Approach to acute liver failure in children
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute liver failure" AND children
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to write a thorough, well-structured response on pediatric acute liver failure. Let me compile everything.
Acute Liver Failure in Children (Pediatric Acute Liver Failure - PALF)
Definition
PALF is defined by:
- Severe hepatic dysfunction within 8 weeks of illness onset
- No underlying chronic liver disease
- Liver-based coagulopathy:
- INR ≥ 1.5 (with hepatic encephalopathy, HE), OR
- INR ≥ 2.0 / PT ≥ 20 (without encephalopathy)
Historically associated with mortality of 70-95%; with modern ICU care and liver transplantation (LT), this has declined to approximately 30%.
- Fischer's Mastery of Surgery, 8th ed.
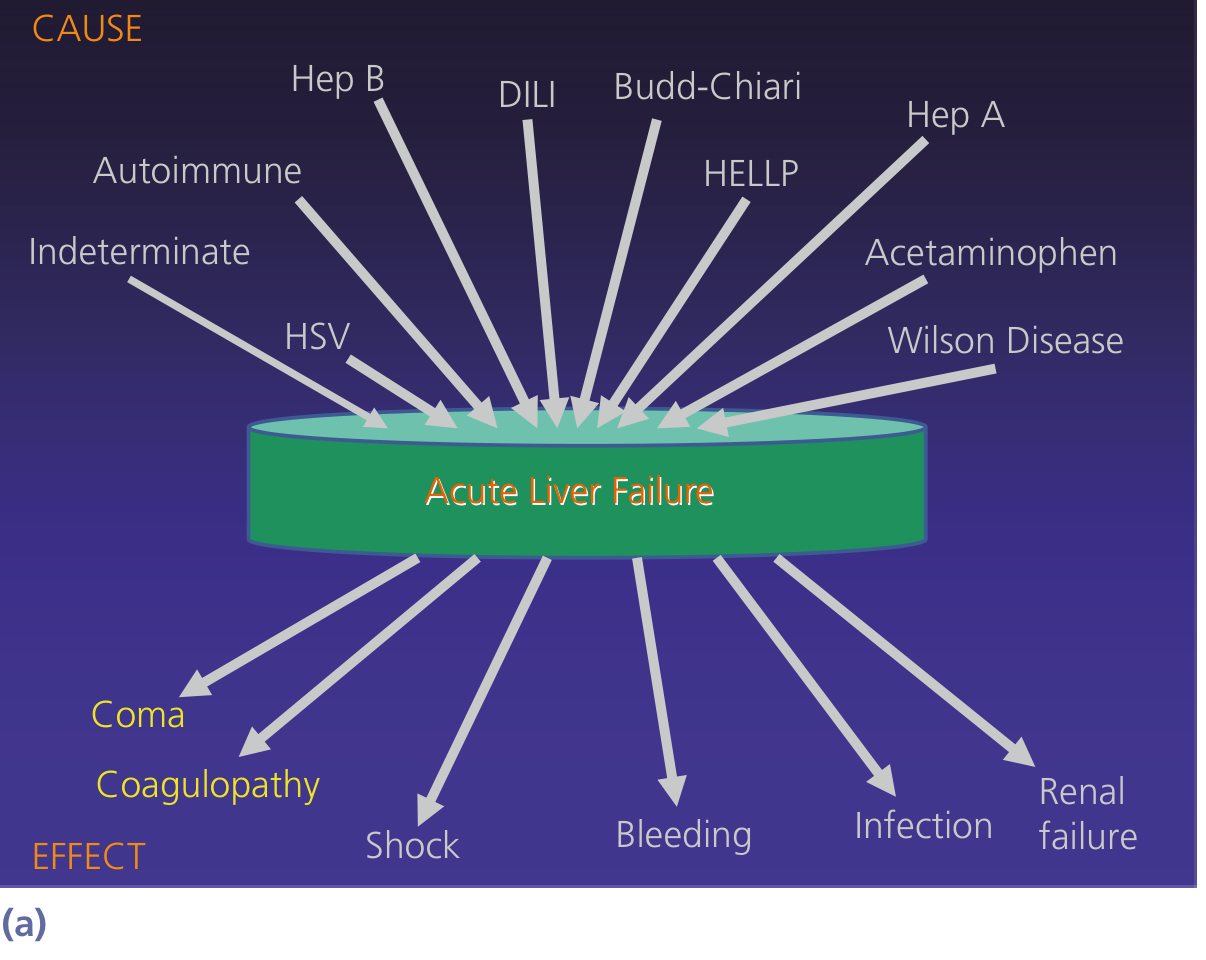
Etiology (Age-Stratified)
The cause is indeterminate in ~50% of PALF cases - a major difference from adult ALF. Known causes vary by age:
| Age Group | Common Causes |
|---|---|
| Neonates / Infants | Neonatal hemochromatosis (gestational alloimmune liver disease), herpes simplex virus (HSV), galactosemia, tyrosinemia, mitochondrial disorders, urea cycle defects |
| Toddlers (1-5 yr) | Acetaminophen toxicity, Wilson disease (less common in young children), autoimmune hepatitis, hepatitis A |
| School-age / Adolescents | Acetaminophen (intentional or unintentional), autoimmune hepatitis, Wilson disease, hepatitis A/B, idiosyncratic DILI |
Other causes across all pediatric ages:
- Valproic acid, salicylates (Reye syndrome)
- Viral: EBV, CMV, parvovirus B19, adenovirus, enterovirus
- Metabolic: organic acidemias (MSUD, propionic acidemia, methylmalonic acidemia), Crigler-Najjar, fatty acid oxidation defects
- Budd-Chiari syndrome (prothrombotic states)
- Malignant infiltration
Bradley and Daroff's Neurology in Clinical Practice; Fischer's Mastery of Surgery, 8th ed.
Clinical Presentation
The classic triad is jaundice + coagulopathy + hepatic encephalopathy. Encephalopathy may be subtle initially - especially in young children - and requires active surveillance.
Hepatic encephalopathy staging in children:
| Stage | Features |
|---|---|
| 1 | Mild confusion, irritability, excessive crying, sleep disturbances, short attention span |
| 2 | Excessive sleepiness, moderate confusion, personality changes, intermittent disorientation |
| 3 | Profound confusion, stupor, delirium, hyperreflexia, extensor plantar response |
| 4a | Coma with response to pain |
| 4b | Coma without response to pain (decerebrate/decorticate posturing) |
- Intracranial hypertension and cerebral edema are invariably present in stage 4, and brainstem herniation is the most common cause of death on post-mortem.
- Seizures occur in 10-30% of patients.
- EEG shows early alpha slowing → delta frequencies → triphasic waves (poor prognosis).
Bradley and Daroff's Neurology in Clinical Practice
Other systemic features:
- Hypotension, vasodilation, low SVR (similar to septic physiology)
- Renal failure (hepatorenal syndrome - reversible with liver recovery)
- Infection: very common, gram-positive organisms predominate
- Metabolic: hypoglycemia, lactic acidosis, coagulopathy
Diagnostic Work-up
Initial labs (urgent):
- LFTs: AST, ALT, bilirubin (typically very elevated)
- PT/INR, aPTT, factor V (factor V is the most sensitive biomarker of trends over time due to its short half-life)
- Serum albumin
- Serum ammonia (arterial preferred)
- BMP: glucose, electrolytes, creatinine, bicarbonate, lactate
- CBC with differential
- Blood gas (metabolic acidosis = poor prognosis in acetaminophen)
Etiology work-up (targeted):
- Viral: HAV IgM, HBsAg/anti-HBc IgM, anti-HEV, HSV PCR/DFA, EBV, CMV, adenovirus, enterovirus
- Metabolic: serum lactate/pyruvate ratio, plasma amino acids, urine organic acids, acylcarnitine profile, alpha-1-antitrypsin, galactose-1-phosphate uridyl transferase
- Wilson disease: serum ceruloplasmin, 24-hr urine copper, slit-lamp exam (Kayser-Fleischer rings), liver copper content; note that ceruloplasmin may be falsely low in ALF from any cause
- Autoimmune: ANA, ASMA, anti-LKM1, IgG levels
- Drug screen: serum acetaminophen level, acetaminophen-protein adducts (research tool - detects unrecognized APAP overdose in ~20% of indeterminate cases)
- Neonatal hemochromatosis: ferritin, transferrin saturation, MRI (extrahepatic iron deposition)
- Neuroimaging: CT/MRI to detect cerebral edema, hemorrhage
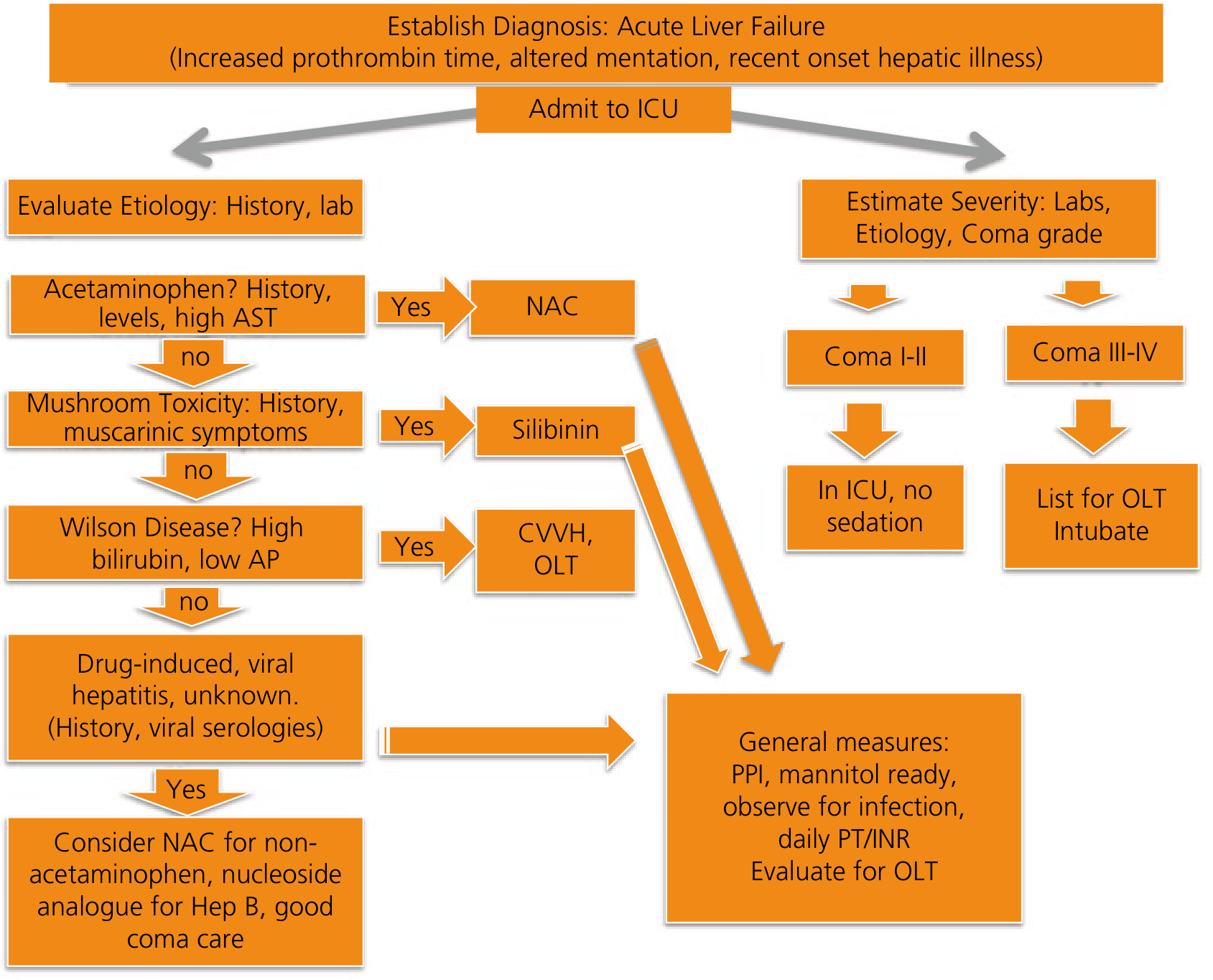
Management
1. General Principles
- Urgent transfer to a pediatric liver transplant center is mandatory once diagnosis is established.
- All patients require ICU-level care.
- Grade any degree of encephalopathy as a trigger for mandatory LT evaluation.
Yamada's Textbook of Gastroenterology, 7th ed.
2. Neurological - Cerebral Edema & Encephalopathy
- Head-of-bed elevation 30°, minimize stimulation, avoid sedation unless intubated
- Ammonia reduction:
- Lactulose, polyethylene glycol (PEG)
- Rifaximin (preferred in children; neomycin as alternative for bowel decontamination)
- L-ornithine-L-aspartate (LOLA)
- Protein restriction (short-term; prolonged restriction is harmful)
- Cerebral edema:
- Fluid restriction
- Hyperosmolar therapy: 3% hypertonic saline or mannitol
- Hyperventilation (short-term, bridge only)
- Target serum Na 145-150 mEq/L (hypernatremia protective against brain edema)
- ICP monitoring: consider in stage 3-4 encephalopathy at experienced centers
- Avoid benzodiazepines (liver cannot metabolize; worsen encephalopathy)
- Flumazenil may transiently reduce HE severity if benzodiazepine exposure occurred
3. Etiology-Specific Therapy
| Etiology | Treatment |
|---|---|
| Acetaminophen | N-acetylcysteine (NAC): 140 mg/kg loading dose IV/PO, then 70 mg/kg q4h |
| Autoimmune hepatitis | IV methylprednisolone (use cautiously - risk of infection; avoid if uncertain) |
| Herpes simplex virus | IV acyclovir (always cover HSV empirically in neonates with ALF) |
| Wilson disease | Copper chelation (D-penicillamine or trientine); albumin dialysis; LT often required |
| Hepatitis B | Nucleos(t)ide analogues (entecavir, tenofovir) |
| Galactosemia | Galactose-free formula immediately |
| Tyrosinemia type 1 | Nitisinone (NTBC) |
NAC beyond acetaminophen: Based on limited data, IV NAC is also commonly used in ALF from idiosyncratic DILI, hepatitis B, autoimmune hepatitis, and indeterminate ALF (especially grade 1-2 HE) given its low risk profile.
- Goldman-Cecil Medicine, International Edition
4. Hemodynamic Support
- IV fluids: avoid over-hydration (worsens cerebral edema); balanced crystalloids preferred
- Vasopressors if needed: norepinephrine first-line
- Correct hypoglycemia aggressively (10% dextrose infusion, target glucose 80-120 mg/dL)
- Packed RBCs as needed; avoid routine FFP (masks coagulopathy used to track prognosis; use only for active bleeding or procedures)
5. Renal & Metabolic Support
- Continuous renal replacement therapy (CRRT) for hepatorenal syndrome or renal failure - also improves ammonia clearance
- Avoid nephrotoxic drugs
- Sodium management: hypernatremia (145-150) for cerebral protection in HE grades 3-4
6. Infection
- Surveillance cultures (blood, urine, tracheal aspirate)
- Low threshold for empiric antibiotics (gram-positive coverage: vancomycin + piperacillin-tazobactam)
- Antifungal prophylaxis with fluconazole in prolonged ICU stay
- HSV and CMV empirical coverage in neonates/infants
7. Nutritional Support
- Early enteral nutrition via NG tube (preferred over TPN)
- Moderate protein restriction short-term (0.5-1 g/kg/day) to reduce ammonia; prolonged restriction worsens outcomes
- High glucose to prevent hypoglycemia
Liver Transplantation
Transfer to transplant center and urgent evaluation is mandatory in all PALF cases. LT listing is a difficult decision given:
- Possibility of spontaneous recovery (especially in autoimmune hepatitis, HAV, indeterminate)
- LT for PALF carries higher mortality than other indications: 1-year patient survival ~73% (vs. ~89% for biliary atresia)
LT listing criteria (various scoring systems used):
- King's College Criteria (originally for adults, adapted for children)
- PALF Study Group criteria
- Etiology is important: acetaminophen ALF has high spontaneous recovery; indeterminate etiology has worst prognosis
Contraindications to urgent listing: active uncontrolled infection, severe hemodynamic instability, multi-organ failure beyond reversibility, underlying malignancy
LT listing for PALF has decreased recently (7.7% in 2020), reflecting improved medical management and better patient selection.
Fischer's Mastery of Surgery, 8th ed.
Prognosis Indicators
Poor prognostic signs:
- INR > 4, bilirubin > 18 mg/dL
- HE grade 3-4
- Rapid progression from HE onset to coma
- Hyperammonemia (arterial NH3 > 150-200 µmol/L)
- Severe metabolic acidosis (pH < 7.3 after fluid resuscitation)
- Renal failure requiring dialysis
- Indeterminate etiology (worst natural history)
- Subacute onset (weeks to onset of HE)
Better prognosis:
- Acetaminophen etiology (high spontaneous recovery)
- HAV etiology
- Younger patients with metabolic disease on specific therapy (NTBC for tyrosinemia)
Special Neonatal Considerations
- Neonatal HSV: empiric IV acyclovir until excluded; mortality is extremely high without treatment
- Neonatal hemochromatosis (gestational alloimmune liver disease, GALD): treat with antioxidant cocktail (NAC, vitamin E, selenium, N-acetylcysteine) + exchange transfusion + IVIG; LT may be required
- Mitochondrial liver disease: NAC, avoid valproate; LT generally contraindicated if extrahepatic disease present
Key Points Summary
- PALF = coagulopathy (INR ≥1.5 with HE; ≥2.0 without) + acute hepatic illness < 8 weeks, no pre-existing liver disease
- Etiology is indeterminate in ~50% of cases - systematic work-up is essential
- Transfer immediately to a pediatric liver transplant center
- ICU care addressing all organ systems simultaneously
- NAC for acetaminophen; consider for indeterminate/DILI/autoimmune; acyclovir for neonatal HSV
- HE management: lactulose, rifaximin, ammonia control, cerebral edema therapy
- LT is life-saving in selected patients; 1-year survival ~73% for PALF after LT
- Factor V and serial INR are the most useful prognostic bedside markers
Recent literature note (2025): A systematic review on recurrent PALF (PMID 41159810, Liver Int 2025) highlights a distinct phenotype with recurrent episodes - often genetic/metabolic etiology - with different long-term outcomes, suggesting genetic work-up in any child with recurrent episodes.
Sources: Fischer's Mastery of Surgery (8th ed.) | Yamada's Textbook of Gastroenterology (7th ed.) | Goldman-Cecil Medicine | Bradley and Daroff's Neurology in Clinical Practice | Miller's Anesthesia (10th ed.) | Robbins Pathology
Slides on Approach to acute liver failure in children
Reading File
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/palf-slides && ls /home/daytona/workspace/palf-slides/
Writing File
~/palf-slides/palf.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Approach to Acute Liver Failure in Children (PALF)";
// ─── PALETTE ────────────────────────────────────────────────────────────────
const C = {
navy: "0B2545", // dominant dark bg
teal: "1B6CA8", // section headers, key shapes
tealLt: "2B8DC8", // lighter accent
gold: "F0A500", // accent / highlight
goldLt: "FFD166", // sub-accent
red: "C0392B", // warning / critical
white: "FFFFFF",
offWhite:"F4F8FB",
grayLt: "D6E4F0",
grayMid: "8BA7C0",
textDark:"0B2545",
};
// ─── HELPERS ────────────────────────────────────────────────────────────────
function addSlide(bg) {
const s = pres.addSlide();
if (bg) s.background = { color: bg };
return s;
}
// Dark header bar + title + subtitle
function sectionHeader(slide, title, subtitle) {
// top bar
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: C.navy }, line: { color: C.navy } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 1.0, w: 10, h: 0.06, fill: { color: C.gold }, line: { color: C.gold } });
slide.addText(title, { x: 0.4, y: 0.08, w: 9.2, h: 0.82, fontSize: 24, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
if (subtitle) {
slide.addText(subtitle, { x: 0.4, y: 1.12, w: 9.2, h: 0.44, fontSize: 13, color: C.teal, fontFace: "Calibri", bold: true, margin: 0 });
}
}
// Bullet card (rounded rect with content)
function addCard(slide, x, y, w, h, title, bullets, titleColor, cardColor) {
cardColor = cardColor || C.white;
titleColor = titleColor || C.navy;
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w, h,
fill: { color: cardColor },
shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.12 },
line: { color: C.grayLt, pt: 1 }
});
if (title) {
slide.addShape(pres.shapes.RECTANGLE, { x, y, w, h: 0.34, fill: { color: titleColor }, line: { color: titleColor } });
slide.addText(title, { x: x + 0.12, y: y + 0.02, w: w - 0.18, h: 0.30, fontSize: 11, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
}
if (bullets && bullets.length > 0) {
const ty = title ? y + 0.38 : y + 0.1;
const th = h - (title ? 0.42 : 0.14);
const items = bullets.map((b, i) => ({
text: b,
options: { bullet: { code: "25B8", color: C.teal }, breakLine: i < bullets.length - 1, fontSize: 10.5, color: C.textDark, fontFace: "Calibri" }
}));
slide.addText(items, { x: x + 0.18, y: ty, w: w - 0.28, h: th, valign: "top", margin: 0 });
}
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE SLIDE
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.navy);
// Decorative side stripe
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.28, h: 5.625, fill: { color: C.gold }, line: { color: C.gold } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 0, w: 0.08, h: 5.625, fill: { color: C.teal }, line: { color: C.teal } });
// Bottom accent bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.1, w: 10, h: 0.525, fill: { color: C.teal }, line: { color: C.teal } });
// Main title
s.addText("Pediatric Acute Liver Failure", {
x: 0.65, y: 1.2, w: 9.0, h: 1.2,
fontSize: 38, bold: true, color: C.white, fontFace: "Calibri",
align: "left", valign: "middle", margin: 0
});
s.addText("(PALF)", {
x: 0.65, y: 2.3, w: 4, h: 0.7,
fontSize: 30, bold: true, color: C.goldLt, fontFace: "Calibri",
align: "left", margin: 0
});
// Subtitle
s.addText("Approach to Diagnosis & Management", {
x: 0.65, y: 3.1, w: 8.5, h: 0.55,
fontSize: 17, color: C.grayLt, fontFace: "Calibri", align: "left", margin: 0
});
// Divider line
s.addShape(pres.shapes.RECTANGLE, { x: 0.65, y: 3.7, w: 5.5, h: 0.04, fill: { color: C.goldLt }, line: { color: C.goldLt } });
// Footer text
s.addText("Pediatric Gastroenterology & Hepatology | Intensive Care", {
x: 0.65, y: 5.13, w: 9, h: 0.38,
fontSize: 11, color: C.white, fontFace: "Calibri", align: "left", margin: 0
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 2 — DEFINITION & DIAGNOSTIC CRITERIA
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Definition & Diagnostic Criteria", "What defines PALF?");
// Central definition box
s.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 1.65, w: 9.4, h: 1.12,
fill: { color: C.navy }, line: { color: C.navy }
});
s.addText([
{ text: "PALF: ", options: { bold: true, color: C.goldLt, fontSize: 13 } },
{ text: "Severe hepatic dysfunction within 8 weeks of illness onset, no pre-existing liver disease, and liver-based coagulopathy", options: { color: C.white, fontSize: 13 } }
], { x: 0.45, y: 1.68, w: 9.1, h: 1.06, valign: "middle", margin: 0 });
// Three criteria cards
const cards = [
{ title: "WITH Encephalopathy", bullets: ["INR ≥ 1.5", "or PT > 15 seconds"] },
{ title: "WITHOUT Encephalopathy", bullets: ["INR ≥ 2.0", "or PT ≥ 20 seconds"] },
{ title: "Time Frame", bullets: ["< 8 weeks illness onset", "No prior liver disease"] },
];
cards.forEach((c, i) => {
addCard(s, 0.3 + i * 3.15, 2.88, 2.95, 1.62, c.title, c.bullets,
i === 0 ? C.red : i === 1 ? C.teal : C.navy);
});
// Historical mortality note
s.addShape(pres.shapes.RECTANGLE, { x: 0.3, y: 4.62, w: 9.4, h: 0.7, fill: { color: C.grayLt }, line: { color: C.grayLt } });
s.addText([
{ text: "Historically: ", options: { bold: true, color: C.red, fontSize: 11.5 } },
{ text: "Mortality 70–95% ", options: { color: C.textDark, fontSize: 11.5 } },
{ text: " | With modern ICU care + transplantation: ", options: { color: C.textDark, fontSize: 11.5 } },
{ text: "~30% mortality today", options: { bold: true, color: C.teal, fontSize: 11.5 } }
], { x: 0.5, y: 4.65, w: 9.0, h: 0.62, valign: "middle", margin: 0 });
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 3 — ETIOLOGY (Age-stratified)
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Etiology of PALF", "Age-stratified causes — etiology is INDETERMINATE in ~50% of cases");
// Age columns
const ages = [
{
label: "Neonates / Infants",
items: ["Gestational alloimmune liver disease (neonatal hemochromatosis)", "Herpes simplex virus (HSV)", "Galactosemia", "Tyrosinemia type 1", "Mitochondrial disorders", "Urea cycle defects"],
color: C.teal
},
{
label: "Toddlers (1–5 yr)",
items: ["Acetaminophen toxicity", "Autoimmune hepatitis", "Hepatitis A / B", "Wilson disease (less common)", "Idiosyncratic DILI", "Viral: EBV, CMV, adenovirus"],
color: C.navy
},
{
label: "School-age / Adolescents",
items: ["Acetaminophen (intentional OD)", "Wilson disease", "Autoimmune hepatitis", "Hepatitis A / B / E", "Idiosyncratic DILI", "Budd-Chiari syndrome"],
color: C.red
},
];
ages.forEach((a, i) => {
const x = 0.28 + i * 3.18;
s.addShape(pres.shapes.RECTANGLE, { x, y: 1.62, w: 3.0, h: 0.38, fill: { color: a.color }, line: { color: a.color } });
s.addText(a.label, { x: x + 0.08, y: 1.64, w: 2.88, h: 0.34, fontSize: 11, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
s.addShape(pres.shapes.RECTANGLE, { x, y: 2.0, w: 3.0, h: 2.82, fill: { color: C.white }, line: { color: C.grayLt, pt: 1 } });
const items = a.items.map((t, ii) => ({
text: t,
options: { bullet: { code: "25CF", color: a.color }, breakLine: ii < a.items.length - 1, fontSize: 10.5, color: C.textDark, fontFace: "Calibri" }
}));
s.addText(items, { x: x + 0.18, y: 2.08, w: 2.72, h: 2.68, valign: "top", margin: 0 });
});
// Footer note
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 4.92, w: 9.44, h: 0.46, fill: { color: C.goldLt }, line: { color: C.goldLt } });
s.addText("⚠ Across ALL ages: valproic acid, salicylates (Reye syndrome), organic acidemias, malignancy, Budd-Chiari, indeterminate", {
x: 0.42, y: 4.94, w: 9.2, h: 0.40, fontSize: 10.5, bold: false, color: C.navy, fontFace: "Calibri", valign: "middle", margin: 0
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 4 — CLINICAL FEATURES & HE STAGING
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Clinical Presentation & Hepatic Encephalopathy Staging", "Classic triad: Jaundice · Coagulopathy · Encephalopathy");
// Left column — features
addCard(s, 0.28, 1.62, 4.0, 1.5, "Systemic Features", [
"Jaundice, dark urine, pale stools",
"Coagulopathy — bleeding, petechiae",
"Hypotension, vasodilation (low SVR)",
"Hypoglycemia, lactic acidosis",
"Renal failure (hepatorenal syndrome)",
"Gram-positive sepsis very common"
], C.teal);
addCard(s, 0.28, 3.22, 4.0, 1.55, "CNS Features in Children", [
"Irritability / excessive crying (early)",
"Asterixis (flapping tremor)",
"Seizures in 10–30%",
"Cerebral edema → herniation (Stage 4)",
"EEG: alpha slowing → delta → triphasic waves",
"CT/MRI: edema, T1 GP hyperintensity"
], C.navy);
// Right column — HE staging table
s.addShape(pres.shapes.RECTANGLE, { x: 4.55, y: 1.62, w: 5.1, h: 0.34, fill: { color: C.navy }, line: { color: C.navy } });
s.addText("Hepatic Encephalopathy Staging (Pediatric Modifications)", { x: 4.62, y: 1.64, w: 4.96, h: 0.30, fontSize: 10.5, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
const heStages = [
{ stage: "Stage 1", color: C.goldLt, desc: "Irritability, excessive crying, sleep disturbances, mild confusion, short attention span" },
{ stage: "Stage 2", color: "FFA040", desc: "Excessive sleepiness, moderate confusion, personality changes, intermittent disorientation" },
{ stage: "Stage 3", color: "FF7043", desc: "Profound confusion, stupor, delirium, hyperreflexia, extensor plantar response" },
{ stage: "Stage 4a", color: "D32F2F", desc: "Coma with response to pain (decerebrate/decorticate posturing)" },
{ stage: "Stage 4b", color: "7B0000", desc: "Coma without any response to pain — imminent herniation risk" },
];
heStages.forEach((h, i) => {
const y = 2.0 + i * 0.62;
s.addShape(pres.shapes.RECTANGLE, { x: 4.55, y, w: 1.18, h: 0.58, fill: { color: h.color }, line: { color: h.color } });
s.addText(h.stage, { x: 4.57, y: y + 0.02, w: 1.14, h: 0.54, fontSize: 10.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
s.addShape(pres.shapes.RECTANGLE, { x: 5.73, y, w: 3.92, h: 0.58, fill: { color: C.white }, line: { color: C.grayLt, pt: 1 } });
s.addText(h.desc, { x: 5.82, y: y + 0.04, w: 3.74, h: 0.50, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "middle", margin: 0 });
});
s.addShape(pres.shapes.RECTANGLE, { x: 4.55, y: 5.12, w: 5.1, h: 0.35, fill: { color: C.red }, line: { color: C.red } });
s.addText("⚠ Stage 4 → Cerebral edema invariably present → Most common cause of death", {
x: 4.62, y: 5.14, w: 4.96, h: 0.30, fontSize: 9.5, color: C.white, bold: true, fontFace: "Calibri", valign: "middle", margin: 0
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 5 — DIAGNOSTIC WORK-UP
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Diagnostic Work-up", "Urgent investigation — etiology guides specific therapy");
const groups = [
{
title: "Liver Function & Severity", color: C.teal,
items: ["LFTs: AST, ALT, bilirubin", "PT / INR / aPTT", "Factor V (most sensitive trend marker)", "Serum albumin", "Arterial ammonia", "Blood gas + lactate, glucose"]
},
{
title: "Infection Screen", color: C.navy,
items: ["HAV IgM, HBsAg + anti-HBc IgM", "HSV PCR / DFA (esp. neonates)", "EBV, CMV, parvovirus B19", "Adenovirus, enterovirus PCR", "Blood + urine cultures", "HEV serology"]
},
{
title: "Metabolic / Genetic", color: C.gold,
items: ["Plasma amino acids, urine organic acids", "Acylcarnitine profile (FAOD)", "Serum lactate : pyruvate ratio", "Galactose-1-PUT (galactosemia)", "Alpha-1-antitrypsin level + phenotype", "Serum ferritin (neonatal hemochromatosis)"]
},
{
title: "Wilson Disease", color: "6A0D83",
items: ["Serum ceruloplasmin (may be falsely low in ALF)", "24-hr urine copper", "Slit-lamp exam (KF rings)", "Liver biopsy copper content"]
},
{
title: "Autoimmune / Other", color: C.red,
items: ["ANA, ASMA, anti-LKM1, IgG", "Anti-SLA, anti-LC1", "APAP-protein adducts (if indeterminate)", "Doppler USS / MRI (Budd-Chiari)", "Bone marrow biopsy (malignancy)"]
},
];
// Two-row layout: 3 + 2
[0, 1, 2].forEach((i) => {
addCard(s, 0.22 + i * 3.25, 1.62, 3.08, 2.0, groups[i].title, groups[i].items, groups[i].color);
});
[3, 4].forEach((j) => {
addCard(s, 0.22 + j * 4.9 - 4.9 * 0.5 + 0.8, 3.74, 3.7, 1.72, groups[j].title, groups[j].items, groups[j].color);
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 6 — IMMEDIATE MANAGEMENT (ICU)
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Immediate Management", "ALL patients → ICU | Transfer to Pediatric Liver Transplant Center");
// Emergency banner
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 1.62, w: 9.44, h: 0.44, fill: { color: C.red }, line: { color: C.red } });
s.addText("⚡ Transfer to a pediatric liver transplant center URGENTLY — mandatory for all PALF cases", {
x: 0.4, y: 1.63, w: 9.2, h: 0.40, fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0
});
const pillars = [
{
title: "Neurological", color: C.navy,
items: ["HOB 30°, minimize stimulation", "Lactulose / rifaximin (ammonia ↓)", "3% NaCl or mannitol (cerebral edema)", "Target Na 145–150 mEq/L", "ICP monitoring: Stage 3–4 HE", "Avoid sedatives / benzodiazepines"]
},
{
title: "Hemodynamic", color: C.teal,
items: ["Balanced crystalloid resuscitation", "Norepinephrine (vasopressors PRN)", "Continuous glucose 10% (target 80–120)", "Avoid FFP (masks coagulopathy marker)", "Correct coags only for active bleeding / procedures"]
},
{
title: "Renal / Metabolic", color: "7B3F00",
items: ["CRRT for AKI / HRS", "CRRT also aids ammonia clearance", "Correct electrolytes (K, Mg, Phos)", "Monitor for lactic acidosis"]
},
{
title: "Infection", color: C.red,
items: ["Empiric: vancomycin + pip-tazo", "Antifungal prophylaxis (fluconazole)", "HSV empiric acyclovir in neonates", "Surveillance cultures q48–72h", "Avoid aminoglycosides (nephrotoxic)"]
},
{
title: "Nutrition", color: "2E7D32",
items: ["Early enteral feeding (NGT)", "Short-term protein restriction 0.5–1 g/kg/day", "High dextrose (prevent hypoglycemia)", "Avoid prolonged protein restriction"]
},
];
[0,1,2,3,4].forEach((i) => {
const row = i < 3 ? 0 : 1;
const col = i < 3 ? i : i - 3;
const xBase = row === 0 ? 0.22 + col * 3.25 : 0.22 + col * 4.9;
const w = row === 0 ? 3.08 : 3.7;
addCard(s, xBase, 2.2 + row * 1.72, w, 1.6, pillars[i].title, pillars[i].items, pillars[i].color);
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 7 — ETIOLOGY-SPECIFIC THERAPY
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Etiology-Specific Therapy", "Targeted treatment is key — always identify the underlying cause");
// NAC banner
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 1.62, w: 9.44, h: 0.68, fill: { color: C.teal }, line: { color: C.teal } });
s.addText([
{ text: "N-Acetylcysteine (NAC): ", options: { bold: true, color: C.goldLt, fontSize: 13 } },
{ text: "Loading 140 mg/kg IV/PO → 70 mg/kg q4h. Use for: APAP toxicity (definite), DILI, Hep B, autoimmune, indeterminate (grade 1–2 HE)", options: { color: C.white, fontSize: 12 } }
], { x: 0.42, y: 1.64, w: 9.2, h: 0.62, valign: "middle", margin: 0 });
// Table
const rows = [
["Acetaminophen overdose", "N-Acetylcysteine (NAC) — loading + maintenance", C.goldLt],
["Autoimmune hepatitis", "IV methylprednisolone (cautiously; risk infection)", C.white],
["Herpes simplex virus", "IV Acyclovir — empiric in all neonates with ALF", C.goldLt],
["Wilson disease", "D-penicillamine / trientine; albumin dialysis; LT often needed", C.white],
["Hepatitis B", "Entecavir or tenofovir (nucleos(t)ide analogue)", C.goldLt],
["Galactosemia", "Galactose-free formula — immediately", C.white],
["Tyrosinemia type 1", "Nitisinone (NTBC) — start urgently", C.goldLt],
["Neonatal hemochromatosis", "IVIG + exchange transfusion + antioxidant cocktail (NAC, vit E, selenium)", C.white],
["Budd-Chiari", "Anticoagulation; interventional shunt; consider LT", C.goldLt],
];
// Table header
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 2.38, w: 4.6, h: 0.36, fill: { color: C.navy }, line: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 4.88, y: 2.38, w: 4.84, h: 0.36, fill: { color: C.navy }, line: { color: C.navy } });
s.addText("Etiology", { x: 0.32, y: 2.40, w: 4.52, h: 0.30, fontSize: 10.5, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
s.addText("Treatment", { x: 4.92, y: 2.40, w: 4.76, h: 0.30, fontSize: 10.5, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
rows.forEach((r, i) => {
const y = 2.74 + i * 0.30;
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y, w: 4.6, h: 0.29, fill: { color: r[2] }, line: { color: C.grayLt, pt: 0.5 } });
s.addShape(pres.shapes.RECTANGLE, { x: 4.88, y, w: 4.84, h: 0.29, fill: { color: r[2] }, line: { color: C.grayLt, pt: 0.5 } });
s.addText(r[0], { x: 0.36, y: y + 0.02, w: 4.44, h: 0.26, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", bold: true, valign: "middle", margin: 0 });
s.addText(r[1], { x: 4.94, y: y + 0.02, w: 4.70, h: 0.26, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "middle", margin: 0 });
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 8 — CEREBRAL EDEMA MANAGEMENT
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Management of Cerebral Edema & Raised ICP", "Leading cause of death in Stage 4 HE — anticipate and prevent");
// Mechanism box
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 1.62, w: 9.44, h: 0.54, fill: { color: C.navy }, line: { color: C.navy } });
s.addText([
{ text: "Mechanism: ", options: { bold: true, color: C.goldLt, fontSize: 12 } },
{ text: "Ammonia → astrocyte swelling (glutamine accumulation) → cytotoxic edema → raised ICP → herniation. NOT from portal hypertension.", options: { color: C.white, fontSize: 11.5 } }
], { x: 0.42, y: 1.63, w: 9.2, h: 0.50, valign: "middle", margin: 0 });
const steps = [
{ num: "1", title: "Head Positioning", detail: "HOB 30°, midline head, avoid hip flexion > 30°, minimize stimulation", color: C.teal },
{ num: "2", title: "Hypernatremia Target", detail: "Target serum Na 145–150 mEq/L using 3% hypertonic saline (prophylactic / therapeutic)", color: C.teal },
{ num: "3", title: "Mannitol", detail: "0.5–1 g/kg IV bolus for acute ICP spikes. Avoid if serum osmolality > 320 mOsm/L or renal failure", color: C.navy },
{ num: "4", title: "Hyperventilation", detail: "Short-term bridge only — target PaCO₂ 30–35 mmHg. Not for sustained use (causes cerebral vasoconstriction)", color: "7B3F00" },
{ num: "5", title: "ICP Monitoring", detail: "Consider epidural or intraparenchymal monitor in Stage 3–4 HE at experienced transplant centers", color: "6A0D83" },
{ num: "6", title: "Avoid", detail: "Sedatives / BZDs, fever (increases ICP), excessive IV fluids, hypoxemia, hypercapnia", color: C.red },
];
steps.forEach((st, i) => {
const col = i % 3;
const row = Math.floor(i / 3);
const x = 0.28 + col * 3.22;
const y = 2.28 + row * 1.55;
// Number circle
s.addShape(pres.shapes.ELLIPSE, { x: x, y: y, w: 0.42, h: 0.42, fill: { color: st.color }, line: { color: st.color } });
s.addText(st.num, { x: x, y: y, w: 0.42, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
s.addShape(pres.shapes.RECTANGLE, { x: x + 0.46, y, w: 2.65, h: 0.42, fill: { color: st.color }, line: { color: st.color } });
s.addText(st.title, { x: x + 0.50, y: y, w: 2.58, h: 0.42, fontSize: 10.5, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
s.addShape(pres.shapes.RECTANGLE, { x, y: y + 0.44, w: 3.11, h: 1.06, fill: { color: C.white }, line: { color: C.grayLt, pt: 1 } });
s.addText(st.detail, { x: x + 0.1, y: y + 0.48, w: 2.92, h: 0.96, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 9 — LIVER TRANSPLANTATION
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Liver Transplantation in PALF", "Life-saving but difficult listing decision — evaluate ALL patients");
// Key stats
const stats = [
{ val: "~30%", label: "Current PALF\nMortality (w/ LT)" },
{ val: "73%", label: "1-yr Patient Survival\nafter LT for PALF" },
{ val: "7.7%", label: "LT Listing Rate\nfor PALF (2020)" },
{ val: "~50%", label: "Indeterminate\nEtiology" },
];
stats.forEach((st, i) => {
s.addShape(pres.shapes.RECTANGLE, { x: 0.28 + i * 2.42, y: 1.62, w: 2.22, h: 1.22,
fill: { color: i % 2 === 0 ? C.navy : C.teal }, line: { color: i % 2 === 0 ? C.navy : C.teal } });
s.addText(st.val, { x: 0.28 + i * 2.42, y: 1.64, w: 2.22, h: 0.72, fontSize: 28, bold: true, color: C.goldLt, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
s.addText(st.label, { x: 0.28 + i * 2.42, y: 2.3, w: 2.22, h: 0.52, fontSize: 9.5, color: C.white, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
});
addCard(s, 0.28, 2.98, 4.62, 2.44, "Indications / When to List", [
"Stage 3–4 encephalopathy with worsening trajectory",
"INR > 4, rapidly rising bilirubin",
"Renal failure + ammonia > 150 µmol/L",
"Wilson disease (most require LT)",
"DILI not responding to NAC",
"Indeterminate etiology — worst prognosis",
"Metabolic disease unresponsive to medical Rx"
], C.teal);
addCard(s, 5.10, 2.98, 4.62, 2.44, "Contraindications / Cautions", [
"Active uncontrolled systemic sepsis",
"Multi-organ failure beyond reversibility",
"Underlying mitochondrial disease (extrahepatic)",
"Brain death / irreversible CNS injury",
"Acetaminophen-induced (high spontaneous recovery — avoid rushing to list)",
"HAV etiology — favorable natural history"
], C.red);
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 10 — PROGNOSTIC INDICATORS
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Prognostic Indicators", "Serial monitoring is key — factor V & INR are best bedside prognostic markers");
addCard(s, 0.28, 1.62, 4.62, 3.62, "Poor Prognosis", [
"INR > 4 or rapidly rising",
"Serum bilirubin > 18 mg/dL",
"Arterial ammonia > 150–200 µmol/L",
"HE grade 3–4",
"Severe metabolic acidosis (pH < 7.3 post-resuscitation)",
"Renal failure requiring dialysis",
"Indeterminate or subacute etiology",
"Age < 1 year (neonatal PALF)",
"Rapid progression: jaundice → coma < 7 days",
"EEG: triphasic waves"
], C.red);
addCard(s, 5.10, 1.62, 4.62, 3.62, "Favorable Prognosis", [
"Acetaminophen etiology (high spontaneous recovery)",
"Hepatitis A etiology",
"HE grade 1–2 at presentation",
"INR improving over 48–72 hours",
"Tyrosinemia responding to nitisinone (NTBC)",
"Autoimmune hepatitis (partial steroid response)",
"Factor V > 25% of normal",
"Rising factor V over serial measurements",
"Young child with known metabolic disease on specific Rx"
], "2E7D32");
// Footer
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 5.3, w: 9.44, h: 0.2, fill: { color: C.grayLt }, line: { color: C.grayLt } });
s.addText("King's College Criteria (adapted) and PALF Study Group scores are used to guide listing decisions alongside clinical judgment", {
x: 0.4, y: 5.32, w: 9.2, h: 0.2, fontSize: 9, color: C.grayMid, fontFace: "Calibri", valign: "middle", margin: 0
});
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 11 — SPECIAL CONSIDERATIONS: NEONATES
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.offWhite);
sectionHeader(s, "Special Considerations: Neonatal ALF", "Different etiology spectrum — unique diagnostic & treatment approaches");
const nCards = [
{
title: "Neonatal HSV",
color: C.red,
items: [
"Always empiric IV acyclovir until excluded",
"20 mg/kg IV q8h",
"HSV PCR: blood, CSF, skin swab",
"Mortality near 100% if untreated",
"Present: vesicles, seizures, coagulopathy, fever (or hypothermia)"
]
},
{
title: "Gestational Alloimmune Liver Disease (GALD / Neonatal Hemochromatosis)",
color: C.navy,
items: [
"Maternal IgG crosses placenta → fetal hepatocyte injury",
"Dx: MRI (extrahepatic siderosis), ferritin, buccal biopsy",
"Rx: IVIG + exchange transfusion + antioxidant cocktail",
"(NAC + vitamin E + selenium + N-acetylcysteine)",
"LT if no response to medical therapy"
]
},
{
title: "Mitochondrial Liver Disease",
color: "7B3F00",
items: [
"POLG mutations, respiratory chain defects",
"Clue: lactic acidosis, elevated lactate:pyruvate ratio",
"Avoid valproic acid",
"NAC supportive",
"LT generally contraindicated if extrahepatic disease present",
"Genetic / electron transport chain testing"
]
},
];
nCards.forEach((c, i) => {
addCard(s, 0.28 + i * 3.22, 1.62, 3.08, 3.72, c.title, c.items, c.color);
});
// Summary note
s.addShape(pres.shapes.RECTANGLE, { x: 0.28, y: 5.42, w: 9.44, h: 0.1, fill: { color: C.gold }, line: { color: C.gold } });
}
// ═══════════════════════════════════════════════════════════════════════════
// SLIDE 12 — SUMMARY / KEY TAKEAWAYS
// ═══════════════════════════════════════════════════════════════════════════
{
const s = addSlide(C.navy);
// Decorative elements
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.06, fill: { color: C.gold }, line: { color: C.gold } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.565, w: 10, h: 0.06, fill: { color: C.gold }, line: { color: C.gold } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.06, w: 0.28, h: 5.505, fill: { color: C.teal }, line: { color: C.teal } });
s.addText("Key Takeaways", {
x: 0.55, y: 0.15, w: 9.0, h: 0.62,
fontSize: 24, bold: true, color: C.goldLt, fontFace: "Calibri", margin: 0
});
const points = [
["1", "PALF = coagulopathy (INR ≥1.5 with HE; ≥2.0 without) + acute hepatic illness < 8 wks, no pre-existing liver disease"],
["2", "Etiology is INDETERMINATE in ~50% — systematic work-up is mandatory in every case"],
["3", "Transfer IMMEDIATELY to a pediatric liver transplant center — do not delay"],
["4", "ICU care addressing all organ systems: neuro, hemodynamic, renal, infectious, nutritional"],
["5", "NAC for APAP; acyclovir for HSV (esp. neonates); disease-specific therapy always first-line"],
["6", "Hepatic encephalopathy monitoring is critical — cerebral edema + herniation is the leading cause of death"],
["7", "Liver transplant is life-saving in selected patients — LT decision requires early parallel evaluation"],
["8", "Serial INR + factor V are the most useful bedside prognostic markers"],
];
points.forEach((p, i) => {
const y = 0.88 + i * 0.58;
s.addShape(pres.shapes.ELLIPSE, { x: 0.42, y: y, w: 0.38, h: 0.38, fill: { color: C.gold }, line: { color: C.gold } });
s.addText(p[0], { x: 0.42, y: y, w: 0.38, h: 0.38, fontSize: 11, bold: true, color: C.navy, fontFace: "Calibri", align: "center", valign: "middle", margin: 0 });
s.addText(p[1], { x: 0.9, y: y + 0.02, w: 8.8, h: 0.36, fontSize: 11, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
});
}
// ─── WRITE FILE ──────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/palf-slides/PALF_Approach_Children.pptx" })
.then(() => console.log("SUCCESS: PALF_Approach_Children.pptx created"))
.catch(err => { console.error("ERROR:", err); process.exit(1); });
Running Command
cd /home/daytona/workspace/palf-slides && node palf.js
Reading File
Editing File
~/palf-slides/palf.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/palf-slides/palf.js'
Searching Content
"pres.shapes.ELLIPSE" in ~/palf-slides
Searching Content
"pres.shapes.ELLIPSE" in ~/palf-slides
Editing File
~/palf-slides/palf.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/palf-slides/palf.js'
Running Command
cd /home/daytona/workspace/palf-slides && node palf.js
Running Command
ls -lh /home/daytona/workspace/palf-slides/PALF_Approach_Children.pptx
Your presentation is ready!
PALF Approach Children
Presentation · PPTX
12 slides covering the full clinical approach, with a navy/teal/gold color scheme:
| Slide | Content |
|---|---|
| 1 | Title slide |
| 2 | Definition & Diagnostic Criteria (INR thresholds, historical mortality) |
| 3 | Etiology - age-stratified table (neonate / toddler / adolescent) |
| 4 | Clinical Presentation + HE Staging (pediatric-modified grading table) |
| 5 | Diagnostic Work-up (5 category cards: LFTs, infection, metabolic, Wilson, autoimmune) |
| 6 | Immediate ICU Management (5 pillars: neuro, hemodynamic, renal, infection, nutrition) |
| 7 | Etiology-Specific Therapy (NAC dosing banner + treatment table for 9 causes) |
| 8 | Cerebral Edema Management (mechanism + 6-step protocol) |
| 9 | Liver Transplantation (stats, indications, contraindications) |
| 10 | Prognostic Indicators (poor vs. favorable prognosis cards) |
| 11 | Special Considerations - Neonatal ALF (HSV, GALD, mitochondrial disease) |
| 12 | Key Takeaways (8-point summary on dark background) |
Approach to acute liver failure in children
I covered this topic in detail just a few minutes ago. Here's a concise recap — let me know if you want me to go deeper on any specific section.
Approach to Acute Liver Failure in Children (PALF)
Definition
PALF requires all three:
- Acute hepatic illness < 8 weeks duration
- No pre-existing liver disease
- Liver-based coagulopathy:
- INR ≥ 1.5 with encephalopathy, OR
- INR ≥ 2.0 / PT ≥ 20 without encephalopathy
Mortality has fallen from 70-95% historically to ~30% with modern ICU care and liver transplantation.
Etiology (Age-Stratified)
| Age | Key Causes |
|---|---|
| Neonates | HSV, gestational alloimmune liver disease (GALD/neonatal hemochromatosis), galactosemia, tyrosinemia, mitochondrial disease, urea cycle defects |
| Toddlers 1-5 yr | Acetaminophen, autoimmune hepatitis, HAV/HBV, Wilson disease, idiosyncratic DILI, viral (EBV, CMV, adenovirus) |
| School-age / Teens | Acetaminophen (intentional OD), Wilson disease, autoimmune hepatitis, HAV/HBV/HEV, DILI |
| All ages | Valproic acid, Reye syndrome (salicylates), organic acidemias, Budd-Chiari, malignancy |
Etiology remains indeterminate in ~50% of PALF cases - the most important single epidemiological fact.
Clinical Presentation
Classic triad: Jaundice + Coagulopathy + Hepatic Encephalopathy
Hepatic Encephalopathy Staging (Pediatric)
| Stage | Features |
|---|---|
| 1 | Irritability, excessive crying, sleep disturbance, mild confusion |
| 2 | Excessive sleepiness, moderate confusion, personality change, intermittent disorientation |
| 3 | Stupor, profound confusion, delirium, hyperreflexia, extensor plantar response |
| 4a | Coma with pain response |
| 4b | Coma without any pain response - imminent herniation |
Other features: hypoglycemia, metabolic acidosis, hypotension (low SVR), gram-positive sepsis, hepatorenal syndrome, seizures (10-30%), cerebral edema (invariable at Stage 4 - leading cause of death).
Diagnostic Work-up
Urgency and severity markers:
- PT/INR, factor V (most sensitive trend marker - shortest half-life)
- Serum albumin, bilirubin, AST/ALT
- Arterial ammonia, blood gas + lactate, glucose
- CBC, BMP, creatinine
Etiology-directed (run simultaneously):
- Viral: HAV IgM, HBsAg/anti-HBc IgM, HEV; HSV PCR (esp. neonates); EBV, CMV, adenovirus
- Metabolic: plasma amino acids, urine organic acids, acylcarnitine profile, lactate:pyruvate ratio, galactose-1-phosphate uridyl transferase
- Wilson disease: ceruloplasmin (may be falsely low), 24-hr urine copper, slit-lamp exam (KF rings)
- Autoimmune: ANA, ASMA, anti-LKM1, IgG
- Neonatal HC: ferritin, MRI (extrahepatic iron), buccal biopsy
- APAP adducts: detects occult acetaminophen toxicity in ~20% of "indeterminate" cases
- Imaging: liver Doppler USS (Budd-Chiari), CT/MRI brain (edema, hemorrhage)
Management
Step 1 - Transfer Immediately
All PALF patients must be transferred to a pediatric liver transplant center. Any degree of encephalopathy mandates LT evaluation in parallel with medical management.
Step 2 - ICU Supportive Care
Neurological / Cerebral Edema:
- Head of bed 30°, minimize stimulation
- Ammonia reduction: lactulose, rifaximin, L-ornithine-L-aspartate (LOLA)
- Cerebral edema: 3% hypertonic saline (target Na 145-150 mEq/L), mannitol 0.5-1 g/kg IV
- Hyperventilation only as short-term bridge (PaCO₂ 30-35 mmHg)
- ICP monitoring in Stage 3-4 at experienced centers
- Avoid benzodiazepines and sedatives
Hemodynamic:
- Balanced crystalloids; vasopressors (norepinephrine first-line)
- 10% dextrose infusion - target glucose 80-120 mg/dL
- Avoid routine FFP (masks prognosis); use only for active bleeding or procedures
Renal:
- CRRT for AKI/hepatorenal syndrome - also clears ammonia
- Avoid nephrotoxic agents
Infection:
- Empiric: vancomycin + piperacillin-tazobactam
- Antifungal prophylaxis: fluconazole
- Empiric acyclovir in all neonates/infants until HSV excluded
- Surveillance cultures q48-72h
Nutrition:
- Early enteral feeding (NGT preferred)
- Short-term moderate protein restriction (0.5-1 g/kg/day); prolonged restriction is harmful
Step 3 - Etiology-Specific Treatment
| Cause | Treatment |
|---|---|
| Acetaminophen | NAC: 140 mg/kg loading → 70 mg/kg q4h IV/PO |
| Autoimmune hepatitis | IV methylprednisolone (cautious - infection risk) |
| HSV | IV acyclovir 20 mg/kg q8h - empiric in neonates |
| Wilson disease | D-penicillamine / trientine + albumin dialysis; LT usually needed |
| Hepatitis B | Entecavir or tenofovir |
| Galactosemia | Galactose-free formula immediately |
| Tyrosinemia type 1 | Nitisinone (NTBC) urgently |
| GALD/Neonatal HC | IVIG + exchange transfusion + antioxidant cocktail |
| Budd-Chiari | Anticoagulation, interventional shunt, ± LT |
NAC beyond APAP: Also used in idiosyncratic DILI, hepatitis B, autoimmune, and indeterminate ALF (especially grades 1-2 HE) given low risk profile.
Liver Transplantation
Indications to list:
- HE grade 3-4 with worsening trajectory
- INR > 4, rapidly rising bilirubin
- Renal failure + severe hyperammonemia (NH₃ > 150-200 µmol/L)
- Wilson disease, DILI unresponsive to NAC, indeterminate etiology
- 1-year post-LT patient survival for PALF: ~73% (lower than other indications)
- LT listing rate for PALF has declined (7.7% in 2020) reflecting better medical management
Relative contraindications: Active uncontrolled sepsis, brain death/irreversible CNS injury, extrahepatic mitochondrial disease, unresectable malignancy.
Good natural history (caution before listing): Acetaminophen-induced, HAV, autoimmune hepatitis partially responding to steroids.
Prognostic Markers
| Poor Prognosis | Favorable Prognosis |
|---|---|
| INR > 4, rising factor V absent | Acetaminophen etiology |
| Ammonia > 150-200 µmol/L | HAV etiology |
| HE Grade 3-4 | HE Grade 1-2 |
| pH < 7.3 post-resuscitation | INR improving at 48-72h |
| Renal failure on dialysis | Factor V > 25% or rising |
| Indeterminate / subacute etiology | Specific metabolic disease on targeted Rx |
| EEG triphasic waves | Young child with known treatable cause |
Neonatal ALF - Special Notes
- HSV: empiric IV acyclovir until excluded - near 100% mortality untreated
- GALD: maternal IgG-mediated fetal hepatocyte injury - diagnose with MRI + buccal biopsy; treat with IVIG + exchange transfusion
- Mitochondrial disease: avoid valproate; LT generally contraindicated if extrahepatic involvement present
Sources: Fischer's Mastery of Surgery (8th ed.) | Yamada's Textbook of Gastroenterology (7th ed.) | Goldman-Cecil Medicine | Bradley and Daroff's Neurology in Clinical Practice
I don’t need summary i need detail study
Finding Sources
Finding Sources
Searching PubMed
"pediatric acute liver failure" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is the comprehensive, detailed study on pediatric acute liver failure:
Pediatric Acute Liver Failure (PALF) - Detailed Study
SECTION 1: DEFINITION & CLASSIFICATION
Standard Definition (AASLD / PALF Study Group)
Pediatric acute liver failure (PALF) is defined as a clinical syndrome meeting ALL of the following:
- Acute hepatic illness - no prior evidence of liver disease
- Liver-based coagulopathy (not correctable by vitamin K alone):
- INR ≥ 1.5 if hepatic encephalopathy (HE) is present
- INR ≥ 2.0 (or PT ≥ 20 seconds) if HE is absent
- Illness duration < 8 weeks from onset of symptoms
Note: The AASLD adult definition allows up to 26 weeks. Pediatric definitions are stricter (8 weeks) because neonates and children with Wilson disease, autoimmune hepatitis, and certain metabolic diseases often have unrecognized pre-existing liver disease that must be excluded clinically.
The presence of any degree of mental alteration is sufficient for the encephalopathy criterion - it does not need to be advanced coma.
Subclassification by Time Course
This classification predates "PALF" but remains clinically relevant:
| Type | Time: Symptom Onset to Encephalopathy | Features |
|---|---|---|
| Hyperacute | < 7 days | Acetaminophen, ischemia. High cerebral edema risk. Paradoxically better prognosis with treatment |
| Acute | 7-21 days | Hepatitis A, HBV |
| Subacute (Subfulminant) | 21 days to 8 weeks | Idiosyncratic DILI, indeterminate. Portal hypertension more common. Worst transplant-free survival |
Key point: Shorter time from onset to encephalopathy correlates with greater cerebral edema risk; longer duration correlates with greater portal hypertension. Etiology is a more reliable outcome predictor than timing.
Yamada's Textbook of Gastroenterology, 7th ed. | Sabiston Textbook of Surgery
SECTION 2: EPIDEMIOLOGY
- PALF is rare - approximately 2,000 cases per year in the USA total (adults + children)
- In the pretransplant era: mortality exceeded 90%
- With modern ICU care + liver transplantation: current mortality ~30%
- Annual incidence in developed countries: < 10 cases per million population
- ~50% of PALF cases have indeterminate etiology - the single most important epidemiological feature distinguishing PALF from adult ALF (where acetaminophen accounts for ~46%)
- PALF commands clinical attention disproportionate to its frequency because it:
- Affects young patients
- Carries high resource utilization
- Can be reversible with correct management
- Requires immediate transplant center involvement
Yamada's Textbook of Gastroenterology, 7th ed. | Bailey and Love's Surgery, 28th ed.
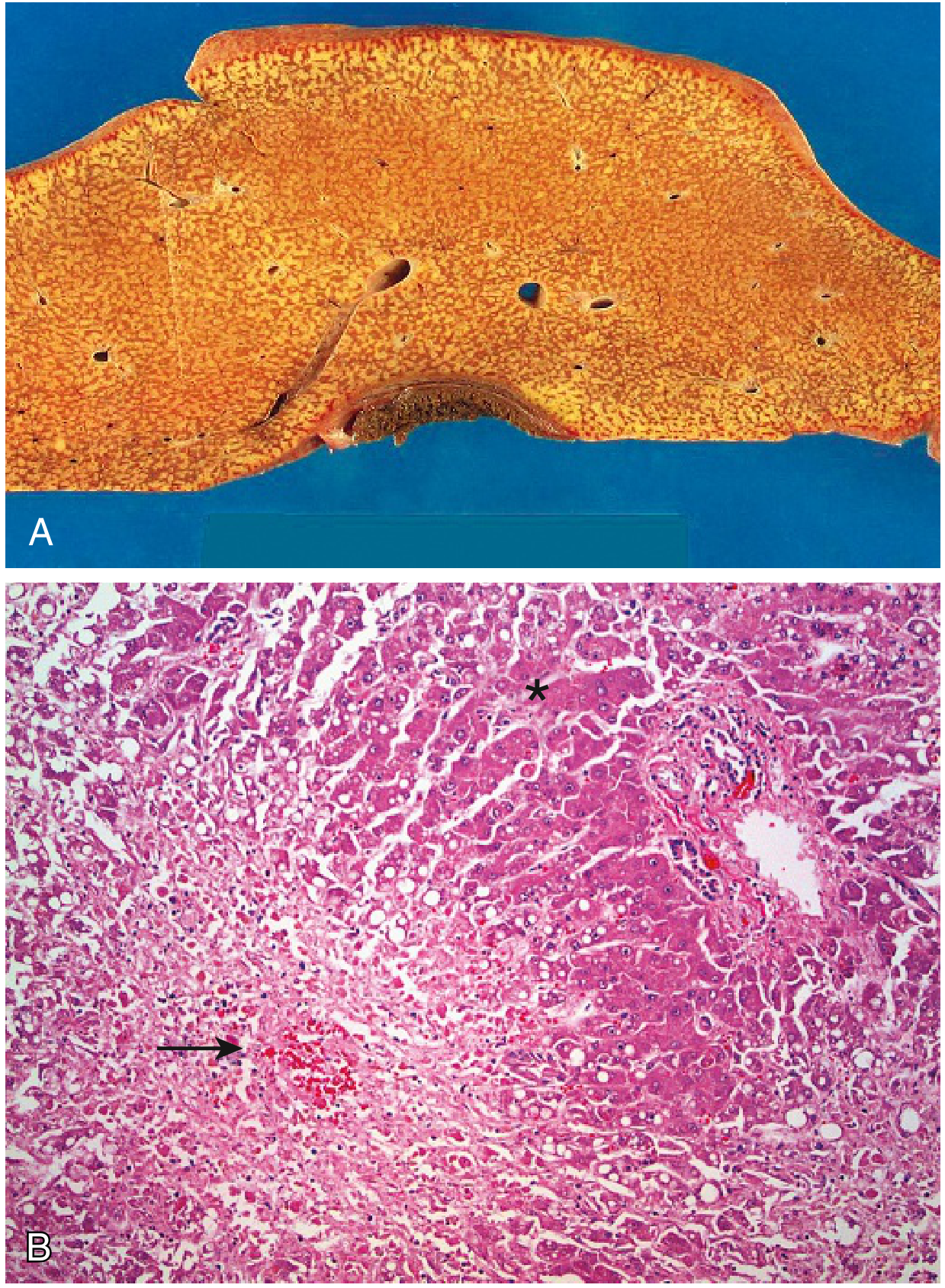
SECTION 2: PATHOPHYSIOLOGY
Mechanism of Hepatocyte Death
Regardless of cause, the final pathway is massive hepatic necrosis:
Gross pathology: The liver is small and shrunken due to loss of parenchyma (can weigh as little as 700g).
Histology (Robbins Pathology):
- Large zones of confluent necrosis surrounding occasional islands of regenerating hepatocytes
- In acetaminophen toxicity: perivenular (zone 3) necrosis - where CYP2E1 is concentrated
- Minimal scarring (acute process - no time for fibrosis)
- Minimal inflammation (hepatocytes die faster than inflammatory response develops)
Consequences of Massive Hepatocyte Loss
| Function Lost | Consequence |
|---|---|
| Coagulation factor synthesis | Coagulopathy (all factors except VIII are liver-derived) |
| Ammonia detoxification (urea cycle) | Hyperammonemia |
| Gluconeogenesis + glycogen storage | Hypoglycemia |
| Bilirubin conjugation + excretion | Jaundice |
| Drug metabolism | Drug toxicity, prolonged sedative effects |
| Immune defense (Kupffer cells) | Susceptibility to gram-positive sepsis |
| Cytokine processing | Systemic inflammatory response, vasodilation |
The Ammonia-Cerebral Edema Cascade
This is the dominant mechanism of death in PALF:
- Gut bacteria and enterocytes produce ammonia via glutamine metabolism
- Normally, portal blood carries ammonia to the liver → metabolized in the urea cycle
- In liver failure: urea cycle fails → ammonia enters systemic circulation
- In the CNS: ammonia is taken up by astrocytes → converted to glutamine (osmotically active)
- Glutamine accumulation → astrocyte swelling → cytotoxic (cellular) cerebral edema
- Elevated intracranial pressure (ICP) → reduced cerebral perfusion pressure → brain ischemia
- Uncal herniation through the falx → brainstem compression → death
Important distinction: In chronic liver disease (cirrhosis), cerebral edema does NOT develop because the process is gradual and adaptive mechanisms exist. In ALF, the edema develops rapidly and is cytotoxic (not vasogenic), making it more severe and harder to treat.
- Cerebral edema develops in ~80% of patients reaching grade 4 HE
- It is the most common cause of death in ALF (>50% of ALF mortality)
- Arterial ammonia > 150-200 µmol/L is associated with increased risk of cerebral herniation
Robbins Pathology | Goldman-Cecil Medicine | Current Surgical Therapy 14th ed.
Hemodynamic Changes
ALF produces a hemodynamic state resembling hyperdynamic sepsis:
- High cardiac output with low systemic vascular resistance (SVR)
- Warm extremities, bounding pulse, low blood pressure
- Splanchnic vasodilation (mediated by nitric oxide, prostacyclin)
- Reactive renal vasoconstriction → sets the stage for hepatorenal syndrome
Coagulopathy Mechanism
- Liver synthesizes all coagulation factors except Factor VIII (which is also produced by vascular endothelium)
- Factor VII has the shortest half-life (~4-6 hours) → first to fall
- Factor V has the next shortest half-life (~12 hours) → most useful for trend monitoring
- Paradox of coagulopathy in ALF: While PT/INR is prolonged (pro-bleeding), there is also reduced anticoagulant protein synthesis (Protein C, S, antithrombin), so patients can also develop thrombosis. True bleeding risk correlates poorly with INR in ALF.
- DO NOT correct INR with FFP unless there is active bleeding or a planned procedure - INR is your prognostic marker.
Renal Failure Mechanism
- "Functional" renal failure (hepatorenal syndrome type): splanchnic vasodilation → reduced effective arterial volume → renal vasoconstriction via renin-angiotensin-aldosterone, sympathetic nervous system, endothelin
- Kidneys are histologically normal - failure is hemodynamically driven and reversible with liver recovery or transplantation
- Type 1 HRS: rapidly progressive (creatinine doubles to > 2.5 mg/dL in < 2 weeks)
- Type 2 HRS: slower progression
SECTION 3: ETIOLOGY IN CHILDREN (DETAILED)
The single most important difference from adult ALF: etiology is indeterminate in approximately 50% of PALF cases. A smaller fraction of adult ALF is indeterminate (~12-17%).
A. Acetaminophen (Paracetamol) Toxicity
Mechanism:
- Normal doses: 90-95% metabolized by glucuronidation and sulfation to non-toxic conjugates; ~5% by CYP2E1 → highly reactive toxic metabolite NAPQI (N-acetyl-p-benzoquinoneimine)
- NAPQI is immediately neutralized by hepatic glutathione
- In overdose: glutathione stores depleted → NAPQI accumulates → covalent binding to hepatocyte proteins → zone 3 (perivenular) necrosis (CYP2E1 concentrated here)
Risk factors for hepatotoxicity at lower doses:
- Chronic alcohol use (induces CYP2E1, depletes glutathione)
- Malnutrition / fasting (glutathione depletion)
- Concomitant CYP450 inducers: phenytoin, carbamazepine, rifampicin
- Multiple simultaneous acetaminophen-containing products ("staggered overdose")
Clinical patterns:
- Intentional (suicidal) overdose: Single large dose, usually presents within 4 hours, receives NAC promptly → better outcome
- Unintentional ("therapeutic misadventure"): Multiple small doses over days, late presentation, NAC less effective → worse outcome (6 deaths vs 1 in suicidal group in one series)
Hallmark lab pattern: Very high AST (often > 3,000-10,000 IU/L), disproportionately elevated compared to bilirubin. This "hyperacute" enzyme pattern (rapid rise and fall) is characteristic.
Acetaminophen-protein adducts: A research tool that detects covalent binding of NAPQI to cysteine residues on proteins. Detectable for 6-8 days. Found in 20% of "indeterminate" PALF cases - revealing unrecognized APAP poisoning. Not yet clinically approved but expected in emergency departments soon.
Treatment: NAC - see Section 5.
B. Autoimmune Hepatitis (AIH)
- Characterized by: elevated aminotransferases, autoantibodies (ANA, ASMA, anti-LKM1, SLA/LP), polyclonal hypergammaglobulinemia (elevated IgG), lymphoplasmocytic interface hepatitis
- Female preponderance (~3-4:1)
- Can present as acute or even fulminant hepatitis in both children and adults - must always be considered in PALF
- AIH-1: anti-ANA + ASMA; associated with HLA DR3, DR4
- AIH-2: anti-LKM1 + anti-LC1; associated with HLA DR3, DR7; more common in children
- Transplant-free survival lower than acetaminophen group
- Treatment: IV methylprednisolone - but requires caution in PALF setting (risk of infection, may precipitate sepsis in already immunocompromised patient)
C. Wilson Disease
- Autosomal recessive mutation in ATP7B gene (copper-transporting P-type ATPase) on chromosome 13q14
- Results in impaired biliary copper excretion → copper accumulates in liver, brain, cornea, kidneys
- Classic triad: Liver disease + Kayser-Fleischer (KF) rings + neuropsychiatric symptoms
- Liver disease spectrum: asymptomatic hepatomegaly → chronic hepatitis → cirrhosis → fulminant liver failure
- In PALF, Wilson disease presents with a distinctive pattern:
- Coombs-negative hemolytic anemia (copper released from necrotic hepatocytes damages RBCs)
- Very high serum bilirubin (> 18 mg/dL) with disproportionately low alkaline phosphatase (ALP)
- ALP:bilirubin ratio < 4 is suggestive (alkaline phosphatase paradoxically low because copper inhibits its release)
- Renal tubular acidosis (Fanconi syndrome)
- Neuropsychiatric: mood changes, dysarthria, tremor, ataxia
- Diagnosis:
- Serum ceruloplasmin: low (< 20 mg/dL) - but may be falsely normal or even elevated in acute inflammation
- 24-hour urine copper: elevated (> 100 µg/24h; typically > 500 µg in ALF setting)
- Slit-lamp examination: KF rings (absent in ~50% of hepatic-predominant presentation)
- Liver biopsy copper content > 250 µg/g dry weight
- Serum copper: usually very high in ALF from Wilson disease
- Treatment: Copper chelation with D-penicillamine or trientine. In acute fulminant Wilson disease, liver transplantation is almost always required - medical therapy alone rarely sufficient
- First-line medical bridge: penicillamine chelation + albumin dialysis (MARS) to buy time for transplant
D. Hepatitis Viruses
Hepatitis A (HAV):
- Feco-oral transmission, self-limited
- ALF rate: 0.1-0.4% overall; higher in underlying liver disease
- Favorable etiology - high spontaneous recovery rate (> 50% transplant-free survival)
- No specific antiviral; supportive care
Hepatitis B (HBV):
- ALF from acute HBV: 1-4% of acute HBV infections
- Or: Acute flare of chronic HBV (spontaneous reactivation or immunosuppression-related)
- Treatment: nucleos(t)ide analogues (entecavir or tenofovir) - reduce viral replication, may allow spontaneous recovery
- HBV reactivation (in immunocompromised child, cancer treatment): prophylactic lamivudine/entecavir before immunosuppression
Hepatitis E (HEV):
- Feco-oral transmission (water-borne in endemic areas: South Asia, Africa, Middle East)
- Dominant etiology of ALF in developing world
- Genotype 1 and 2: epidemics in pregnancy (mortality 20% in pregnant women)
- Genotype 3 and 4: zoonotic, sporadic cases in developed countries
Herpes Simplex Virus (HSV):
- Rare cause overall but extremely important in neonates and immunocompromised
- HSV hepatitis in neonates: may present WITHOUT skin vesicles
- Clinical clue: fever, hepatomegaly, coagulopathy, seizures, conjunctivitis in a neonate
- Diagnosis: HSV PCR (blood, CSF, vesicle swab, liver biopsy) + HSV DFA
- Near-100% mortality if untreated → empiric IV acyclovir 20 mg/kg q8h in ALL neonates with ALF until HSV excluded
- Histology: eosinophilic intranuclear inclusions (Cowdry type A)
Epstein-Barr, CMV, Adenovirus, Enterovirus, Parvovirus B19:
- Less common; typically in immunocompromised patients
- Adenovirus: serious in post-transplant children
E. Drug-Induced Liver Injury (DILI) - Idiosyncratic
- Distinct from acetaminophen (dose-related, predictable) - idiosyncratic DILI is unpredictable, rare, not dose-dependent
- Implicated drugs in children: valproic acid (especially in mitochondrial disease/POLG mutation), isoniazid, halothane, NSAIDs, antidepressants, statins, antibiotics (amoxicillin-clavulanate, nitrofurantoin)
- Pattern: Subacute - slower evolution, weeks to months of jaundice before encephalopathy
- Histology varies by agent: hepatocellular, cholestatic, or mixed
- Transplant-free survival: lower than acetaminophen (~25%)
- Diagnosis: drug history (including herbal/CAM products), drug withdrawal + improvement in aminotransferases
- Treatment: withdraw offending agent; NAC may be considered
F. Metabolic/Genetic Diseases (Pediatric-Specific - Critical Category)
These are unique to PALF and rarely cause ALF in adults:
Galactosemia:
- AR; deficiency of galactose-1-phosphate uridyl transferase (GALT)
- Galactose-1-phosphate accumulates → hepatocyte injury
- Presents in neonates after initiation of milk feeding
- Clinical: jaundice, coagulopathy, E. coli sepsis, cataracts, hypoglycemia
- Diagnosis: GALT enzyme assay on RBCs; urine reducing substances (Clinitest positive, glucose negative)
- Treatment: Galactose-free formula immediately - this is an emergency
Tyrosinemia Type 1 (Hepatorenal Tyrosinemia):
- AR; deficiency of fumarylacetoacetate hydrolase (FAH)
- Accumulation of fumarylacetoacetate + succinylacetone → hepatocyte and renal tubular damage
- Presents in infancy with ALF, rickets (renal Fanconi syndrome), hepatocellular carcinoma risk
- Diagnosis: elevated succinylacetone in urine/blood; plasma amino acids (elevated tyrosine, phenylalanine, methionine)
- Treatment: Nitisinone (NTBC) - blocks upstream enzyme (4-HPPD), dramatically reduces toxic metabolite production; must start urgently
Urea Cycle Disorders (OTC deficiency, CPS1 deficiency):
- X-linked (OTC) or AR (CPS1)
- Defect in ammonia detoxification → hyperammonemia without liver failure per se (AST/ALT may be relatively normal, NH₃ very elevated)
- OTC (ornithine transcarbamylase) deficiency: most common urea cycle disorder; X-linked
- Treatment: protein restriction, sodium benzoate + sodium phenylacetate (alternative ammonia scavengers), dialysis, liver transplantation (curative)
Organic Acidemias (MSUD, MMA, Propionic Acidemia):
- Amino acid oxidation defects → accumulation of toxic organic acids
- Maple syrup urine disease (MSUD): branched-chain amino acid catabolism defect
- Presents with metabolic acidosis, elevated anion gap, encephalopathy
- Diagnosis: plasma amino acids, urine organic acids, acylcarnitine profile
Fatty Acid Oxidation Defects (LCHAD, VLCAD):
- Long-chain 3-hydroxyacyl-CoA dehydrogenase (LCHAD) or very-long-chain acyl-CoA dehydrogenase deficiency
- Presents with hypoglycemia, hepatopathy, lactic acidosis
- Important: LCHAD deficiency in the fetus causes AFLP (acute fatty liver of pregnancy) in the heterozygous mother
- Acylcarnitine profile diagnostic
Mitochondrial Liver Disease (POLG mutations, Alpers syndrome):
- POLG: mitochondrial DNA polymerase gamma - essential for mtDNA replication
- Alpers-Huttenlocher syndrome: POLG mutation + liver failure triggered by valproate use
- Other features: refractory seizures, psychomotor regression, cerebellar ataxia
- Diagnosis: muscle/liver biopsy (mitochondrial proliferation, COX deficiency), POLG sequencing, lactate:pyruvate ratio
- Critical: LT is generally contraindicated in mitochondrial disease because extrahepatic disease (brain, muscle) continues to progress
- Avoid valproate in any child with suspected mitochondrial disease
Neonatal Hemochromatosis / Gestational Alloimmune Liver Disease (GALD):
- Mechanism: maternal IgG antibodies (against unknown fetal hepatocyte antigen) cross the placenta → complement-mediated fetal hepatocyte injury → iron deposition in liver and extrahepatic sites
- Extrahepatic siderosis distinguishes it from other neonatal liver disease
- Presents at birth or in first days/weeks: coagulopathy, hypoglycemia, hypoalbuminemia, jaundice
- Diagnosis:
- MRI: T2 hypointensity of pancreas, heart, adrenals, thyroid (extrahepatic iron)
- Buccal mucosal biopsy: stainable iron (sensitive + non-invasive)
- Elevated ferritin (often extremely high)
- Treatment: IVIG + double-volume exchange transfusion + antioxidant cocktail (NAC, vitamin E, selenium, desferrioxamine)
- Next pregnancy prevention: IVIG infusions to mother in subsequent pregnancies significantly reduce recurrence
G. Budd-Chiari Syndrome (Hepatic Vein Thrombosis)
- Obstruction of hepatic venous outflow at any level: hepatic veins, inferior vena cava, right atrium
- Causes centrilobular congestion and necrosis
- In children: associated with prothrombotic states (myeloproliferative disease, protein C/S/antithrombin deficiency, activated protein C resistance, antiphospholipid syndrome)
- Acute presentation: sudden hepatomegaly, abdominal pain, ascites, jaundice
- Diagnosis: Doppler ultrasound (absent/reversed flow in hepatic veins); CT/MRI with contrast
- Treatment: anticoagulation, TIPS (transjugular intrahepatic portosystemic shunt), LT
H. Reye Syndrome
- Classic description: Acute non-inflammatory encephalopathy + hepatic dysfunction following viral illness (varicella, influenza) in children treated with salicylates (aspirin)
- Mechanism: aspirin + viral illness → mitochondrial dysfunction → microvesicular steatosis in liver
- Histology: panlobular microvesicular steatosis WITHOUT hepatocellular necrosis
- Laboratory: elevated AST/ALT, elevated ammonia, normal bilirubin (cholestasis absent)
- Now very rare since aspirin contraindicated in children < 16 years with febrile illness
- Treatment: supportive (glucose supplementation, ammonia reduction, ICP management)
SECTION 4: CLINICAL FEATURES (DETAILED)
Initial Presentation
Symptoms often non-specific initially:
- Nausea, vomiting, anorexia, malaise
- Right upper quadrant or epigastric pain
- Fatigue and lethargy
As liver failure progresses:
- Jaundice (yellow discoloration of skin + sclera) - may be absent early
- Dark urine (bilirubinuria) + pale stools (cholestasis)
- Coagulopathy manifestations: easy bruising, petechiae, prolonged bleeding from venipuncture sites, epistaxis, mucosal bleeding
- Hepatomegaly initially (liver swollen/edematous); then liver may shrink (parenchymal loss) - "rapid liver shrinkage" is an ominous sign of massive necrosis
Hepatic Encephalopathy - Detailed Staging in Children
Important: HE in children - especially young children - is often missed because early signs differ from adults:
| Stage | Adult Features | Pediatric Modifications (Stages 1 & 2) |
|---|---|---|
| 1 | Mild confusion, subtle personality change, sleep inversion | Irritability, excessive crying, decreased interaction, poor feeding, sleep disturbances, short attention span |
| 2 | Drowsiness, asterixis, disorientation | Excessive sleepiness, moderate confusion, personality changes, inappropriate behavior, intermittent disorientation, inability to perform age-appropriate tasks |
| 3 | Stupor, hyperreflexia, responds to verbal stimuli only | Stupor, delirium, hyperreflexia, extensor plantar response, responds to verbal stimuli |
| 4a | Coma, responds to pain | Coma with decerebrate/decorticate response to pain |
| 4b | Coma, no pain response | Deep coma, no pain response, risk of herniation imminent |
Asterixis (liver flap): Non-rhythmic, rapid extension-flexion of the wrist when arms are held outstretched with dorsiflexed wrists. Cannot be elicited in deep coma - requires consciousness.
Seizures: Occur in 10-30% of PALF patients with HE. Can be focal or generalized.
EEG changes (progressive):
- Slowing of alpha rhythm (8-13 Hz background)
- Progressive delta slowing (0-4 Hz)
- Triphasic waves - characteristic of metabolic encephalopathy; portends poor prognosis
- Burst-suppression pattern in severe/late disease
MRI findings:
- T2 hyperintensity in basal ganglia (globus pallidus): chronic copper deposition (Wilson disease)
- T1 hyperintensity in globus pallidus: manganese accumulation in chronic liver disease
- Diffuse cerebral edema, sulcal effacement in acute herniation
Systemic Manifestations
Cardiovascular:
- Hyperdynamic circulation: high CO, low SVR, warm extremities, bounding pulse
- Blood pressure may be low (vasodilated state)
- Relative adrenal insufficiency common in critical illness
Renal:
- Hepatorenal syndrome Type 1: acute, rapid decline in GFR
- Clinical: rising creatinine, oliguria, hyponatremia, concentrated urine (FENa < 1%)
- Distinguish from ATN (FENa > 1%, muddy brown casts)
- Prerenal dehydration (responds to fluid challenge) - always rule out first
Pulmonary:
- Hepatopulmonary syndrome: V/Q mismatch, intrapulmonary shunting → hypoxemia
- Portopulmonary hypertension: elevated pulmonary artery pressure → right heart strain
- Aspiration risk (reduced gag reflex in HE)
- ARDS in severe multi-organ failure
Metabolic:
- Hypoglycemia (loss of gluconeogenesis + glycogen storage + impaired insulin degradation): dangerous and common - monitor glucose q1-2h
- Hyponatremia: may be dilutional; careful correction (overly rapid correction worsens cerebral edema)
- Hypokalemia, hypomagnesemia, hypophosphatemia: common, require monitoring and repletion
- Metabolic alkalosis (early) → metabolic acidosis (late, poor prognostic sign)
- Lactic acidosis: indicates tissue hypoperfusion / mitochondrial dysfunction
Infection:
- Occurs in > 50% of ALF patients
- Gram-positive organisms predominate (skin flora from invasive catheters + impaired Kupffer cell function)
- Procalcitonin is unreliable in ALF (markedly elevated in severe hepatic necrosis even without infection)
- Fungal infections (Candida) especially with prolonged ICU stay + broad-spectrum antibiotics
SECTION 5: DIAGNOSIS (DETAILED)
Clinical Algorithm
Laboratory Investigations
Severity and Synthetic Function:
| Test | Significance |
|---|---|
| PT / INR | Defines PALF (INR ≥ 1.5 with HE, ≥ 2.0 without). Primary prognosis marker |
| Factor V | Shortest half-life of all clotting factors (~12h) - most sensitive for trend monitoring. Rising factor V = recovery. Falling = deterioration |
| Factor VII | Even shorter half-life (4-6h) - earliest indicator but less prognostically validated |
| Serum albumin | Reflects chronic synthetic function; may be acutely low |
| AST / ALT | Massively elevated (thousands). May paradoxically fall as all hepatocytes destroyed - "enzyme burnout" |
| Bilirubin | Total + direct; rises progressively |
| Alkaline phosphatase (ALP) | Paradoxically LOW in Wilson disease - copper inhibits ALP release |
| GGT | Elevated in cholestatic DILI; may guide etiology |
| Arterial ammonia | Correlates with HE severity in ALF (unlike chronic liver disease). Target < 75 µmol/L; levels > 150-200 associated with herniation risk |
| Serum lactate | Elevated = poor prognosis (tissue hypoperfusion; also seen in mitochondrial disease) |
| Blood gas (arterial) | Acid-base status; pH < 7.3 after resuscitation = Kings College Criteria criterion |
| Blood glucose | Monitor q1-2h; hypoglycemia very common and dangerous |
| Creatinine + BUN | Renal involvement; also Kings College Criteria component |
| CBC + differential | Thrombocytopenia; hemolysis (Wilson disease = Coombs-negative) |
| Fibrinogen | < 100 mg/dL indicates severe coagulopathy; needed before ICP monitor |
| APAP level | Always check even if not suspected; adducts for indeterminate cases |
Etiology-Directed Work-up (ALL to be sent simultaneously, not sequentially):
Viral panel:
- HAV IgM
- HBsAg, anti-HBc IgM, HBV DNA
- Anti-HCV (rarely causes ALF acutely)
- HEV IgM / HEV RNA (if travel history or endemic area)
- HSV-1/2 PCR (blood + CSF + skin swab) - mandatory in ALL neonates
- CMV PCR, EBV PCR, adenovirus PCR, enterovirus PCR
- Parvovirus B19 IgM
Metabolic:
- Plasma amino acids (tyrosinemia: tyrosine; MSUD: leucine/isoleucine/valine; urea cycle: citrulline, argininosuccinic acid)
- Urine organic acids (succinylacetone in tyrosinemia; organic acids in OA)
- Acylcarnitine profile (fatty acid oxidation defects)
- Serum lactate + pyruvate ratio (mitochondrial disease: > 25)
- Galactose-1-phosphate uridyl transferase (galactosemia) in neonates
- Urine reducing substances (Clinitest)
- Alpha-1-antitrypsin level + phenotype (PiZZ genotype)
Wilson Disease:
- Serum ceruloplasmin (note: falsely low in normal liver due to acute phase response - may be "normal" in Wilson ALF)
- 24-hour urine copper
- Slit-lamp for KF rings
- Serum copper (very high in Wilson ALF)
- Liver biopsy copper content (if INR allows)
- ALP:bilirubin ratio (< 4 suggests Wilson)
Autoimmune:
- ANA titre
- Anti-smooth muscle antibody (ASMA)
- Anti-liver-kidney microsome type 1 (anti-LKM1)
- Anti-soluble liver antigen (anti-SLA/LP)
- Serum IgG level (polyclonal hypergammaglobulinemia)
Neonatal hemochromatosis / GALD:
- Serum ferritin (very high)
- Transferrin saturation
- MRI liver + pancreas + heart: T2 hypointensity
- Buccal mucosal biopsy: stainable iron
Imaging:
- Liver Doppler ultrasound: liver size, echotexture, portal and hepatic vein flow (Budd-Chiari), ascites, splenomegaly
- CT/MRI brain: cerebral edema (sulcal effacement, loss of grey-white differentiation), intracranial hemorrhage
- CT of abdomen if hepatic vein thrombosis suspected
- Chest X-ray: pulmonary infiltrates (aspiration, ARDS)
Liver biopsy: Reserved for specific situations:
- Suspicion of autoimmune hepatitis (requires histological confirmation for steroid decision)
- Malignant infiltration
- Requires INR < 1.5, platelets > 50,000, fibrinogen > 100 mg/dL
- Route: transjugular preferred when coagulopathic
SECTION 6: MANAGEMENT (DETAILED)
Triage and Initial Response
Immediate steps upon diagnosis:
- Contact pediatric liver transplant center NOW - transfer is mandatory
- Admit to PICU
- NPO + IV access (two large-bore peripheral IVs minimum)
- Continuous cardiorespiratory monitoring + pulse oximetry
- Foley catheter for strict urine output monitoring
- Serum glucose check + IV 10% dextrose if hypoglycemic (avoid 50% dextrose boluses - osmotic load worsens cerebral edema)
- Neurological assessment q1-2h for encephalopathy grade
Airway management:
- Grade 1-2 HE: awake, monitor closely, NO sedatives
- Grade 3-4 HE: elective intubation for airway protection before respiratory failure; use short-acting agents (avoid benzodiazepines - cannot be metabolized; propofol in short-acting doses is preferable); RSI with fentanyl + rocuronium
- Intubation itself raises ICP - pre-treat with lignocaine 1.5 mg/kg IV + ensure adequate sedation during laryngoscopy
Management of Hepatic Encephalopathy and Cerebral Edema
Ammonia Reduction
Critical difference from chronic liver disease: Lactulose has NOT been shown to improve survival in ALF. Its mechanism (lowering gut ammonia production by acidification) works in cirrhosis but may be problematic in ALF because:
- Can cause colonic distension (complicates LT surgery)
- May worsen fluid/electrolyte balance However, it is still commonly used as it does lower ammonia levels.
- Lactulose: 1-2 mL/kg (neonates), 10-30 mL q6h (older children) - titrate to 2-3 soft stools per day. Avoid colonic distension.
- Rifaximin: 10-20 mg/kg/day (max 1200 mg/day) - preferred over neomycin (less nephrotoxic/ototoxic). Reduces intestinal bacterial ammonia generation.
- L-ornithine-L-aspartate (LOLA): Provides substrates for urea cycle and glutamine synthesis in residual hepatocytes. IV or oral.
- Protein restriction: Short-term to reduce amino acid-derived ammonia load. Limit to 0.5-1 g/kg/day transiently. Prolonged restriction is harmful (causes catabolism, worsens outcome).
- CRRT (Continuous Renal Replacement Therapy): Most effective method for rapid ammonia clearance even in the absence of renal failure. Superior to intermittent hemodialysis in hemodynamically unstable patients.
- Polyethylene glycol (PEG): Recent data support use as single-dose bowel prep for rapid ammonia reduction; may be preferable to lactulose for this purpose.
Cerebral Edema - Step-by-Step Protocol
Environmental and positional:
- Head of bed at 30 degrees, head in midline neutral position (no neck flexion/rotation)
- Quiet environment, minimize stimulation, dim lights
- Avoid fever (hyperthermia increases cerebral metabolic demand and worsens edema) - target normothermia
- Avoid hypoxemia (O2 saturation > 95%) and hypercapnia
Osmotherapy:
- Target serum sodium 145-150 mEq/L (hypernatremia is cerebroprotective - increases serum osmolality, reduces brain water)
- Use 3% hypertonic saline (NaCl): 200 mL of 2.7% solution or 20 mL of 30% - can give continuously to maintain target Na
- Mannitol 20%: 0.5-1 g/kg IV over 15-20 minutes for acute ICP spikes. Do NOT give if serum osmolality > 320 mOsm/L or if renal failure (mannitol will accumulate and worsen osmolality)
- Both agents work by osmotic withdrawal of water from brain cells
Hyperventilation:
- Target PaCO₂ 30-35 mmHg (mild) or 25-30 mmHg (acute crisis)
- Works by cerebral vasoconstriction → reduces cerebral blood volume → lowers ICP
- Short-term bridge only - vasoconstriction cannot be sustained (cerebral ischemia risk)
ICP Monitoring:
- Considered for Grade 3-4 HE at experienced transplant centers
- Goals: ICP < 20-25 mmHg; cerebral perfusion pressure (CPP) > 50 mmHg (CPP = MAP - ICP)
- Risks: Bleeding (coagulopathic patients); infection; procedure-related ICP spike
- Prerequisites before insertion: INR < 1.4, platelets > 50,000/mm³, fibrinogen > 100 mg/dL
- Types: epidural (lower risk) > subdural > intraparenchymal (most accurate but highest risk)
- ICP monitoring has largely fallen out of favor as no randomized trial shows mortality benefit, and risks are significant
- Non-invasive alternatives: Transcranial Doppler ultrasound (pulsatility index reflects ICP), optic nerve sheath diameter by USS (> 5 mm suggests elevated ICP), jugular venous oximetry
Hypothermia:
- Induced mild hypothermia (target 33-35°C): Used as last resort for refractory intracranial hypertension - no RCT data in PALF, but physiologically decreases cerebral metabolic demand + ammonia production
- Risk: coagulopathy, cardiac arrhythmia, infection
- Note: CVVH/CRRT itself causes mild hypothermia, which may be partially protective
Barbiturate coma:
- Pentobarbital coma for refractory ICP elevation - last resort, no controlled trial data
- Significant side effects: hemodynamic instability, prolonged sedation
Hemodynamic Management
Fluids:
- Goal: Maintain adequate perfusion without fluid overload (worsens cerebral and pulmonary edema)
- Balanced crystalloids (Ringer's lactate or Plasmalyte) preferred over normal saline (avoids hyperchloremic acidosis)
- Avoid excessive free water (worsens hyponatremia + cerebral edema)
- Continuous 10% dextrose infusion to maintain euglycemia (80-120 mg/dL)
Vasopressors:
- Norepinephrine (noradrenaline): first-line vasopressor for ALF-associated vasodilatory shock
- Vasopressin: second agent if norepinephrine inadequate
- Relative adrenal insufficiency is common in critical illness - low-dose hydrocortisone 1-2 mg/kg/day may be considered if refractory vasopressor dependence (stress-dose steroids)
Coagulopathy management:
- Do NOT prophylactically correct INR - it is your prognostic marker
- Vitamin K 1-2 mg IV (or 10 mg in older children/adolescents): Give once - to rule out vitamin K deficiency as a correctable component
- Fresh Frozen Plasma (FFP): Use ONLY for active hemorrhage or before invasive procedures. Each dose lasts 4-6 hours. May worsen fluid overload and mask prognosis.
- Prothrombin complex concentrate (PCC): If fibrinogen < 100 mg/dL; faster and lower volume than FFP; short-acting (hours)
- Cryoprecipitate: For fibrinogen replacement (target > 100 mg/dL)
- Platelets: Transfuse if < 50,000/mm³ and bleeding, or before ICP monitor placement
- Recombinant Factor VIIa (rFVIIa): Can temporarily correct INR for procedures; expensive, short-acting
Renal Management
- CRRT (continuous venovenous hemofiltration/hemodialysis): Preferred over intermittent hemodialysis in hemodynamically unstable patients
- Manages fluid balance, electrolytes, acid-base
- Removes ammonia (best pharmacological ammonia-lowering therapy available)
- Delivers stable hemodynamics
- Target: Urine output > 1 mL/kg/hour; serum creatinine trending down or stable
- Avoid nephrotoxins: aminoglycosides, vancomycin trough monitoring, NSAIDs, contrast agents
- Hepatorenal syndrome: responds to liver recovery/transplantation - vasoconstrictors (terlipressin, norepinephrine + albumin) may be used as bridge
Infection Management
- Surveillance cultures every 48-72 hours: Blood (all lines), urine, tracheal aspirate
- Broad-spectrum empiric antibiotics when signs of infection appear:
- Gram-positive coverage: Vancomycin (adjust for renal function)
- Gram-negative coverage: Piperacillin-tazobactam or meropenem
- HSV coverage: IV acyclovir empirically in all neonates with ALF until HSV excluded
- Antifungal prophylaxis: Fluconazole in prolonged ICU stay (> 3 days), especially post-transplant
- Prophylactic antibiotics: No clear survival benefit shown in controlled trials, but empiric use is common in presence of SIRS without evident infectious source
- Note: Procalcitonin is NOT reliable in ALF (elevated from hepatic necrosis itself)
Nutritional Support
- Early enteral nutrition via nasogastric tube is preferred
- Do NOT withhold nutrition waiting for LT evaluation
- High carbohydrate content to prevent hypoglycemia
- Short-term protein restriction: 0.5-1 g/kg/day to reduce ammonia load; INCREASE back to normal as condition stabilizes
- Avoid branched-chain amino acid supplementation - no proven benefit in PALF
- Total parenteral nutrition if enteral route not feasible (obstruction, ileus)
Acid-Base and Electrolytes
- Glucose: continuous 10% dextrose drip, check q1-2h
- Hyponatremia: Manage carefully - rapid correction causes osmotic demyelination; use hypertonic saline slowly (target Na 145-150 for cerebral protection)
- Hypokalemia, hypomagnesemia, hypophosphatemia: Common, require supplementation monitoring
- Metabolic acidosis: Bicarbonate therapy for pH < 7.1 as temporizing measure; CRRT is more effective for refractory acidosis
- Hyperlactataemia: pH < 7.3 + lactate > 3.5 after resuscitation = very poor prognosis (King's College Criterion in APAP)
Gastrointestinal Protection
- Proton pump inhibitor (pantoprazole IV): prophylaxis against stress ulceration
- H2 blockers can be used if PPI unavailable
- Monitor for gastrointestinal bleeding (coagulopathy)
SECTION 7: ETIOLOGY-SPECIFIC THERAPIES (DETAILED)
N-Acetylcysteine (NAC)
Primary indication: Acetaminophen toxicity (highest evidence)
Mechanism of action:
- Glutathione precursor: Provides cysteine (rate-limiting substrate) for glutathione synthesis → replenishes depleted GSH stores → neutralizes NAPQI
- Direct antioxidant: Sulfhydryl groups directly scavenge free radicals
- Anti-inflammatory: Improves microcirculatory flow, reduces cytokine storm
- Anti-apoptotic: Improves mitochondrial function
Dosing:
- IV protocol (preferred when ALF is established):
- Loading dose: 150 mg/kg in 5% dextrose over 60 minutes
- Maintenance: 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours (standard adult protocol)
- Alternative (older protocol): 140 mg/kg loading, then 70 mg/kg q4h for 17 doses
- Oral: 140 mg/kg loading, then 70 mg/kg q4h - for 72 hours in mild toxicity
- Most effective within 8-10 hours of ingestion, but still beneficial up to 24-36 hours; continue until liver recovery
NAC beyond acetaminophen:
- An RCT (Lee et al., Gastroenterology 2009) showed IV NAC improved transplant-free survival in non-acetaminophen ALF - specifically in grade 1-2 HE
- No benefit in grade 3-4 HE with non-acetaminophen etiology
- Now commonly used in: idiosyncratic DILI, autoimmune hepatitis, hepatitis B, indeterminate ALF (especially grades 1-2 HE)
- Low risk/high benefit: Given NAC's safety profile, most centers use it broadly in PALF
Acyclovir
- Indication: HSV hepatitis/ALF - especially neonates and immunocompromised
- Dose: 20 mg/kg/dose IV q8h (neonatal); 10-15 mg/kg/dose IV q8h in older children
- Duration: 14-21 days; then consider oral suppressive therapy
- Empiric use: All neonates with unexplained ALF should receive IV acyclovir empirically until HSV is excluded by PCR
- Monitor renal function (nephrotoxic - ensure adequate hydration)
Corticosteroids for Autoimmune Hepatitis
- IV methylprednisolone 1-2 mg/kg/day
- Controversy in fulminant AIH: Risk of worsening infection vs. benefit of inflammation control
- Best evidence for steroids in autoimmune hepatitis when coagulopathy is present WITHOUT HE grade 3-4
- If HE grade 3-4: risk likely outweighs benefit; LT listing should not be delayed for steroid trial
- Prednisolone 1 mg/kg/day orally for milder presentations; switch to azathioprine for maintenance
Nucleos(t)ide Analogues for Hepatitis B
- Entecavir (first-line) or tenofovir disoproxil fumarate (TDF)
- Start immediately in acute HBV ALF
- Aim: reduce viral replication → allow spontaneous regeneration
- Monitoring: HBV DNA level at 1-2 weeks to confirm response
Wilson Disease - Specific Management
Acute presentation requiring emergency treatment:
- Stop all copper intake (dietary restriction temporarily; avoid copper-containing supplements)
- D-penicillamine: 20 mg/kg/day orally - chelates copper for urinary excretion. Long-term definitive therapy. Poor efficacy in acute fulminant Wilson disease (too slow).
- Trientine: Alternative copper chelator with fewer side effects; better tolerated
- Zinc acetate: Inhibits intestinal copper absorption; maintenance therapy
- Albumin dialysis (MARS - Molecular Adsorbent Recirculating System): Removes protein-bound copper + other toxins. Used as bridge to transplantation.
- Continuous venovenous hemofiltration (CVVH): Also clears free copper; reduces hemolysis
- Liver transplantation: Usually required for fulminant Wilson disease. LT is curative (replaces the metabolic defect).
Neonatal Hemochromatosis (GALD) Treatment
- Double-volume exchange transfusion: Removes maternal IgG antibodies (passive immunity responsible for injury)
- IVIG: 1 g/kg IV - blocks Fc receptors, prevents complement activation
- Antioxidant cocktail:
- N-acetylcysteine: 100 mg/kg/day IV
- Vitamin E (alpha-tocopherol): 25 IU/kg/day
- Selenium: 3 µg/kg/day
- Desferrioxamine: iron chelation 30 mg/kg/day IV (removes excess iron)
- Prostaglandin E1 (some protocols)
- LT if no response within 48-72 hours
Galactosemia / Tyrosinemia - Specific Treatment
Galactosemia:
- IMMEDIATELY switch to galactose-free formula (soy-based or casein hydrolysate)
- Treat concurrent E. coli sepsis aggressively
- Supportive care: correct coagulopathy, hypoglycemia
- Long-term: strict galactose-free diet; monitoring for ovarian failure, cognitive delays despite compliance
Tyrosinemia Type 1:
- Nitisinone (NTBC) 1-2 mg/kg/day PO - blocks 4-hydroxyphenylpyruvate dioxygenase (4-HPPD) enzyme, preventing accumulation of toxic metabolites (fumarylacetoacetate, succinylacetone)
- Must simultaneously restrict dietary tyrosine and phenylalanine (low-Phe/Tyr formula)
- Prevents hepatocellular carcinoma (regular surveillance with AFP + imaging still required)
- LT if NTBC fails, established cirrhosis, or HCC develops
Mushroom Toxicity (Amanita phalloides)
- Amatoxins: α-amanitin inhibits RNA polymerase II → stops mRNA synthesis → hepatocyte death
- Characteristic: delayed presentation (6-24 hours after ingestion), initial GI symptoms, then apparent recovery, then fulminant hepatic failure at 3-5 days
- Treatment:
- Silibinin (Silymarin): IV formulation (not available in all countries); competes with amatoxin for hepatocyte uptake; start within 48 hours
- N-acetylcysteine
- Penicillin G IV (large doses): displaces amatoxin from albumin
- Consider MARS/extracorporeal support
- Liver transplantation if hepatic failure established
SECTION 8: EXTRACORPOREAL LIVER SUPPORT
These devices aim to "bridge" patients to transplantation or spontaneous recovery by temporarily performing liver functions:
MARS (Molecular Adsorbent Recirculating System)
- Blood is dialyzed across an albumin-impermeable membrane
- Albumin-bound toxins (bilirubin, bile acids, copper) + water-soluble toxins removed through secondary circuit
- Randomized trials: No overall mortality benefit in ALF, but improvements in HE symptoms and hemodynamics noted
- Best evidence for: Wilson disease (copper removal), hyperbilirubinemia reduction, bridge to LT
Prometheus System
- Fractionated plasma separation + adsorption + dialysis
- Separates patient's albumin from blood → passes through two absorbent columns + high-flux dialyzer
- Safety established; no survival benefit demonstrated in acute on chronic liver failure
High-Volume Plasma Exchange (HVP)
- Removes toxins AND replaces beneficial plasma proteins (coagulation factors, albumin)
- Small studies suggest survival benefit in non-acetaminophen ALF; larger RCTs pending
- Practically: removes 8-12 L of plasma, replaced with FFP
Bioartificial Liver Systems
- Incorporate live hepatocytes (porcine or human cell lines) to replicate metabolic functions
- Still largely experimental; safety concerns with xenogeneic cells
SECTION 9: LIVER TRANSPLANTATION (DETAILED)
Timing
Transplant evaluation begins on admission - in parallel with medical management, not after:
- PALF patients are UNOS Status 1A (highest priority): expected death within 7 days without LT
- Time to deterioration from grade 2 to grade 4 HE can be hours
Listing Criteria and Decision-Making
The difficulty: some patients recover spontaneously (no LT needed), others die without LT. Identifying which is which remains a major clinical challenge.
King's College Criteria (KCC) - for Adults, used in PALF:
For acetaminophen-induced ALF:
- Arterial pH < 7.30 after resuscitation
OR all three of:
- INR > 6.5 (PT > 100s)
- Serum creatinine > 3.4 mg/dL (301 µmol/L)
- Grade III or IV encephalopathy
Additionally: Hyperlactatemia (lactate > 3.5 mmol/L) or hyperphosphatemia (phosphate > 1.2 mmol/L) are strong predictors of poor prognosis and should be added to KCC.
For non-acetaminophen ALF:
- INR > 6.5
OR 3 out of 5 of:
- Age < 10 or > 40 years
- Etiology: non-A non-B hepatitis, idiosyncratic DILI
- Duration of jaundice before HE > 7 days
- PT > 50 seconds (~INR > 3.5)
- Serum bilirubin > 18 mg/dL (300 µmol/L)
Limitations of KCC in children:
- Validated in adults; age cut-off (< 10 years) not applicable to neonates/infants
- Some PALF-specific modifications proposed (PALF Study Group criteria)
- Etiology remains the most powerful predictor once encephalopathy grade is established
Expected Outcomes Without Transplant (Transplant-Free Survival by Etiology)
| Etiology | Transplant-Free Survival |
|---|---|
| Acetaminophen | ~65% |
| Hepatitis A | ~50-60% |
| Ischemic hepatitis | ~50% |
| Pregnancy-related | ~50% |
| Autoimmune hepatitis | ~20-30% |
| Hepatitis B | ~25-30% |
| Idiosyncratic DILI | ~20-25% |
| Wilson disease (fulminant) | ~0-10% (almost always requires LT) |
| Indeterminate | Worst prognosis in PALF; ~15-20% |
Source: Yamada's Gastroenterology, based on ALFSG registry data
Surgical Aspects
- Living donor liver transplantation (LDLT): Important option in children given organ size matching; can use left lateral segment from parent; LDLT is occasionally used emergently in PALF
- Whole liver (from deceased donor): standard
- Split liver: Right lobe to adult; left lobe to child
- Contraindications to LT:
- Brain death / irreversible anoxic brain injury
- Active uncontrolled systemic sepsis
- Extrahepatic malignancy
- Mitochondrial disease with extrahepatic involvement
- Severe multi-organ failure unlikely to be reversed by LT
- Poor social/psychosocial support (relative; especially for APAP with repeated suicide attempts)
Post-Transplant Outcomes in PALF
- 1-year patient survival: ~73% (Fischer's Mastery of Surgery)
- 1-year graft survival: ~59%
- Compared to biliary atresia: 89% patient survival / 78% graft survival
- PALF has lower post-LT survival than other indications because patients are sicker at time of LT, more likely to have multi-organ failure, cerebral edema, infection
- 5-year survival post-LT for pediatric liver disease overall: 80-90%
- Neurological complications post-LT occur in ~30-48% of pediatric recipients (seizures most common)
SECTION 10: PROGNOSIS - DETAILED SCORING AND PREDICTION
Clinical and Laboratory Predictors
Unfavorable prognostic markers:
| Parameter | Threshold / Sign |
|---|---|
| INR | > 4, or not improving at 48-72h |
| Factor V | < 25% of normal; falling trend |
| Serum bilirubin | > 18 mg/dL |
| Arterial ammonia | > 150-200 µmol/L |
| HE grade | 3 or 4 at presentation |
| Pace of HE progression | Rapid (days from jaundice to coma) |
| Blood gas pH | < 7.3 after resuscitation (APAP) |
| Serum lactate | > 3.5 mmol/L |
| Serum phosphate | > 1.2 mmol/L (hyperphosphatemia post-APAP = massive hepatocyte ATP depletion) |
| Renal failure | Creatinine > 3.4 mg/dL (APAP KCC) |
| Etiology | Indeterminate, subacute, Wilson disease, DILI |
| EEG | Triphasic waves, burst-suppression |
| Liver volume | Rapid shrinkage on serial imaging |
Favorable prognostic markers:
- Acetaminophen etiology (treated early with NAC)
- Hepatitis A
- Early HE grade (1-2)
- INR / factor V improving over 48-72h
- Specific metabolic disease on targeted Rx (NTBC for tyrosinemia; galactose-free diet)
- Rising liver enzymes (indicates remaining hepatocyte mass)
- Hyperacute presentation (short jaundice-to-HE interval)
PALF-Specific Score (PALF Study Group)
Based on multicenter US data, predictors of poor outcome specific to children include:
- White cell count > 9 × 10⁹/L (systemic inflammation)
- INR trajectory (not single value)
- Etiology category (indeterminate vs. known)
Serial Monitoring Protocol
Every 6-12 hours:
- INR + factor V
- Arterial ammonia
- Blood glucose
- Electrolytes (Na, K, Mg, Phos)
- Fluid balance
- Neurological examination (HE grade)
Every 24 hours:
- Full LFTs
- Creatinine, BUN
- Blood gas
- Cultures if febrile
SECTION 11: NEONATAL ALF - IN-DEPTH
Unique Features of Neonatal Presentation
- Hepatic encephalopathy may be absent or atypical in neonates (neurological immaturity, inability to assess)
- Irritability, poor feeding, reduced activity are early signs
- Hypoglycemia is more prominent in neonates (limited glycogen stores)
- The etiology spectrum is completely different from older children and adolescents
Neonatal HSV Hepatitis - Complete Protocol
Epidemiology: 1/3,000 to 1/20,000 live births; 85% acquire HSV perinatally (vertical transmission during delivery). HSV-2 more common than HSV-1 in neonatal disease.
Clinical presentations (three overlapping forms):
- Skin-eye-mouth (SEM) disease: 45%; best prognosis
- CNS disease: 30%; encephalitis + seizures
- Disseminated disease: 25%; multi-organ failure including fulminant hepatitis; highest mortality
Neonatal HSV ALF features:
- May present WITHOUT skin vesicles (40% of disseminated/CNS disease has no rash)
- High fever or hypothermia
- Hepatomegaly + coagulopathy + DIC
- Seizures (often refractory)
- Elevated AST/ALT (thousands)
- Diagnosis: HSV PCR (blood, CSF, surface swabs - mouth/eye/rectum, vesicle swab). Ophthalmological examination (conjunctivitis/keratitis). Liver biopsy: Cowdry type A intranuclear inclusions.
Treatment:
- IV acyclovir 20 mg/kg/dose q8h × 14-21 days (CNS/disseminated)
- After IV course: oral acyclovir suppressive therapy for 6 months (reduces CNS sequelae)
- Monitor renal function; ensure hydration during acyclovir
Gestational Alloimmune Liver Disease (GALD) - Complete
Pathogenesis:
- During pregnancy, an unknown fetal liver antigen is recognized as foreign by the maternal immune system
- Maternal IgG (class-specific, placenta-crossing) enters fetal circulation
- Antibody binds fetal hepatocyte surface antigen → complement activation (C5b-9 membrane attack complex)
- Complement-mediated hepatocyte lysis in utero → hepatic failure → reactive iron deposition (iron storage secondary to liver injury, not a primary iron overload)
- Extrahepatic iron accumulates because the normal hepatic iron regulatory system has failed
Why "gestational alloimmune"?
- Mother is healthy (not affected)
- Can recur in subsequent pregnancies (same antibody; recurrence rate ~90% without prevention)
- Prevented by antenatal IVIG in subsequent pregnancies (works by blocking maternal IgG from crossing placenta)
Diagnosis criteria:
- Massive hepatic iron overload (liver biopsy or MRI)
- Extrahepatic siderosis (pancreas, myocardium, adrenals, thyroid) on MRI T2 imaging
- Buccal mucosal biopsy showing stainable iron (90% sensitivity)
- Plasma/serum ferritin: markedly elevated (thousands)
Treatment:
- IVIG 1 g/kg IV - saturates Fc receptors on macrophages, reduces antibody-mediated destruction
- Exchange transfusion (double-volume) - removes maternal IgG already present in infant circulation
- Antioxidant cocktail to reduce oxidative liver injury
- LT if above fails (excellent outcomes, as the graft is free of the alloimmune injury)
Mitochondrial Liver Disease - Complete
Why it matters: Valproic acid is a commonly used anticonvulsant. Its use in a child with unrecognized mitochondrial disease (especially POLG mutation) can precipitate fulminant hepatic failure.
POLG mutations - Alpers-Huttenlocher Syndrome:
- Autosomal recessive
- Features: neurological regression, intractable seizures, liver disease, ataxia
- Liver failure can be triggered or worsened by valproate
- Diagnosis:
- Plasma and CSF lactate (elevated in respiratory chain defects)
- Lactate:pyruvate ratio > 25 (respiratory chain defect)
- Amino acids: elevated alanine (surrogate for elevated pyruvate)
- Muscle biopsy: "ragged red fibers" on modified Gomori trichrome; COX-negative fibers on cytochrome oxidase stain; electron microscopy: mitochondrial proliferation
- Liver biopsy: microvesicular steatosis + mitochondrial proliferation + Mito DNA depletion
- POLG gene sequencing (definitive)
Treatment:
- Remove valproate IMMEDIATELY if suspected
- Supportive care with NAC (as antioxidant)
- CoQ10, riboflavin, thiamine (mitochondrial cofactors - modest benefit)
- Low-fat, high-carbohydrate diet
- LT is GENERALLY CONTRAINDICATED when CNS/muscle involvement is present because:
- Post-transplant immunosuppression may accelerate neurological decline
- Brain and muscle disease is not corrected by liver replacement
- Exception: some POLG patients with purely hepatic disease + very early CNS involvement may benefit
SECTION 12: MONITORING CHECKLIST
Admission Investigations (Complete)
Blood:
- PT, INR, aPTT, fibrinogen
- Factor V level
- LFTs: AST, ALT, GGT, ALP, total + direct bilirubin
- Serum albumin, total protein
- CBC + differential + reticulocyte count
- BMP: Na, K, Cl, CO₂, BUN, creatinine, glucose
- Serum magnesium, phosphate
- Serum uric acid
- Arterial blood gas + lactate
- Arterial ammonia (arterial > venous for accuracy)
- Acetaminophen level (always)
- Toxicology screen (urine + blood)
- Ceruloplasmin, serum copper, urine copper (24h if possible)
- HAV IgM, HBsAg, anti-HBc IgM, HBV DNA, HCV RNA, HEV IgM/RNA
- HSV PCR (blood + CSF in neonates)
- EBV PCR, CMV PCR, adenovirus PCR, enterovirus PCR
- ANA, ASMA, anti-LKM1, IgG, anti-SLA
- Plasma amino acids, urine organic acids
- Acylcarnitine profile
- Serum ferritin, transferrin saturation
- Alpha-1-antitrypsin level + phenotype
- Blood type and screen (for potential transfusion/LT)
- HIV serology (pre-LT evaluation)
Urine:
- Urinalysis + urine culture
- Urine copper (24h collection)
- Urine reducing substances (Clinitest)
- Urine organic acids
CSF (if neonatal or CNS involvement):
- Cell count, protein, glucose
- HSV PCR, enterovirus PCR
- Lactate
Imaging:
- Liver + portal/hepatic Doppler ultrasound
- CT brain without contrast (cerebral edema, hemorrhage)
- Chest X-ray
- MRI abdomen (if GALD suspected - extrahepatic iron)
Sources:
- Yamada's Textbook of Gastroenterology, 7th ed. (Chapter 90 - Acute Liver Failure, ~25 pages)
- Robbins & Kumar Basic Pathology (Morphology + Clinical Features of ALF)
- Current Surgical Therapy, 14th ed. (ALF chapter)
- Sabiston Textbook of Surgery, 26th ed. (ALF and LT)
- Bradley and Daroff's Neurology in Clinical Practice (Hepatic Encephalopathy, Neonatal ALF)
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma (Metabolic encephalopathy)
- Bailey and Love's Short Practice of Surgery, 28th ed. (King's College Criteria, ALF)
- Goldman-Cecil Medicine, International ed. (ALF treatment)
- Recent PubMed: NASPGHAN Consensus Statement on PALF (Squires et al., JPGN 2022, PMID 34347674); ISPGHAN Consensus Recommendations (Lal et al., Hepatol Int 2024, PMID 39212863)
This is a shared conversation. Sign in to Orris to start your own chat.