Aetiopathogenesis and management of carcinoma of stomach
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gastric cancer" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have comprehensive content. Let me compile the full answer with all the information gathered.
Carcinoma of the Stomach: Aetiopathogenesis and Management
1. Epidemiology
Gastric cancer is one of the most common causes of cancer death worldwide. Incidence varies markedly:
- UK: ~15 per 100,000 per year
- USA: ~10 per 100,000 per year
- Eastern Europe: ~40 per 100,000 per year
- Japan: ~70 per 100,000 per year (highest reported)
- Men are more affected than women; incidence rises with age
In the West, total incidence is declining at ~1% per year - this reduction exclusively affects distal and body cancers, while proximal/gastro-oesophageal junction (GOJ) cancers are increasing. Distal gastric cancer is more common in lower socioeconomic groups; proximal cancer increasingly affects higher socioeconomic groups.
2. Aetiopathogenesis
Gastric cancer is a multifactorial disease. The main aetiological factors are:
2a. Helicobacter pylori
- The most important infectious risk factor
- Associated primarily with carcinoma of the body and distal stomach (not proximal)
- Causes chronic active gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → carcinoma (the Correa cascade)
- Sufficient epidemiological evidence to classify it as a Group I carcinogen (WHO)
- Proximal gastric cancer is notably NOT associated with H. pylori
2b. Dietary Factors
- High salt intake (preserved, salted, smoked foods)
- Deficiency of antioxidants (vitamins C and E)
- Exposure to N-nitroso compounds (nitrates and nitrites in food/water → converted to nitrosamines in hypochlorhydric stomach)
- Evidence: incidence among Japanese families in the USA declines toward US rates - clearly environmental/dietary
2c. Pre-malignant Conditions
| Condition | Risk |
|---|---|
| Chronic atrophic gastritis (with pernicious anaemia) | 6-fold increased risk, particularly fundal carcinoma |
| Gastric adenomatous polyps | Increased risk |
| Intestinal metaplasia | Pre-malignant step in Correa cascade |
| Previous peptic ulcer surgery (Billroth II / Pólya gastrectomy, gastroenterostomy, pyloroplasty) | ~4x average risk - bile reflux promotes intestinal metaplasia |
| Gastric remnant (stump) after partial gastrectomy | Increased risk after 15-20 years |
2d. Other Environmental Factors
- Cigarette smoking
- Dust ingestion from industrial processes (coal mining areas)
- Obesity and higher socioeconomic status (proximal cancer specifically)
2e. Genetic / Molecular Factors
- CDH1 mutation: Hereditary diffuse gastric cancer (autosomal dominant); E-cadherin loss promotes diffuse-type tumour
- Tumour suppressor genes: Loss of p53, APC, RUNX3
- HER2 (ERBB2) amplification: Present in ~15-20% of gastric cancers; targetable with trastuzumab
- MSI (microsatellite instability): ~15% of cases; better prognosis; responsive to immune checkpoint inhibitors
- PIK3CA, FGFR2, VEGFR alterations: Targets for emerging therapies
- EBV-associated gastric cancer: ~10% of cases; distinct molecular subtype
2f. Lauren Classification (Histopathological Types)
Two distinct types with different pathogenesis:
| Feature | Intestinal Type | Diffuse Type |
|---|---|---|
| Gross appearance | Polypoidal/ulcerated | Infiltrating (linitis plastica) |
| Histology | Gland-forming | Signet-ring cells, poorly cohesive |
| Pathogenesis | Sequential (Correa cascade): atrophic gastritis → metaplasia → dysplasia | De novo, CDH1 mutation |
| H. pylori association | Strong | Less clear |
| Incidence trend | Declining | Stable |
| Prognosis | Better | Worse |
| Spread | Direct/blood | Submucosal/subserosal lymphatics early |
3. Pathology
Macroscopic Classification (Borrmann)
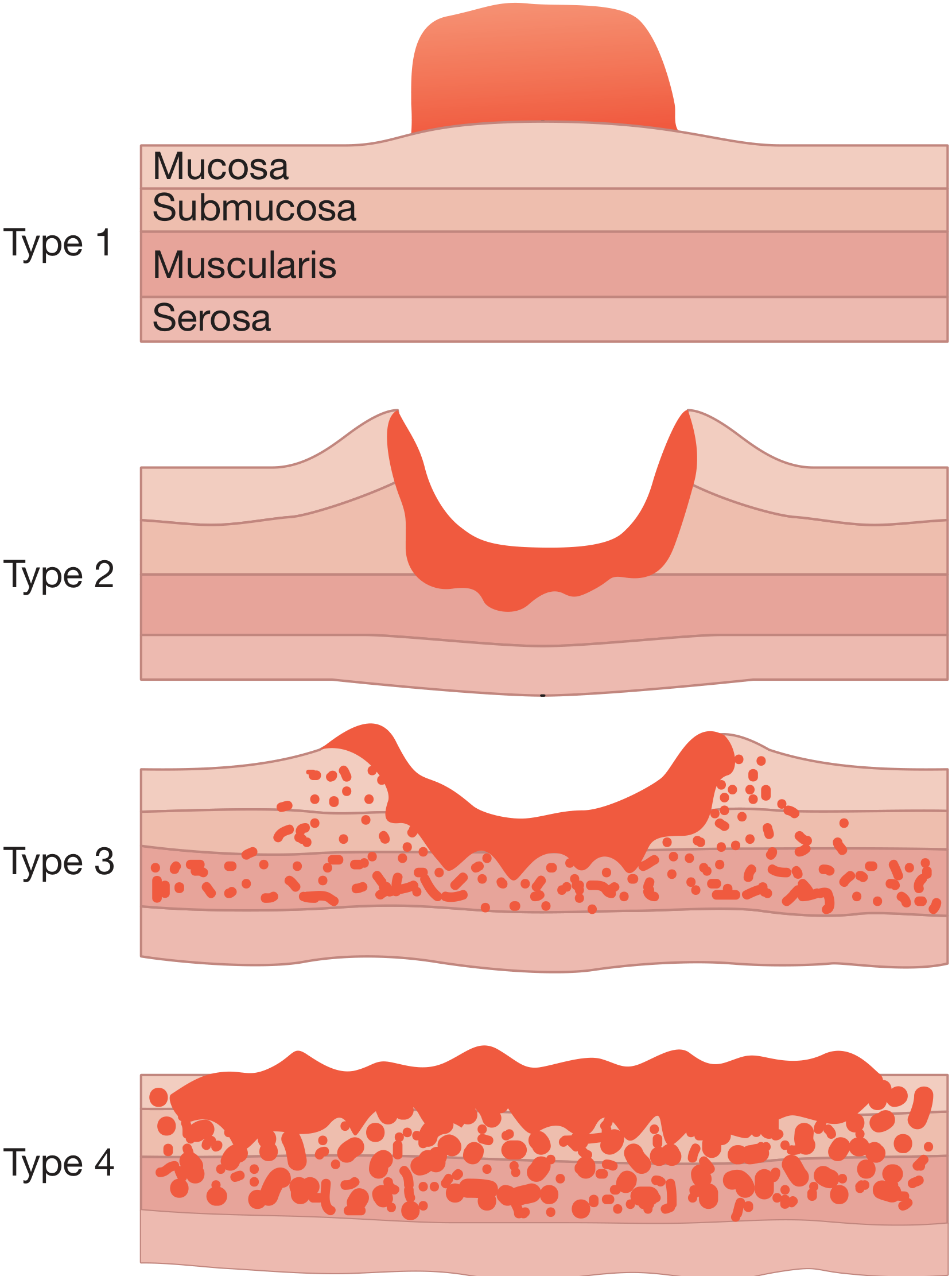
Figure: Borrmann classification - Type 1 (polypoid), Type 2 (ulcerating with defined margins), Type 3 (infiltrating/ulcerating), Type 4 (diffuse infiltrating/linitis plastica)
- Type 1: Polypoid - encroaches into lumen
- Type 2: Ulcerating with clearly defined margins
- Type 3: Infiltrating/ulcerating
- Type 4: Diffuse infiltration - linitis plastica (leather-bottle stomach)
Early vs Advanced Gastric Cancer
- Early gastric cancer (EGC): Confined to mucosa ± submucosa regardless of nodal status; associated with high cure rates
- Type I: Protruded
- Type IIa: Superficial elevated
- Type IIb: Flat
- Type IIc: Superficial depressed
- Type III: Excavated/ulcerated
- Advanced gastric cancer: Invades into muscularis propria or beyond
Histological Types
- Adenocarcinoma (>90%): intestinal or diffuse (Lauren)
- Signet-ring cell carcinoma: mucin displaces nucleus to periphery - aggressive, diffuse type
- Mucinous carcinoma
- Rare: Squamous, adenosquamous, undifferentiated
4. Spread of Carcinoma of the Stomach
Direct Spread
Tumour penetrates muscularis propria → serosa → adjacent organs (pancreas, colon, liver). The diffuse type penetrates the gastric wall early via the submucosal and subserosal lymphatic plexus.
Lymphatic Spread
- By both permeation and embolic routes
- Follows the nodal tiers defined by the lymphatic drainage
- Can reach supraclavicular nodes (left: Troisier's/Virchow's sign)
- Unlike breast cancer, nodal involvement does not necessarily imply systemic dissemination
Blood-Borne Spread
- First to the liver, then to lungs and bones
- Uncommon in the absence of nodal disease
Transperitoneal Spread
- Occurs once tumour reaches serosa
- Indicates incurability
- May cause malignant ascites
- Palpable rectal shelf (Blumer's shelf) on PR examination
- Krukenberg tumours: Transcoelomic spread to ovaries (signet-ring cell type)
- Sister Joseph's nodule: Spread to umbilicus
5. TNM Staging (UICC 8th Edition)
| T Stage | Description |
|---|---|
| Tis | Carcinoma in situ / high-grade dysplasia |
| T1a | Lamina propria or muscularis mucosae |
| T1b | Submucosa |
| T2 | Muscularis propria |
| T3 | Subserosa |
| T4a | Perforates serosa |
| T4b | Invades adjacent structures |
| N Stage | Description |
|---|---|
| N0 | No regional nodes |
| N1 | 1-2 nodes |
| N2 | 3-6 nodes |
| N3a | 7-15 nodes |
| N3b | ≥16 nodes |
| Stage | TNM |
|---|---|
| IA | T1N0M0 |
| IB | T1N1M0 or T2N0M0 |
| IIA | T1N2, T2N1, T3N0 |
| IIB | T1N3, T2N2, T3N1, T4aN0 |
| IIIA-C | Various combinations |
| IV | Any T, Any N, M1 |
6. Clinical Features
Early gastric cancer: Often asymptomatic; may mimic benign dyspepsia (hence, high index of suspicion needed)
Advanced gastric cancer:
- Anorexia, weight loss (often profound)
- Dyspeptic symptoms, early satiety, bloating
- Iron-deficiency anaemia (occult tumour bleeding)
- Dysphagia (cardia involvement), vomiting (pyloric obstruction)
- Gastric outlet obstruction (metabolic alkalosis, but less marked than duodenal ulcer obstruction)
- Paraneoplastic: Thrombophlebitis migrans (Trousseau's sign), DVT
- Signs of advanced disease: Virchow's node, epigastric mass, hepatomegaly, ascites, Blumer's shelf
7. Investigation and Diagnosis
- Upper GI endoscopy with multiple biopsies: gold standard; all gastric ulcers need biopsy and endoscopic follow-up
- CT chest/abdomen/pelvis: Staging and assessment of resectability
- Endoscopic ultrasound (EUS): Best for T and N staging of localised disease
- Staging laparoscopy: Mandatory before planned curative resection - detects peritoneal disease and positive cytology (M1) that CT misses
- PET-CT: Useful for detecting occult distant metastases (not standard for diffuse/signet-ring cell types, which are FDG-negative)
- HER2 testing (IHC ± FISH): On all advanced adenocarcinomas - guides use of trastuzumab
- MSI/MMR testing: Guides immune checkpoint inhibitor therapy
- Serum tumour markers: CEA, CA 19-9, CA 72-4 (limited sensitivity/specificity; useful for monitoring)
8. Management
8a. Surgical Management (Curative Intent)
Surgery is the only potentially curative treatment.
Subtotal (distal) gastrectomy:
- For tumours of the antrum/distal stomach
- Equivalent oncological outcomes to total gastrectomy for distal tumours
- Roux-en-Y or Billroth II reconstruction
Total gastrectomy:
- For proximal, GOJ, and diffuse tumours involving the whole stomach
- Roux-en-Y oesophago-jejunostomy
- Achieves 5-year survival in selected patients
Extent of lymph node dissection (D1 vs D2):
- D1: Removal of perigastric N1 nodes
- D2: Removal of N1 + N2 nodes (nodes around principal arterial trunks - left gastric, common hepatic, splenic, coeliac)
- D2 gastrectomy is the standard in Japan and recommended in specialist centres; associated with improved survival in experienced hands
- Spleen and distal pancreas are now generally preserved (spleen-preserving D2) unless directly involved, as routine pancreatosplenectomy increases morbidity without survival benefit
Endoscopic treatment:
- Endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) for select EGC (T1a, well-differentiated, <2 cm, no ulceration, no LVI) - widely practiced in Japan
8b. Perioperative (Neoadjuvant + Adjuvant) Chemotherapy
- FLOT protocol (5-FU, leucovorin, oxaliplatin, docetaxel): Currently the standard perioperative regimen in Europe/UK for resectable gastric/GOJ cancer; shown to be superior to ECF/ECX in the FLOT4 trial
- ECF/ECX/EOX: (epirubicin, cisplatin/oxaliplatin, 5-FU/capecitabine) - older UK/European standard (MAGIC trial)
- Adjuvant S-1 (Japan) or CAPOX after D2 resection: Standard in Asian centres
8c. Advanced/Metastatic Disease
First-line chemotherapy:
- Platinum + fluoropyrimidine backbone (cisplatin/oxaliplatin + 5-FU/capecitabine)
- Addition of trastuzumab if HER2-positive (ToGA trial: improved OS from 11.1 to 13.8 months)
Immune checkpoint inhibitors (recent evidence):
- Nivolumab (PD-1 inhibitor) + chemotherapy: CheckMate 649 trial showed significant OS benefit, particularly in PD-L1 CPS ≥5 tumours
- Pembrolizumab (KEYNOTE-590, KEYNOTE-859): Benefit in PD-L1 positive disease
- A 2025 meta-analysis in Frontiers in Immunology confirmed that first-line immune checkpoint inhibitors with chemotherapy significantly improve outcomes in advanced gastric and GOJ adenocarcinoma
Second-line:
- Ramucirumab (anti-VEGFR2) ± paclitaxel (REGARD and RAINBOW trials)
- Irinotecan-based regimens
8d. Peritoneal Disease (HIPEC / CRS)
For selected patients with limited peritoneal metastases (PCI <6) after good response to systemic therapy, cytoreductive surgery (CRS) + hyperthermic intraperitoneal chemotherapy (HIPEC) may be considered - preferably in a trial setting. Evidence remains limited (GASTRIPEC trial showed PFS benefit but no OS benefit; Chinese phase III showed OS benefit for HIPEC arm).
8e. Palliative Surgery
- Resection of the primary tumour: Best palliation for pain, obstruction, and bleeding
- Gastrojejunostomy bypass: For unresectable obstructing distal lesions
- Palliative intubation/stenting: For obstructing cardia lesions
- The REGATTA trial showed no benefit of palliative gastrectomy followed by chemotherapy vs chemotherapy alone in patients with single metastatic site
8f. Radiotherapy
- Limited role in gastric cancer compared to other GI malignancies
- Used in the INT-0116 trial (chemoradiation post-resection - more of a US practice)
- Can palliate bleeding, pain, or locally advanced disease
8g. Endoscopic Palliation
- Laser therapy, argon plasma coagulation, stenting for obstruction
- Endoscopic haemostasis for tumour bleeding
9. Prognosis
- Overall 5-year survival: 5-10% in the West (due to late presentation)
- Japan (due to screening and early diagnosis): significantly better outcomes
- Early gastric cancer treated surgically: >90% 5-year survival
- Nodal involvement is the single most important prognostic factor
- Diffuse type / linitis plastica: worse prognosis than intestinal type
- Positive peritoneal cytology (M1): median OS <12 months with systemic therapy alone
Sources: Bailey and Love's Short Practice of Surgery (28th Ed.), pp. 1191-1199; Pye's Surgical Handicraft (22nd Ed.), p. 274; Sabiston Textbook of Surgery; recent meta-analysis on checkpoint inhibitors in gastric cancer (PMID 40386769, Front Immunol 2025).
This is a shared conversation. Sign in to Orris to start your own chat.