Explain me 10 common heart diseases with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Searching the Web
ECG changes 10 common heart diseases images atrial fibrillation MI heart block
Finding Sources
Finding Sources
Reading Web Page
https://mesimedical.com/insights/frequently-diagnosed-condit…
Finding Sources
Searching the Web
ECG images STEMI atrial fibrillation heart block ventricular tachycardia LVH WPW wikimedia commons
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG examples images LITFL complete heart block LVH LBBB pericarditis long QT syndrome wikimedia
Loading Image
Searching the Web
ECG atrial fibrillation ventricular tachycardia complete heart block LVH WPW long QT images site:litfl.com OR site:wikimedia.org
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
ECG atrial fibrillation STEMI inferior complete heart block WPW long QT pericarditis images wikimedia commons
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive guide to 10 common heart diseases with their ECG changes and images.
10 Common Heart Diseases: ECG Changes and Images
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing transmural (full-thickness) myocardial necrosis. The most time-critical cardiac emergency.
Key ECG Changes:
- ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads (in the territory of the occluded artery)
- Hyperacute T waves - the earliest sign, tall and broad before ST elevation
- Pathological Q waves - develop within hours to days (>40 ms wide, >25% of R wave height) indicating completed infarction
- Reciprocal ST depression in opposite leads
- T wave inversion in the sub-acute phase
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Inferior | II, III, aVF | RCA |
| Anterior | V1-V4 | LAD |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | Tall R + ST depression in V1-V3 | RCA / LCx |
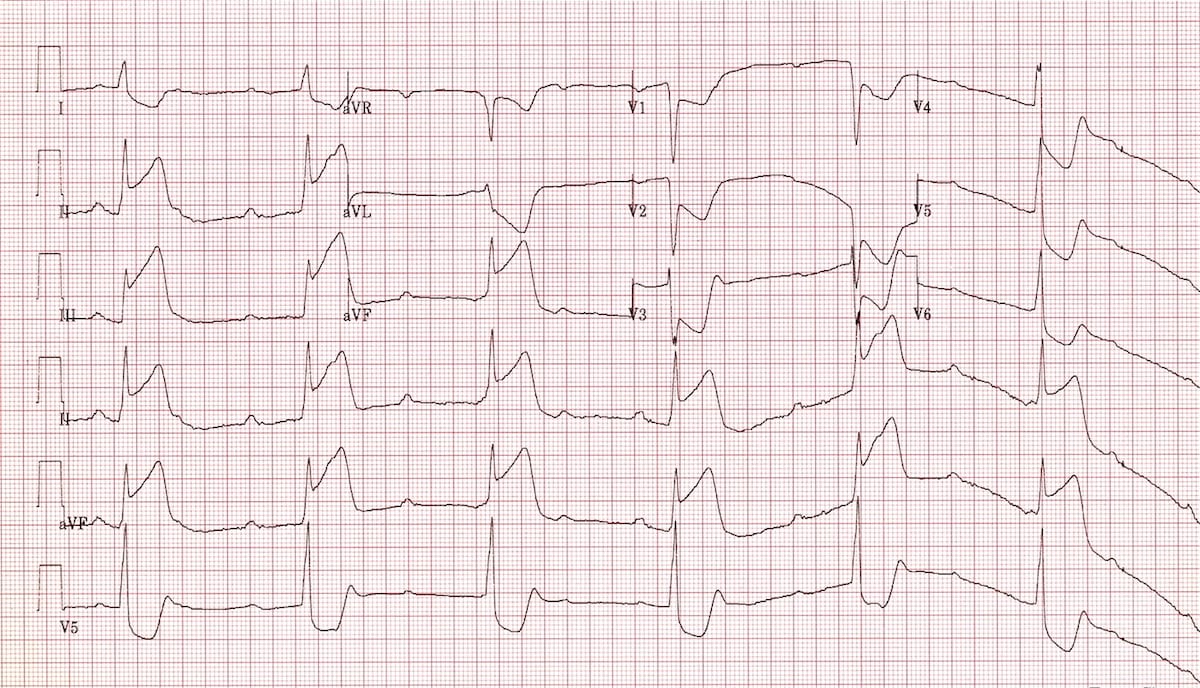
ECG showing Inferior STEMI with concurrent Complete Heart Block (note ST elevation in II, III, aVF and complete AV dissociation):
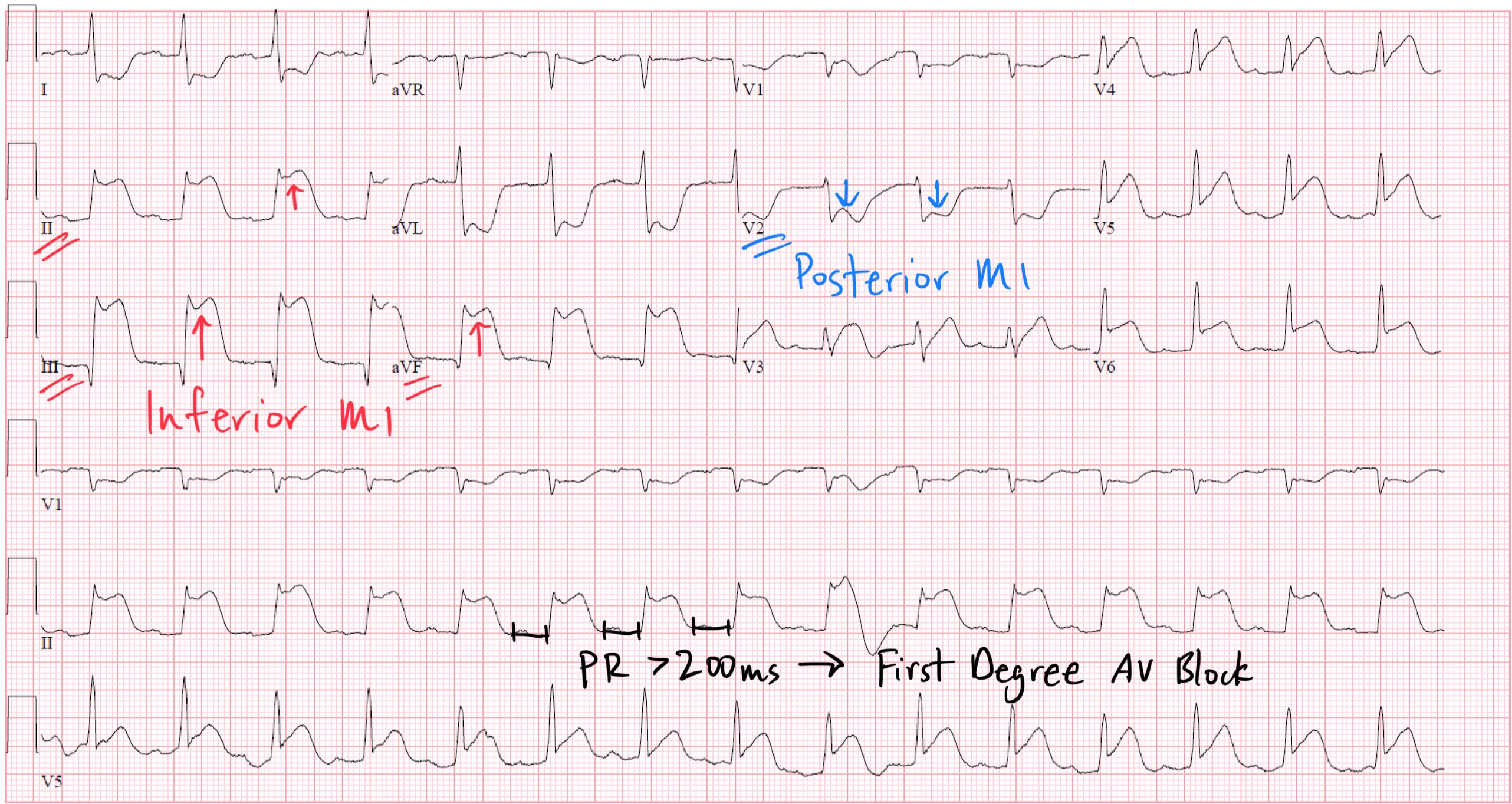
Annotated ECG showing Inferior + Posterior MI with First-Degree AV Block:
2. Non-ST Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
What it is: Partial coronary occlusion causing subendocardial ischemia without full-thickness necrosis. NSTEMI differs from unstable angina only by elevated troponins.
Key ECG Changes:
- ST depression (horizontal or downsloping) - key ischemic marker
- T wave flattening or inversion - especially in the affected territory
- Hyperacute T waves transiently in some cases
- No ST elevation (by definition)
- ECG can be entirely normal in up to 50% of NSTEMI cases - serial ECGs and troponins are required
- Transient ST elevation that resolves may also be seen
3. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized electrical activity in the atria causing an irregularly irregular ventricular response. The most common pathologic tachyarrhythmia.
Key ECG Changes:
- Absent P waves - replaced by fibrillatory (f) waves, best seen in V1 (fine/coarse undulation at ~350-600 bpm)
- Irregularly irregular RR intervals - the hallmark finding
- Narrow QRS complexes (unless aberrant conduction or bundle branch block coexists)
- Ventricular rate typically 100-160 bpm if untreated
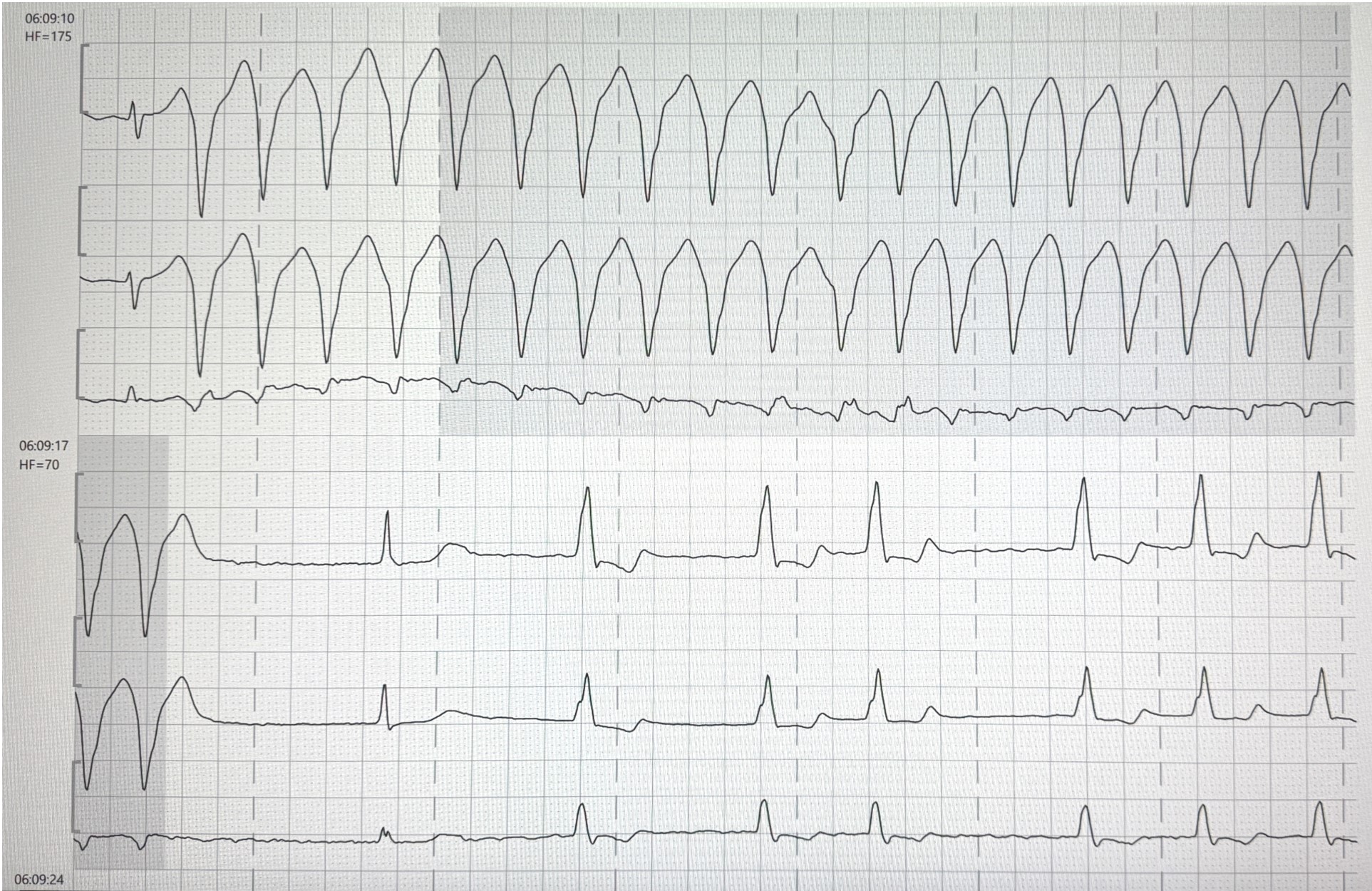
ECG showing Ventricular Tachycardia (top) converting to sinus rhythm after defibrillation, demonstrating wide-complex tachycardia vs normal rhythm:
4. Ventricular Tachycardia (VT)
What it is: Three or more consecutive beats originating in the ventricle at a rate >100 bpm. Frequently occurs with structural heart disease, ischemia, or electrolyte disturbances. Life-threatening.
Key ECG Changes:
- Wide QRS complexes (>120 ms, typically >140 ms)
- Rate 110-250 bpm, usually regular
- AV dissociation - P waves march through independently of QRS (pathognomonic when present)
- Fusion beats and capture beats - confirm VT
- Concordance - all precordial QRS complexes pointing in the same direction (positive or negative concordance)
- LBBB morphology suggests RV origin; RBBB morphology suggests LV origin
- Negative concordance (all precordial leads negative) strongly favors VT
ECG showing monomorphic ventricular tachycardia at 175 bpm, then post-cardioversion rhythm:
5. Left Bundle Branch Block (LBBB)
What it is: Failure of conduction through the left bundle branch, causing abnormal ventricular depolarization. May be caused by ischemia, hypertension, cardiomyopathy, or aortic stenosis. New LBBB with chest pain requires urgent evaluation for MI.
Key ECG Changes:
- QRS duration ≥120 ms (broad complexes)
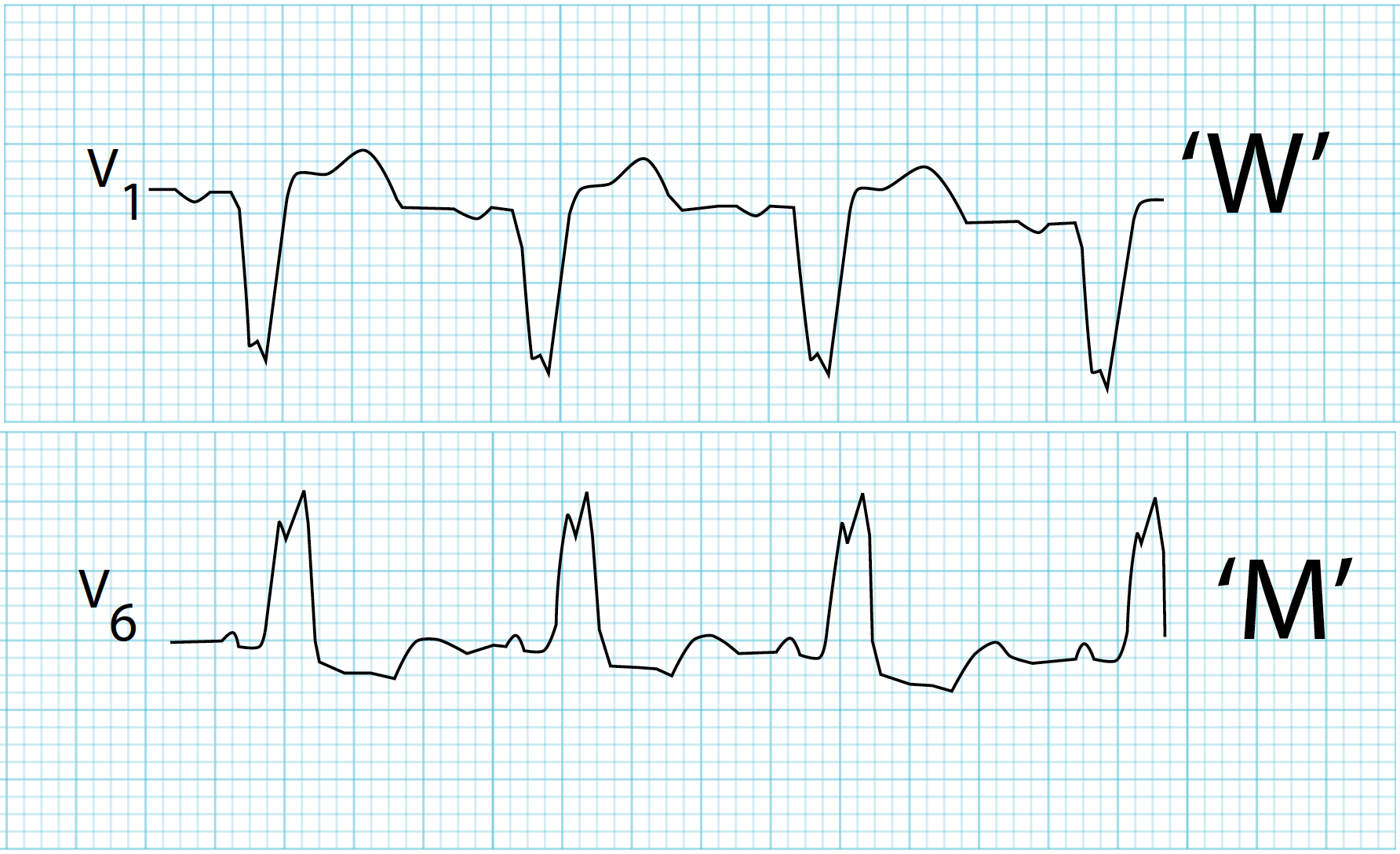
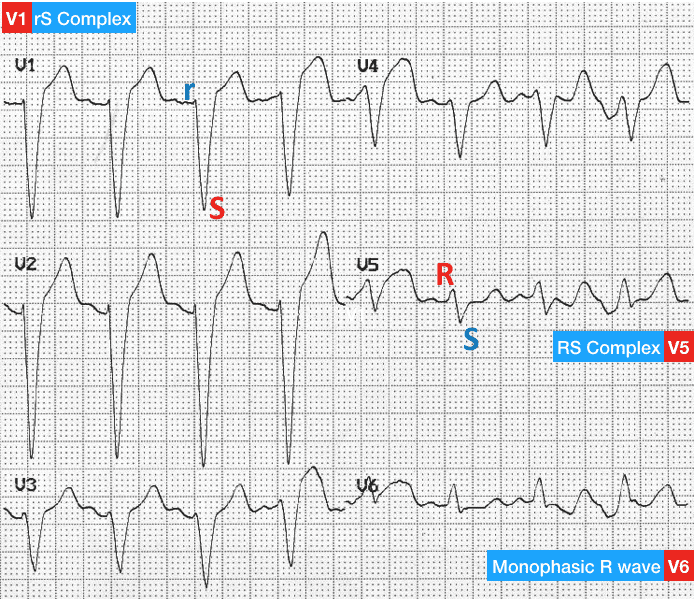
- Dominant S wave in V1 (rS complex - "W" pattern in V1)
- Broad monophasic R wave in V5-V6 ("M" pattern / no Q wave laterally)
- Absence of septal Q waves in I, aVL, V5-V6
- Appropriate discordance - ST and T waves point opposite to the QRS (ST depression + T inversion where tall R; ST elevation where deep S)
LBBB ECG pattern - classic "W" in V1 and "M" in V6:
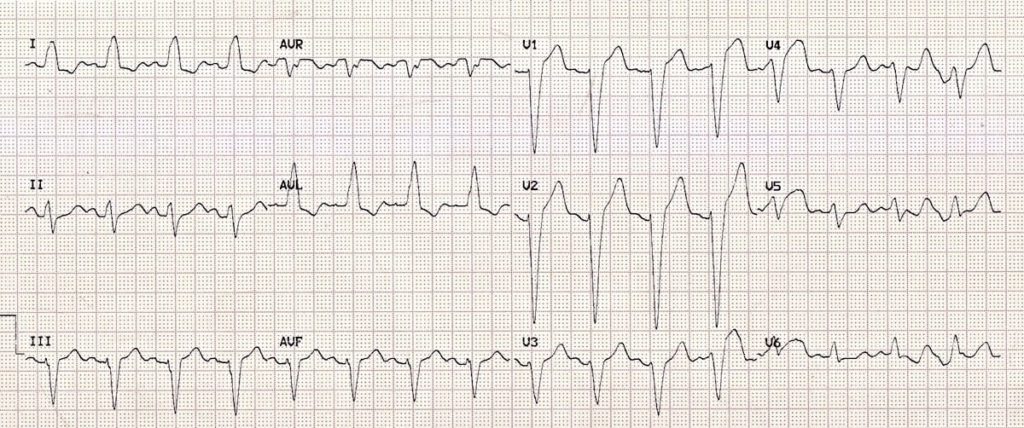
Full 12-lead LBBB showing rS in V1 and broad monophasic R in V6:
Full 12-lead LBBB example:
6. Complete (3rd Degree) AV Heart Block
What it is: Complete failure of conduction between atria and ventricles. The atria and ventricles beat independently. The ventricular rhythm is maintained by a slow junctional or ventricular escape rhythm. Causes include inferior MI, Lev/Lenegre disease, drugs (digoxin, beta-blockers), and Lyme disease.
Key ECG Changes:
- Complete AV dissociation - P waves and QRS complexes are completely independent
- Regular P waves at normal atrial rate (~60-100 bpm)
- Slow, regular escape rhythm - junctional (narrow QRS, 40-60 bpm) or ventricular (wide QRS, 20-40 bpm)
- No relationship between P waves and QRS - the PR interval varies randomly
- The ventricular rate is slower than the atrial rate
The Washington Manual of Medical Therapeutics notes that in complete heart block, none of the supraventricular impulses conduct to the ventricles, and the perfusing rhythm is maintained by junctional or ventricular escape.
7. Pericarditis
What it is: Inflammation of the pericardial sac, most commonly viral. Presents with sharp pleuritic chest pain relieved by leaning forward.
Key ECG Changes (evolve through 4 classic stages):
- Stage 1 (acute): Widespread saddle-shaped (concave) ST elevation in most leads (I, II, aVL, aVF, V3-V6) + PR depression (most specific sign) + PR elevation in aVR
- Stage 2: ST normalization, T waves flatten
- Stage 3: Diffuse T wave inversion
- Stage 4: ECG normalizes
Key distinguishing features from STEMI:
- ST elevation is diffuse (not in a single coronary territory)
- ST elevation is concave (saddle-shaped), not convex
- PR depression is present (absent in MI)
- No reciprocal changes in other territories (except aVR)
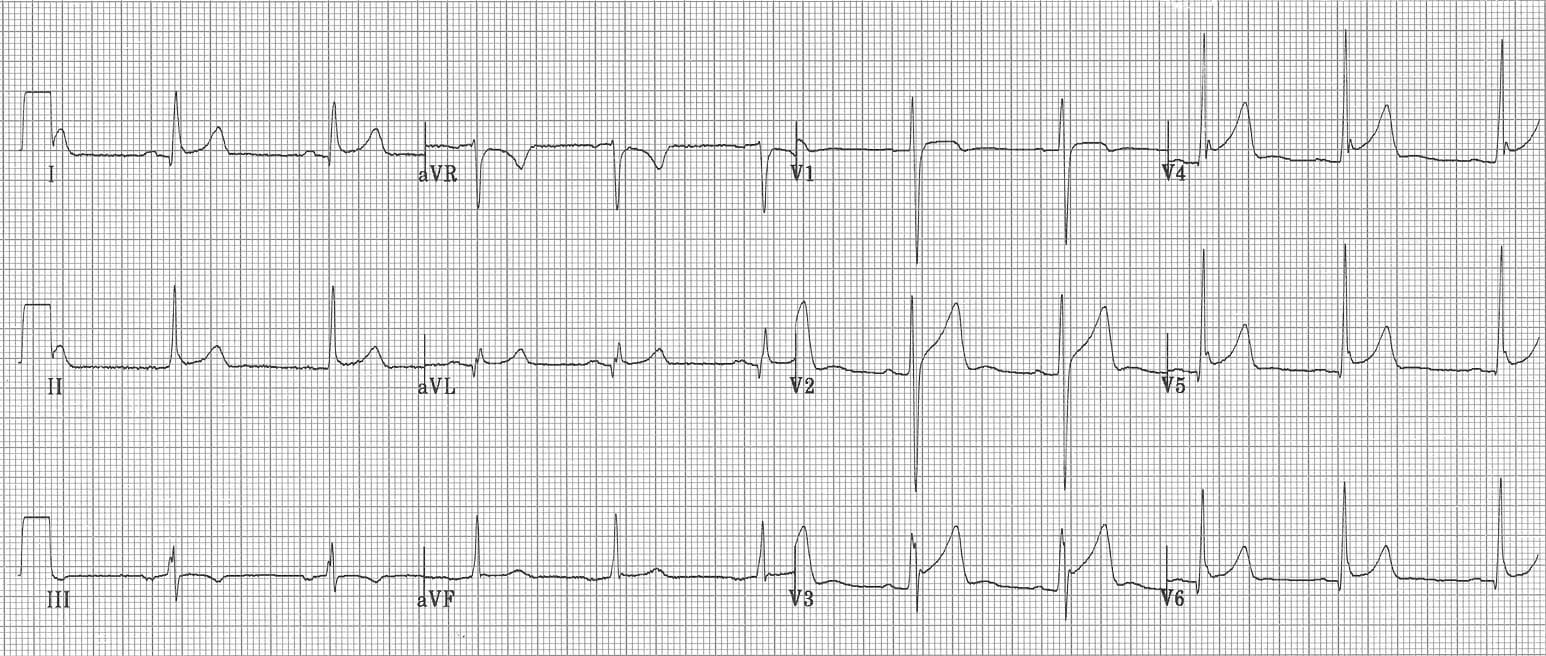
Classic pericarditis 12-lead ECG showing diffuse concave ST elevation and PR depression:
8. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular wall, typically due to longstanding hypertension, aortic stenosis, or hypertrophic cardiomyopathy. ECG has low sensitivity (~50%) but high specificity.
Key ECG Changes:
- High-voltage QRS complexes - classic voltage criteria:
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥35 mm
- Cornell: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- Left axis deviation
- ST depression and T wave inversion in lateral leads (I, aVL, V5-V6) - "LV strain" pattern
- Left atrial enlargement (bifid P wave in II, biphasic P in V1)
- Prolonged QRS (but <120 ms)
9. Wolff-Parkinson-White (WPW) Syndrome
What it is: A congenital accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Predisposes to AVRT and, if AF develops, potentially fatal rapid ventricular conduction.
Key ECG Changes (in sinus rhythm):
- Short PR interval (<120 ms) - impulse bypasses AV nodal delay
- Delta wave - initial slurred upstroke of the QRS (slow conduction through myocardium before normal His-Purkinje activation arrives)
- Wide QRS complex (≥120 ms) due to fusion of pre-excited and normally conducted impulses
- Secondary ST-T changes (discordant to the QRS, can mimic ischemia)
- Type A WPW: Dominant R wave in V1 (left-sided pathway)
- Type B WPW: Dominant S wave in V1 (right-sided pathway)
During AF in WPW: Extremely rapid, irregular wide-complex tachycardia ("irregularly irregular wide-complex tachycardia") - rates may exceed 200-300 bpm, risk of VF.
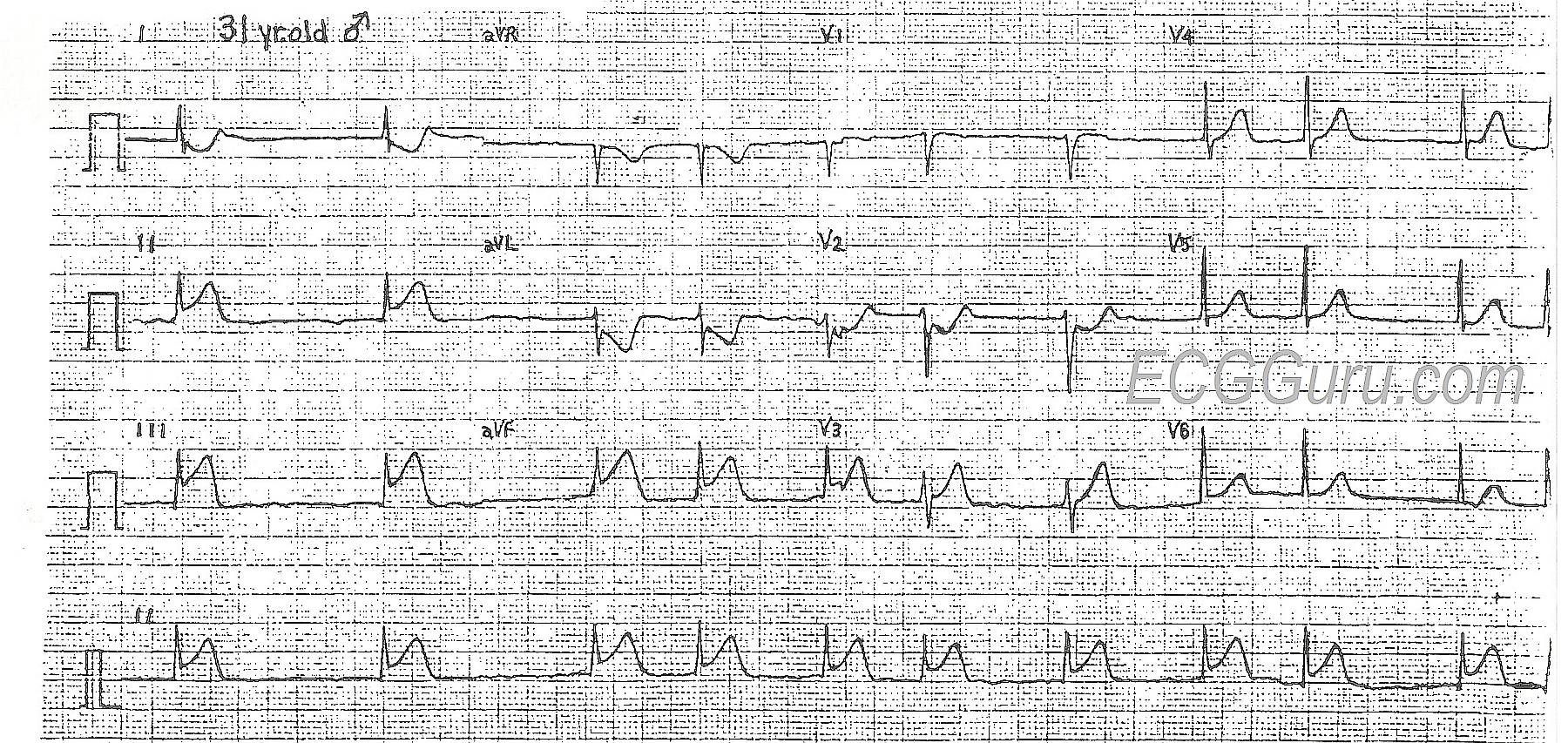
ECG of a 31-year-old male showing classic WPW features - short PR, delta waves, and secondary ST-T changes mimicking ischemia:
10. Long QT Syndrome (LQTS)
What it is: Prolonged ventricular repolarization predisposing to Torsades de Pointes (a polymorphic VT that can degenerate into VF). Can be congenital (ion channel mutations - LQT1, LQT2, LQT3 subtypes) or acquired (drugs, hypokalemia, hypomagnesemia, hypothyroidism).
Key ECG Changes:
- Prolonged QTc interval:
- Males: QTc >440 ms (borderline), >460 ms (abnormal)
- Females: QTc >460 ms (borderline), >480 ms (abnormal)
- QTc >500 ms - high risk of Torsades
- T wave morphology varies by subtype:
- LQT1: Broad-based T waves
- LQT2: Bifid/notched T waves
- LQT3: Long isoelectric ST segment, late peaked T wave
- Torsades de Pointes: Polymorphic VT with characteristic twisting of the QRS axis around the isoelectric line ("twisting of the points")
- U waves may be prominent (hypokalemia-related LQTS)
ECG showing Complete Heart Block with wide escape rhythm - illustrating complete AV dissociation (P waves and QRS complexes march independently):

Quick Reference Summary Table
| # | Condition | Key ECG Findings |
|---|---|---|
| 1 | STEMI | ST elevation in contiguous leads + Q waves + reciprocal changes |
| 2 | NSTEMI/UA | ST depression, T inversion, or normal ECG |
| 3 | Atrial Fibrillation | Absent P waves + irregularly irregular RR intervals |
| 4 | Ventricular Tachycardia | Wide QRS >120ms, rate >100 bpm, AV dissociation |
| 5 | LBBB | Wide QRS + "W" in V1 + "M" in V6 + no septal Q waves |
| 6 | Complete Heart Block | Complete AV dissociation + slow escape rhythm |
| 7 | Pericarditis | Diffuse saddle-shaped ST elevation + PR depression |
| 8 | LVH | High voltage + left strain pattern (ST depression V5-V6) |
| 9 | WPW | Short PR + delta wave + wide QRS |
| 10 | Long QT Syndrome | QTc >460-500 ms + abnormal T wave morphology |
Sources: Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine; The Washington Manual of Medical Therapeutics; LITFL ECG Library (litfl.com); ECGGuru.com
Clinical note: ECG findings must always be interpreted in the context of the full clinical picture - history, examination, and biomarkers. A normal ECG does not rule out MI (NSTEMI), and many ECG patterns overlap between conditions.
This is a shared conversation. Sign in to Orris to start your own chat.