma, leukaemia, infection)
2. PNH Thrombosis is "Backwards"
- Thrombosis typically at unusual venous sites: hepatic vein (Budd-Chiari), portal vein, cerebral sinuses
- A young patient with Budd-Chiari + no liver disease = PNH until proven otherwise
3. B12 vs Folate Neurological Rule
"B12 causes B(rain) and Spinal cord disease - Folate does NOT"
- Subacute combined degeneration = B12 ONLY
- Folate deficiency can cause NTDs in pregnancy but NOT SCD
4. Reticulocyte Count Interpretation
| Reticulocyte Count | Marrow Response | Mechanism |
|---|---|---|
| Low (< 20 × 10⁹/L) | Failure | Aplasia, MDS, megaloblastic, infiltration |
| Normal/High (> 80 × 10⁹/L) | Responding | Hypersplenism, haemolysis |
5. Drug Causes - Mnemonic "CALM-ABC"
Chloramphenicol - Antithyroid (methimazole/PTU) - Linezolid - Methotrexate - Anticonvulsants (carbamazepine) - Benzene - Chemotherapy
6. Bone Marrow is Hypocellular vs Hypercellular - Key Decision
| Bone Marrow | Think |
|---|---|
| Hypocellular (< 25% cellularity) | Aplastic anaemia, drugs, radiation, Q fever, anorexia |
| Normocellular / Hypercellular | MDS, megaloblastic, infiltration, hypersplenism, PNH |
This is why bone marrow biopsy (trephine) is essential - aspirate alone is not enough
7. Hepatitis + Aplastic Anaemia
- Seronegative hepatitis (unknown viral agent) is a well-recognized trigger for aplastic anaemia
- Acute hepatitis → aplastic anaemia within weeks to months
- Examiner loves this because it surprises candidates
8. MDS vs Megaloblastic - How to Tell Apart
| Feature | Megaloblastic | MDS |
|---|---|---|
| Age | Any (vegan) / elderly | Elderly (usually > 60) |
| B12/folate | Low | Normal |
| Response to treatment | Rapid (days) | No response |
| Bone marrow | Hypercellular, nuclear-cytoplasmic dissociation | Dysplastic changes, ring sideroblasts |
| Natural history | Curable | Progressive, may → AML |
9. HLH - The Killer Diagnosis Not to Miss
- Fever + massive splenomegaly + pancytopenia + ferritin > 500 ng/mL (often > 10,000)
- Bone marrow shows macrophages engulfing blood cells (haemophagocytosis)
- Triggered by EBV, CMV, TB, lymphoma
- HScore - used to calculate probability of HLH
10. Fanconi Anaemia Classic FCPS Vignette
- Child with pancytopenia + short stature + absent thumbs / radial aplasia + café-au-lait spots
- Confirmed by chromosomal breakage test (DEB/MMC test)
- High risk of AML and solid tumours
Causes Mnemonic - "MIAMI BLAST" (for ALL causes)
M - Megaloblastic anaemia (B12/folate) I - Infiltrative (leukaemia, lymphoma, myelofibrosis, metastases, TB, Gaucher's) A - Aplastic anaemia (idiopathic, drugs, toxins, infections) M - Medications / toxins (chloramphenicol, benzene, MTX, alcohol) I - Infections (HIV, EBV, CMV, TB, leishmaniasis, HLH) B - B12/folate already covered (reinforcer) L - Liver disease / hypersplenism (cirrhosis, portal hypertension) A - Autoimmune (SLE, Felty, AIHA) S - Storage / systemic (Gaucher's, sarcoidosis, PNH) T - Tropical (leishmaniasis, malaria, brucellosis)
Blood Film Findings - Rapid Recognition Table
| Blood Film Finding | Diagnosis |
|---|---|
| Hypersegmented neutrophils + oval macrocytes | Megaloblastic anaemia |
| Blast cells (large immature cells) | Acute leukaemia - URGENT |
| Teardrop cells (dacrocytes) + nucleated RBCs | Myelofibrosis |
| "Fried egg" / hairy cytoplasmic projections | Hairy cell leukaemia |
| Bilobed / hypolobated neutrophils (Pelger-Huet) | MDS |
| Microangiopathic haemolytic anaemia (MAHA) + thrombocytopenia | TTP/HUS (not true pancytopenia) |
| Smear cells (smudge cells) | CLL (can cause hypersplenism) |
| Ring sideroblasts on iron stain | MDS with ring sideroblasts |
| Amastigotes within macrophages | Leishmaniasis |
Summary Algorithm for the Viva
PANCYTOPENIA confirmed on CBC
|
↓
PERIPHERAL BLOOD FILM + RETICULOCYTES
|
________|________
| |
BLASTS? No blasts
| |
Leukaemia Reticulocytes low?
(URGENT) YES → Production failure
NO → Hypersplenism / destruction
|
BONE MARROW
Hypocellular → Aplasia
Hypercellular + dysplasia → MDS/Megaloblastic
Infiltrated → Malignancy/TB/Gaucher's
One-Line Exam Closers (Impress the Examiner)
- "In pancytopenia, lymphadenopathy essentially rules out aplastic anaemia."
- "PNH is the only condition that causes Coombs-negative haemolysis with thrombosis at unusual venous sites."
- "A dry tap on bone marrow aspirate in a middle-aged man with massive splenomegaly = hairy cell leukaemia."
- "Seronegative hepatitis is an underappreciated but well-established trigger for aplastic anaemia."
- "Megaloblastic anaemia is the most common cause of pancytopenia in the developing world - B12 and folate must always be checked before bone marrow biopsy."
- "Very high ferritin (> 10,000) in a febrile patient with pancytopenia = HLH until proven otherwise."
Sources: Harrison's Principles of Internal Medicine 22e (2025), Ch. 107 | Frameworks for Internal Medicine, pp. 361-366 | Quick Compendium of Clinical Pathology 5e | PMC: Approach to pancytopenia - blood tests to bedside
This is a shared conversation. Sign in to Orris to start your own chat.