Mucociliary clearance, nasal cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent content gathered. I now have comprehensive material from multiple textbooks. Let me compile the full answer.
Mucociliary Clearance
Overview
Mucociliary clearance (MCC) is the primary innate defense mechanism of the respiratory tract - it removes inhaled particles, microorganisms, and debris by trapping them in mucus and transporting that mucus toward the pharynx, where it is swallowed. In healthy subjects, clearance is usually completed within 24 hours of deposition.
- Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders
Airway Surface Liquid (ASL) - Two-Layer System
The airway lumen is lined by two distinct liquid layers:
-
Mobile mucus layer (gel layer) - composed primarily of secreted polymeric mucins. Water accounts for ~98% of its mass; mucins only ~0.5% (yet form the structural backbone). The two major secreted mucins are MUC5AC and MUC5B - both are exceedingly large glycoproteins (up to 3 × 10⁶ Da) that polymerize into long chains and branched networks. MUC5AC forms branched covalent networks; MUC5B forms end-to-end polymers.
-
Periciliary layer (PCL / sol layer) - stationary layer immediately surrounding the cilia, containing membrane-tethered mucins and glycoconjugates. Cilia beat within the PCL; their tips contact the overlying gel layer during the power stroke, propelling it.
The PCL maintains a higher osmotic modulus than the mucus layer above it - this "gel-on-gel" architecture prevents cilia from collapsing. If mucus becomes dehydrated and hyperosmolar (e.g., cystic fibrosis), it draws water out of the PCL, causing cilia to collapse and impair transport.
- Fishman's Pulmonary Diseases and Disorders, p. 326-345
Mucus Composition and Secretory Cells
| Component | Detail |
|---|---|
| Water | ~98% of mucus mass |
| Mucins (MUC5AC, MUC5B) | ~0.5%; principal macromolecular component |
| Salts | ~0.9% |
| Globular proteins | ~0.6% |
| Periciliary immunoproteins | Macrophages, neutrophils, IgA/G/M/E, lysozymes, lactoferrin, interferon |
Mucins are packaged dehydrated in secretory granules; after secretion they adsorb several hundred-fold their mass in water. Adequate bicarbonate must also be present to bind calcium and allow proper mucin expansion. Insufficient surface liquid leads to over-viscous, adhesive mucus that resists clearance.
- Goblet cells produce thick, carbohydrate-rich secretions.
- Submucosal glands (lined by mucinous and serous cells) also contribute and become hypertrophic in chronic bronchitis.
- Seromucinous glands and goblet cells are the main contributors in the nose.
- K.J. Lee's Essential Otolaryngology; Fishman's
Ciliary Structure and Beat Mechanics
- Each multiciliated cell has hundreds of cilia arranged on its apical surface.
- The ciliary axoneme has the classic 9+2 microtubule structure with inner and outer dynein arms - dynein ATPase motors generate the sliding force between microtubules.
- Beat pattern: asymmetric two-phase cycle
- Fast, forward power stroke - extended cilium sweeps through the gel layer, propelling mucus proximally.
- Slower, backward recovery stroke - cilium bends close to the cell surface, moving through the lower-viscosity PCL to minimize backward drag on mucus.
- Cilia beat in metachronal waves - sequential (not synchronized) activity produces a coordinated wave along the airway epithelium.
Regulation of Ciliary Beat Frequency (CBF)
- Increased intracellular calcium → increased CBF
- Increased nitric oxide (NO) → increased CBF
- ATP released extracellularly activates P2Y2 receptors → drives mucin secretion, ion channel opening, and increased CBF; subsequent dephosphorylation to adenosine activates A2b receptors for sustained hydration signals (purinergic signaling cascade)
- Hyperviscous mucus → reduced CBF and efficiency
- Murray & Nadel's, p. 4145-4160
Direction of Mucociliary Transport
- In the lungs: movement is from peripheral airspaces toward the mouth (distal-to-proximal).
- In the nose: mucus travels along the nasal mucosa at 2-10 mm/h toward the nasopharynx.
- In the Eustachian tube/middle ear: cilia transport the mucous blanket from the tympanic orifice toward the nasopharynx. This is an active process - not gravity-dependent.
- Planar cell polarity establishes the directional orientation of cilia. Wnt signaling pathways are involved. The direction is developmentally programmed - surgical reversal of a tracheal segment does NOT reverse cilia beat direction.
- Ciliated cells are most numerous in the trachea and lobar bronchi, decreasing progressively distally.
- Murray & Nadel's; Cummings Otolaryngology
Particle Filtration
- Particles >12 µm are filtered in the nose.
- Particles depositing in ciliated airways are trapped in mucus and cleared centrally.
- If MCC is impaired, coughing becomes the backup clearance mechanism.
- If both MCC and cough fail: retained secretions produce airway obstruction and amplify inflammatory processes.
Evaluation of Mucociliary Transport
| Test | Method |
|---|---|
| Saccharin test | 0.5-mm saccharin particle placed ~1 cm behind the anterior inferior turbinate; time measured until first sweet taste in nasopharynx |
| ⁹⁹Tc-macroaggregated albumin scintigraphy | Radiolabeled droplet placed at anterior nasal floor; gamma camera images over 10-20 min measure transport to nasopharynx |
| Electron microscopy | Absent/shortened outer dynein arms of ciliary ultrastructure in ciliary dyskinesia |
| Nasal nitric oxide | Reduced in primary ciliary dyskinesia (PCD) and cystic fibrosis |
- K.J. Lee's Essential Otolaryngology
Diseases Impairing Mucociliary Clearance
Primary Ciliary Dyskinesia (PCD)
- Congenital, genetically heterogeneous disorder of dynein arms or other ciliary components → loss of ciliary movement.
- Leads to mucus stasis → bronchiectasis, sinusitis, and near-universal otitis media.
- In males: infertility (immotile spermatozoa).
- May cause situs inversus / dextrocardia (role of monociliated cells in embryogenesis - Kartagener syndrome when PCD + situs inversus).
- Nasal NO is markedly reduced.
Cystic Fibrosis (CF)
- Defective CFTR (chloride channel) → reduced chloride secretion into airway lumen + increased ENaC-mediated sodium absorption (worsened by inflammatory proteases) → mucus dehydration → hyperviscous mucus → impaired MCC.
- Airway secretions contain mucus + DNA and actin from dead neutrophils (neutrophil extracellular traps).
- Treatments: hypertonic saline (osmotic gradient draws water into lumen), inhaled mannitol, recombinant DNase (dornase alfa), CFTR modulators.
Acquired causes
-
Tobacco smoking, influenza, and other upper respiratory viruses (ciliated cells may take 1 month to regenerate after viral damage).
-
Bacterial infection (endotoxin release + inflammatory pathways damage cilia).
-
Chronic bronchitis: goblet cell hyperplasia in distal airways, submucosal gland hypertrophy.
-
Chronic sinusitis, middle ear effusions: hyperviscous secretions reduce CBF.
-
Murray & Nadel's; Cummings Otolaryngology; Fishman's
Nasal Cycle
Definition and Mechanism
The nasal cycle is the physiological, cyclical alternation of mucosal congestion and decongestion between the right and left nasal cavities. It was first described by Heetderks in 1927, who documented alternating turgescence of the inferior turbinates in ~80% of a normal population.
-
The changes are driven by vascular activity - specifically, alterations in the volume of blood in capacitance vessels (venous sinusoids) of the nasal mucosa.
-
The cycle is alternating: as one side congests, the other decongests, such that total nasal resistance remains relatively constant.
-
Duration: every 2-12 hours (Heetderks' original observation: mean ~2.5 hours; Scott-Brown's range: 4-12 hours).
-
Demonstrable in up to 80% of adults but not easy to demonstrate in children.
-
Scott-Brown's Otorhinolaryngology; Cummings Otolaryngology
Control: Autonomic Nervous System
The autonomic nervous system is the primary regulator:
- Parasympathetic (vagal) overactivity → vasodilation of sinusoids → nasal congestion.
- Sympathetic tone → vasoconstriction → decongestion.
- High CO₂ in inspired air (rebreathing) → increases nasal resistance; hyperventilation reverses this.
- Drugs that block noradrenaline action → congestion (increased resistance).
- Antihistamines have anticholinergic (anti-parasympathetic) effects → increase sympathetic tone → improve nasal airway.
- Hormonal changes (puberty, pregnancy) affect the nasal mucosa and the cycle.
Factors Affecting the Nasal Cycle
Exercise, pregnancy, hormones, infections, allergy, fear, emotions, sexual activity, body position (lateral decubitus → dependent side congests), and medications all influence the cycle.
Positional effect: When lying on one side, the dependent nasal fossa turbinates fill - this is thought to be one purpose of the cycle (prompting a sleeping person to turn over).
Clinical Significance
Paradoxical Nasal Obstruction
In patients with a deviated nasal septum, the nasal cycle creates a clinically important paradox:
- On the deviated (obstructed) side, patients learn to subconsciously habituate to the steady-state increased resistance.
- The normal (open) side varies with the cycle; when it enters the congested (turgescent) phase, the patient perceives obstruction on what appears to be the clinically wider side.
- This is paradoxical nasal obstruction - the patient complains of the side that looks more patent on examination.
- This unilateral turbinate enlargement is often a normal variant and must not be misinterpreted as pathological.
- Surgical correction must address both the deviated septum AND the hypertrophied turbinate.
Unilateral Turbinate Enlargement
Inferior turbinate hypertrophy on one side in the context of a contralateral septal deviation is often compensatory - the turbinate enlarges into the more open passage to normalize resistance.
- Cummings Otolaryngology, p. 3048-3052
Nasal Cycle and Olfaction
The nasal cycle can increase unilateral nasal resistance by up to 4 times, but multiple studies show minimal effect on monorhinal olfactory threshold. A proposed functional benefit is that differential flow rates between the two sides simultaneously expose the olfactory epithelium to a broader range of odorants (fast-flowing side better detects low-volatility odorants; slow-flowing side better detects high-volatility odorants), thereby expanding the detectable odorant range - a possible evolutionary purpose for the nasal cycle.
- Cummings Otolaryngology, p. 900
Summary Comparison
| Feature | Mucociliary Clearance | Nasal Cycle |
|---|---|---|
| Primary function | Remove particles/pathogens | Alternate nasal airway resistance; possibly enhance olfaction |
| Key structure | Ciliated epithelium + mucus (gel + PCL) | Venous sinusoids (capacitance vessels) of inferior turbinate |
| Control | Purinergic signals, Ca²⁺, NO, autonomic | Autonomic NS (sympathetic/parasympathetic) |
| Rate | 2-10 mm/h (nasal); faster centrally | Cycle every 2-12 hours |
| Key pathology | PCD, CF, chronic bronchitis | Paradoxical nasal obstruction (deviated septum) |
| Evaluated by | Saccharin test, ⁹⁹Tc scintigraphy, nasal NO, EM | Rhinomanometry, acoustic rhinometry |
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine
- Fishman's Pulmonary Diseases and Disorders
- Cummings Otolaryngology - Head and Neck Surgery
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1
- K.J. Lee's Essential Otolaryngology
Otitis media with effusion and tympanostomy tubes
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - great images retrieved. Now I have everything needed for a comprehensive answer.
Otitis Media with Effusion (OME)
Definition
OME is a serous or mucoid (non-purulent) collection of fluid within the middle ear space in the absence of signs or symptoms of acute infection. Unlike acute otitis media (AOM), OME is not classified by duration - it can present over hours or persist for decades. The historical terms "glue ear," "secretory otitis media," and "serous otitis media" all refer to this condition.
Epidemiology
- Most common cause of acquired hearing loss in children.
- Point prevalence on screening: up to 20% of children.
- Peak incidence around 1 year of age; by age 3, nearly all children have experienced at least one episode.
- OME in most children is mild and resolves spontaneously; it becomes clinically significant when bilateral, persistent, or occurring during critical developmental windows.
- Cummings Otolaryngology
Risk Factors
| Host Factors | Environmental Factors |
|---|---|
| Male sex | Low socioeconomic status |
| Age <1 year at first AOM | Daycare attendance |
| Genetic predisposition | Tobacco smoke exposure |
| Craniofacial abnormalities (cleft palate) | Fall/winter season |
| Immunodeficiency | Recurrent URTIs |
| Adenoid hypertrophy | Pacifier use |
| Down syndrome | Older siblings |
Protective: breastfeeding.
Ongoing debate exists about prematurity, allergy, obesity, and gastroesophageal reflux as contributing factors.
Pathophysiology
OME is multifactorial. Two major theories (which are increasingly seen as complementary):
1. Eustachian Tube Dysfunction (Classic Model)
The Eustachian tube's three functions are:
- Pressure equalization (ventilation) of the middle ear
- Mucociliary clearance of secretions toward the nasopharynx
- Protection of the middle ear from nasopharyngeal pathogens
When the ET fails in ventilation, increasingly negative middle ear pressure develops → transudation of fluid that fails to clear.
Why children are more susceptible: The pediatric ET is:
- Smaller in diameter
- More horizontal in orientation (vs. the adult 45° angle)
- More compliant/flexible
- More susceptible to dysfunction from lymphoid tissue (adenoids) at the nasopharyngeal orifice
ET dysfunction arises from:
- Inflammatory causes: allergic disease, LPR/GERD, viral URTIs (mucosal edema)
- Anatomic causes: cleft palate (abnormal tensor/levator veli palatini insertion), synechiae from surgery, nasopharyngeal masses
- Functional causes: ciliary dysmotility (smoking-related, syndromic)
- Mechanical obstruction: prominent adenoid tissue, nasopharyngeal masses
2. Biofilm / Chronic Inflammation Model (Emerging Evidence)
Traditional cultures of MEE are usually negative because bacteria are not free-floating but sequestered in biofilms on the mucosal surface. Biofilms are polysaccharide matrices in "tower and mushroom" configurations that:
- Protect bacteria from host defenses and antibiotics
- Allow bacterial communication via hormonal (quorum sensing) signals
- Persist subclinically, secreting endotoxins and exotoxins
Key studies:
- Post (2001): demonstrated H. influenzae biofilms in a chinchilla model by SEM
- Hall-Stoodley (2006): confocal laser-scanning microscopy found biofilms in mucosal biopsies of 92% of children with chronic OME, vs. 0% of controls
- Coates (2008): transmission electron microscopy demonstrated intracellular bacterial infection of middle ear mucosal epithelial cells in OME
Inflammatory Cascade in OME
Once triggered, the inflammatory process in the submucosa involves:
-
Early mediators: arachidonic acid metabolites, histamine, platelet-activating factor, adhesion molecules
-
Key cytokines: TNF-α and IL-1β are the primary drivers; also IL-6, IL-8 (pro-inflammatory); IL-2, IL-4, IL-5, IL-10, IFN-γ (immunoregulatory); TGF-β and IL-10 (downregulation)
-
Mucosal response: proliferation of lining + secretion of mucus; basal cells differentiate into goblet and ciliated cells → thick, tenacious mucoid effusion rich in mucins
-
The mucin content primarily determines effusion viscosity (children tend toward more mucoid; adults more serous effusions)
-
Shambaugh Surgery of the Ear; Cummings Otolaryngology
Clinical Features
| Feature | Detail |
|---|---|
| Hearing loss | Conductive, typically mild-moderate (15-40 dB HL); often the only symptom |
| Aural fullness | Common |
| Autophony | Own voice sounds louder |
| Otalgia | Generally absent (distinguishes from AOM) |
| Crackling/popping | Air bubbles entering middle ear |
| Balance/motor issues | MEE can affect vestibular end-organ; effects on balance typically reverse with resolution |
| Speech/language delay | Associated with bilateral persistent OME in critical developmental period |
Often asymptomatic - many cases detected only on screening audiometry.
Diagnosis
Otoscopy
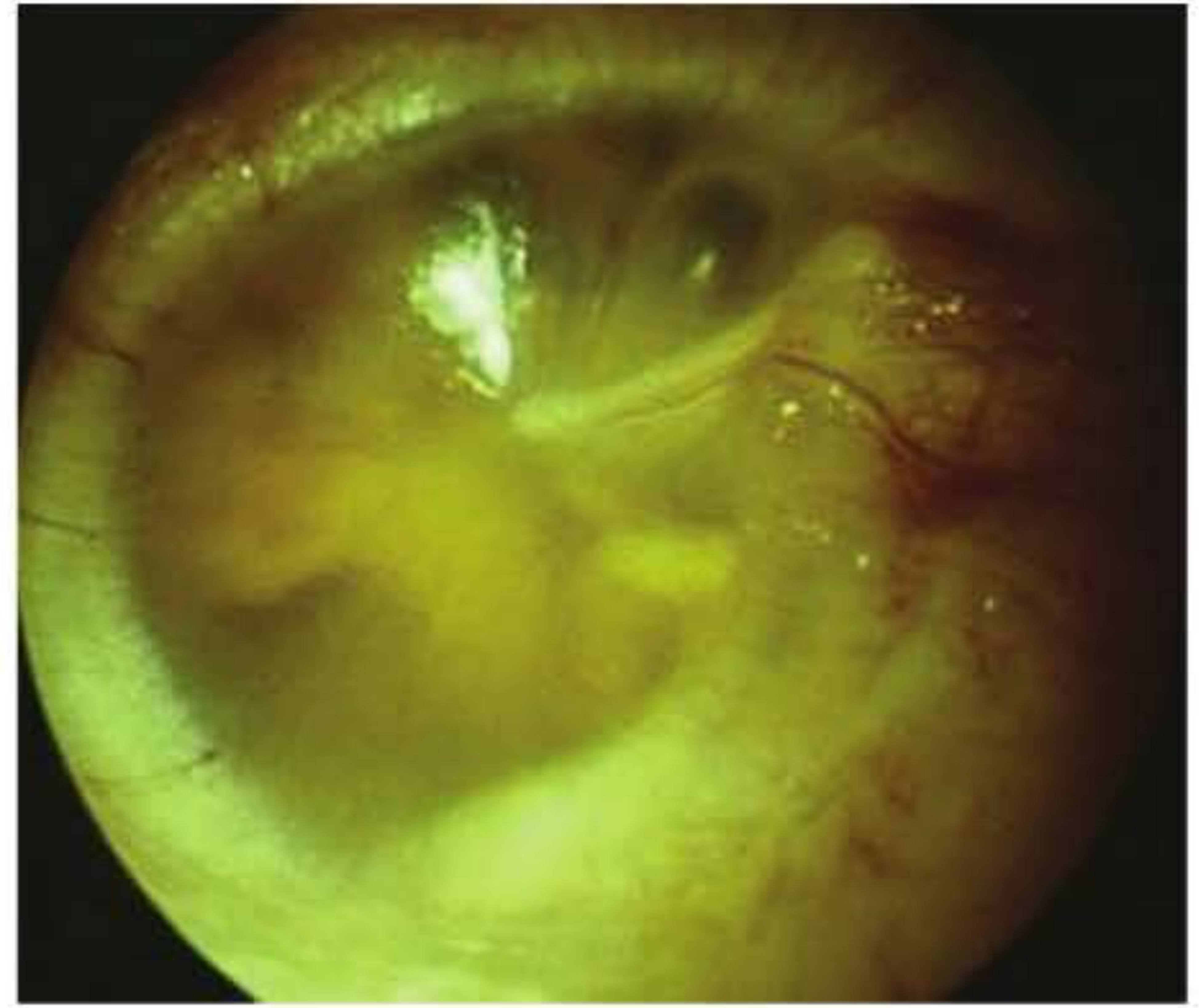
- Amber (yellow/orange) effusion visible behind an intact tympanic membrane
- Air-fluid level or air bubbles may be present
- TM appears dull, retracted, or with decreased mobility
- On pneumatoscopy (Siegle speculum): limited or no TM excursion
Audiometry
- Flat conductive hearing loss (air-bone gap)
Tympanometry
- Type B (flat) curve - no tympanometric peak
- Normal ear canal volume (distinguishes from perforation, where ECV is high)
- Absent stapedial reflexes
Imaging (CT/MRI)
- Opacification of middle ear and mastoid air cell spaces
- No erosion of mastoid septa or cortical bone (distinguishes from coalescent mastoiditis or cholesteatoma)
Natural History and Consequences
- Most OME resolves spontaneously within several months.
- Prolonged bilateral OME → conductive hearing loss → speech and language delay, particularly if occurring during critical developmental periods (first 2-3 years).
- Long-term OME (untreated) can lead to:
- TM atrophy and atelectasis
- Ossicular fixation and erosion
- Retraction pockets → risk of cholesteatoma
- Tympanosclerosis
Management
1. Watchful Waiting
- First-line approach for most children.
- OME resolves spontaneously in the majority within 3 months.
- Hearing should be monitored during this period.
2. Medical Therapy
- Antibiotics: modest short-term benefit; not routinely recommended due to side effects and resistance concerns.
- Intranasal corticosteroids: may reduce adenoid size and ET inflammation; modest effect.
- Antihistamines/decongestants: not recommended (no evidence of benefit).
- Autoinflation (e.g., Otovent device): may help in cooperative older children.
3. Surgical Management - Tympanostomy Tubes
Indicated when:
- Bilateral OME with hearing loss persisting ≥3 months
- Bilateral OME with associated speech/language delay or developmental concerns
- Bilateral OME with at-risk children (cleft palate, Down syndrome, permanent hearing loss, autism, etc.)
- Recurrent AOM with MEE
Tympanostomy Tubes (Ventilation Tubes / Grommets)
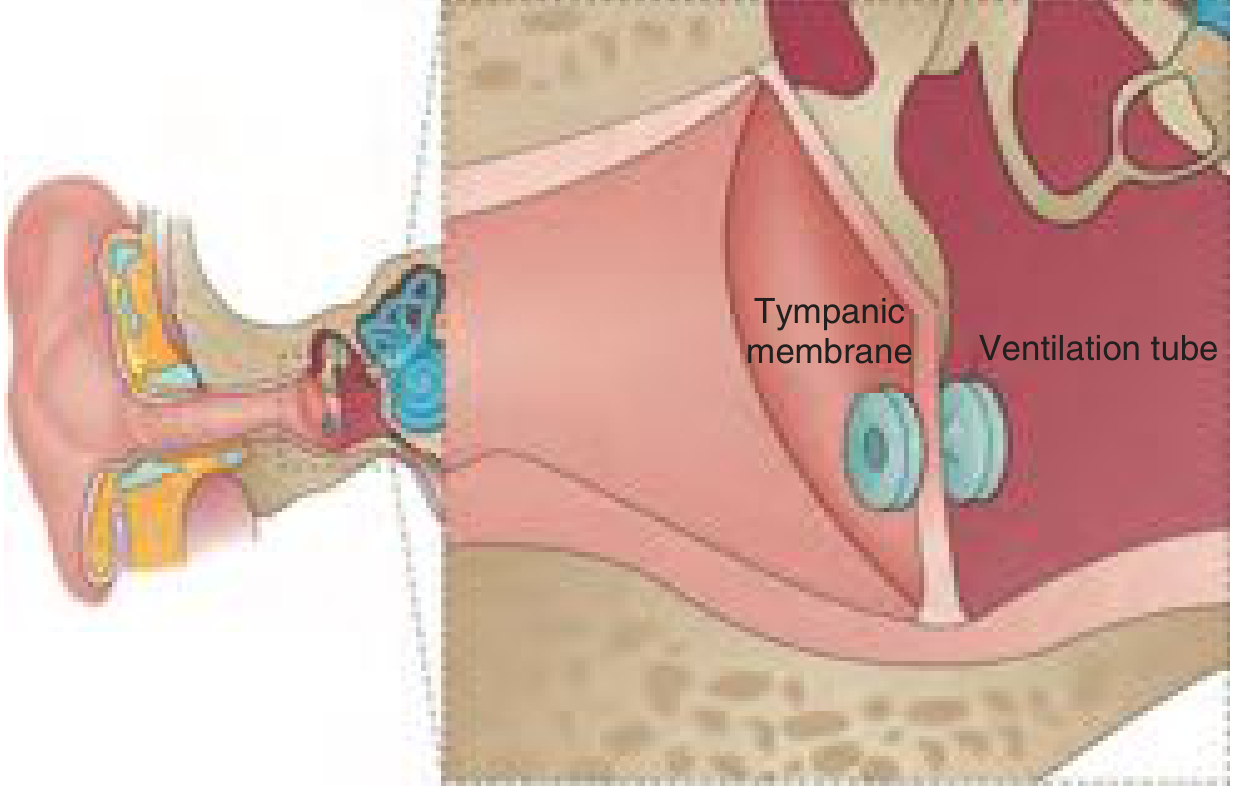
Mechanism of Action
Tympanostomy tubes:
- Provide middle ear ventilation - equalize middle ear pressure with atmospheric pressure, bypassing the dysfunctional ET
- Allow drainage of MEE through the external canal
- Reverse and prevent re-accumulation of MEE
- Create a less favorable environment for microbial growth
- Enable topical treatment of subsequent AOM episodes with antibiotic eardrops directly through the tube (avoiding systemic antibiotics)
Types of Tubes
| Type | Design | Duration | Use |
|---|---|---|---|
| Short-term / Grommet (e.g., Shepard, Armstrong) | Short flanges | ~6-14 months; self-extruding | Most children with OME or rAOM |
| Long-term / T-tube (e.g., Goode T-tube) | Larger medial flange | 2-4+ years | Cleft palate, atrophic TM, multiple prior sets of tubes, craniofacial anomalies |
Extrusion data (randomized trial, 75 children):
- Shepard tubes: 93% extruded by 2 years
- Armstrong tubes: 80% extruded by 2 years
- Reuter-Bobbin: 66% by 2 years
- Goode T-tubes: only 31% extruded by 2 years
Time to extrusion depends on: tube size, medial flange shape, presence of lateral flange, and material. Silicone tubes are associated with the longest time to first infection.
Surgical Technique
- Anesthesia: almost always general anesthesia (face mask) in children; IV access often not required for uncomplicated cases.
- Nitrous oxide can be used - it enhances instrumentation by expanding gases within the middle ear.
- A myringotomy incision is made (typically in the anteroinferior quadrant), MEE is aspirated, and the tube is placed.
- Procedure is brief (minutes per ear).
Indications - AAO-HNS Guidelines
- OME: tubes recommended for bilateral OME with documented hearing loss persisting ≥3 months, or OME of any duration in at-risk children.
- rAOM with MEE present in at least one ear at time of assessment: tubes recommended as an option.
- rAOM without MEE: tubes not recommended by 2013 AAO-HNS guidelines (AAP guidelines allow tubes as an option after failed preventive/medical treatments).
For rAOM: limited evidence shows tympanostomy tubes modestly reduce AOM recurrences vs. observation (approximately 1 fewer episode per 6 months). The largest effect is seen in children with MEE persisting between episodes.
Postsurgical Follow-up
- First visit: 2-3 months after surgery (otoscopy + audiometry)
- Ongoing: every 6-12 months thereafter, or sooner if problems arise
- Monitor for tube patency, extrusion, TM changes
Complications and Sequelae
| Complication | Incidence | Notes |
|---|---|---|
| Acute otorrhea | 25-75% of children develop ≥1 episode | Most common complication; treated with ototopical fluoroquinolone drops (first-line) |
| Tympanosclerosis | ~32% | Calcification of TM; cosmetically significant but rarely affects hearing |
| Focal TM atrophy | ~25% | Weakening of TM layers |
| Retraction pockets | ~3.1% | Risk of subsequent cholesteatoma |
| Persistent perforation | ~4.8% overall (2.2% short-term; 16.6% long-term tubes) | Usually small; myringoplasty if persistent |
| Early extrusion | ~3.9% | Related to infection, improper placement, or atrophic TM |
| Tube blockage | Variable | Dried blood, mucus, or granulation tissue; may require suction |
| Cholesteatoma | 0-6.5% (debated) | Causality controversial; may reflect underlying pathology rather than tube per se |
Management of Otorrhea
- First-line: ototopical fluoroquinolone drops (e.g., ciprofloxacin) - more effective and cost-effective than oral antibiotics; aminoglycoside drops avoided due to potential ototoxicity.
- If no resolution in 2 weeks: culture from tube opening to guide therapy.
- If yeast predominant: topical clotrimazole.
- Persistent/recurrent otorrhea: consider tube removal (biofilm formation on tube may perpetuate drainage).
Prevention of Immediate Postoperative Otorrhea
- Multiple saline washouts (NNT 7)
- Single application of antibiotic-corticosteroid drops intraoperatively (NNT 13)
- Single application of 6% ciprofloxacin otic suspension intraoperatively
Adenoidectomy as Adjunct
- Adenoids serve as a nasopharyngeal reservoir for respiratory pathogens and may obstruct ET function.
- Meta-analysis of 10 RCTs: adenoidectomy (alone or with tubes) most beneficial in children <2 years with rAOM.
- Benefit is modest and must be weighed against surgical risk.
- Re-insertion of a second set of tubes: adding adenoidectomy at this point is supported by evidence and reduces the need for further sets.
Special Populations
| Population | Considerations |
|---|---|
| Cleft palate | Near-universal OME due to abnormal tensor veli palatini; long-term tubes preferred |
| Down syndrome | Narrow EACs complicate examination; may need ABR under GA; diagnosis challenging |
| Craniofacial abnormalities | Higher OME prevalence; heightened surveillance needed |
| Primary ciliary dyskinesia | OME near-universal; tubes often required repeatedly |
Summary: OME vs. AOM
| Feature | OME | AOM |
|---|---|---|
| Fluid | Serous/mucoid, sterile-appearing | Purulent |
| Infection signs | Absent | Present (fever, otalgia, erythema) |
| TM | Intact, dull, amber; poor mobility | Bulging, erythematous |
| Pain | Absent/mild | Often significant |
| Hearing loss | Conductive | Conductive |
| Primary treatment | Watchful waiting → tubes | Antibiotics (± tubes for rAOM) |
Sources:
- Shambaugh Surgery of the Ear
- Cummings Otolaryngology - Head and Neck Surgery
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2
- Harrison's Principles of Internal Medicine, 22nd ed.
- K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.