Paronychia treatment
Reading File
Finding Sources
Searching PubMed
paronychia treatment management
Reading File
Reading File
Reading File
Loading Image
I have comprehensive material. Here is a structured answer:
Paronychia Treatment
Overview
Paronychia is an infection of the lateral nail fold (paronychium), occasionally extending to the cuticle or eponychium. It begins as cellulitis and may progress to frank abscess formation. The most common organisms are S. aureus (including CA-MRSA), Streptococcus species, and anaerobes. In children, anaerobes predominate (linked to finger-sucking/nail-biting). Chronic paronychia (>6 weeks) often involves Candida albicans, especially in immunocompromised patients.
Stage-Based Treatment
1. Early Cellulitis (No Fluctuance)
- Warm soaks 3x daily
- Elevation of the hand
- Oral antibiotics - a short course of a broad-spectrum antistaphylococcal agent (cephalosporin or semisynthetic penicillin)
- Topical antibiotics with or without topical corticosteroids are also used
- Incision has no value at this stage
2. Abscess with Fluctuance - Drainage
Drainage is quickly curative. The key is that paronychia is not a true cutaneous abscess - it is a pus collection in the potential space between the cuticle and the proximal nail.
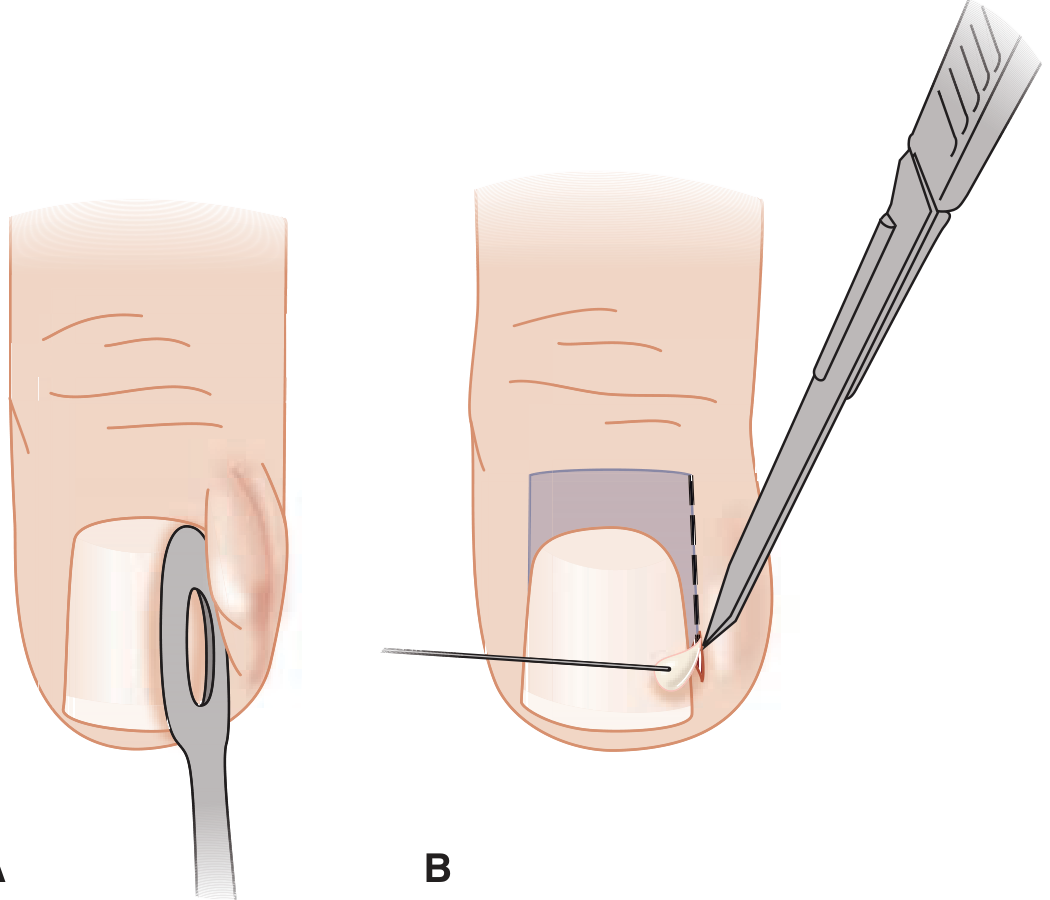
Procedure:
- Perform a digital nerve block (required for most patients; minor infections may tolerate the procedure without anesthesia)
- Soften the eponychium with warm soaks beforehand
- Advance a No. 11 blade, scissors, or 21-23 gauge needle parallel to the nail, lifting the eponychial fold away from the nail matrix - this allows pus to drain without a formal skin incision
- Avoid incising across the eponychial fold (risk of nail deformity)
- Actual skin incision or nail removal is rarely needed as the initial approach
Post-drainage care:
- Warm soaks to keep wound open and clean
- Hand elevation and immobilization
- Routine antibiotics are NOT needed after uncomplicated I&D unless cellulitis, immunocompromise, or vascular insufficiency is present
- When antibiotics are used post-drainage, a 7-day course is typical
- Reassess within 48 hours in complicated cases
3. Extensive / Deep Infection
- If pus extends beneath the nail: remove the lateral or proximal nail portion to ensure adequate drainage
- If the nail is free-floating on a bed of pus: remove the entire nail
- These cases require formal digital block before any procedure
Antibiotic Selection
| Situation | Agent |
|---|---|
| Cellulitis, no abscess | Antistaphylococcal cephalosporin or semisynthetic penicillin |
| MRSA concern | TMP-SMX or clindamycin |
| Post-I&D with cellulitis | Same as above, 7-day course |
| Bite-related / anaerobic | Amoxicillin-clavulanate |
Chronic Paronychia (>6 weeks)
- Avoid wet environments
- Topical corticosteroids + topical antifungals (for Candida)
- Rarely responds to ED intervention
- Refer to dermatology
- Associated with certain drugs: antiretroviral therapy for HIV, epidermal growth factor receptor (EGFR) inhibitors, and FGFR inhibitors
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, 7e - Tintinalli's Emergency Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.