Notes on endometriosis
Reading File
Finding Sources
Searching PubMed
endometriosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the material needed for comprehensive notes. Here they are:
Endometriosis - Clinical Notes
Definition
Endometriosis is a common chronic inflammatory condition defined by the presence of endometrial glands and stroma at extrauterine sites. It affects an estimated 5-10% of women of reproductive age and is found in nearly half of women with infertility.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Robbins & Kumar Basic Pathology
Epidemiology
- Predominantly a disease of reproductive age
- Higher incidence in women with infertility
- A significant proportion of affected women remain asymptomatic
- Gastrointestinal involvement occurs in 12-37% of cases
Pathogenesis
The exact mechanism remains elusive. Four leading theories:
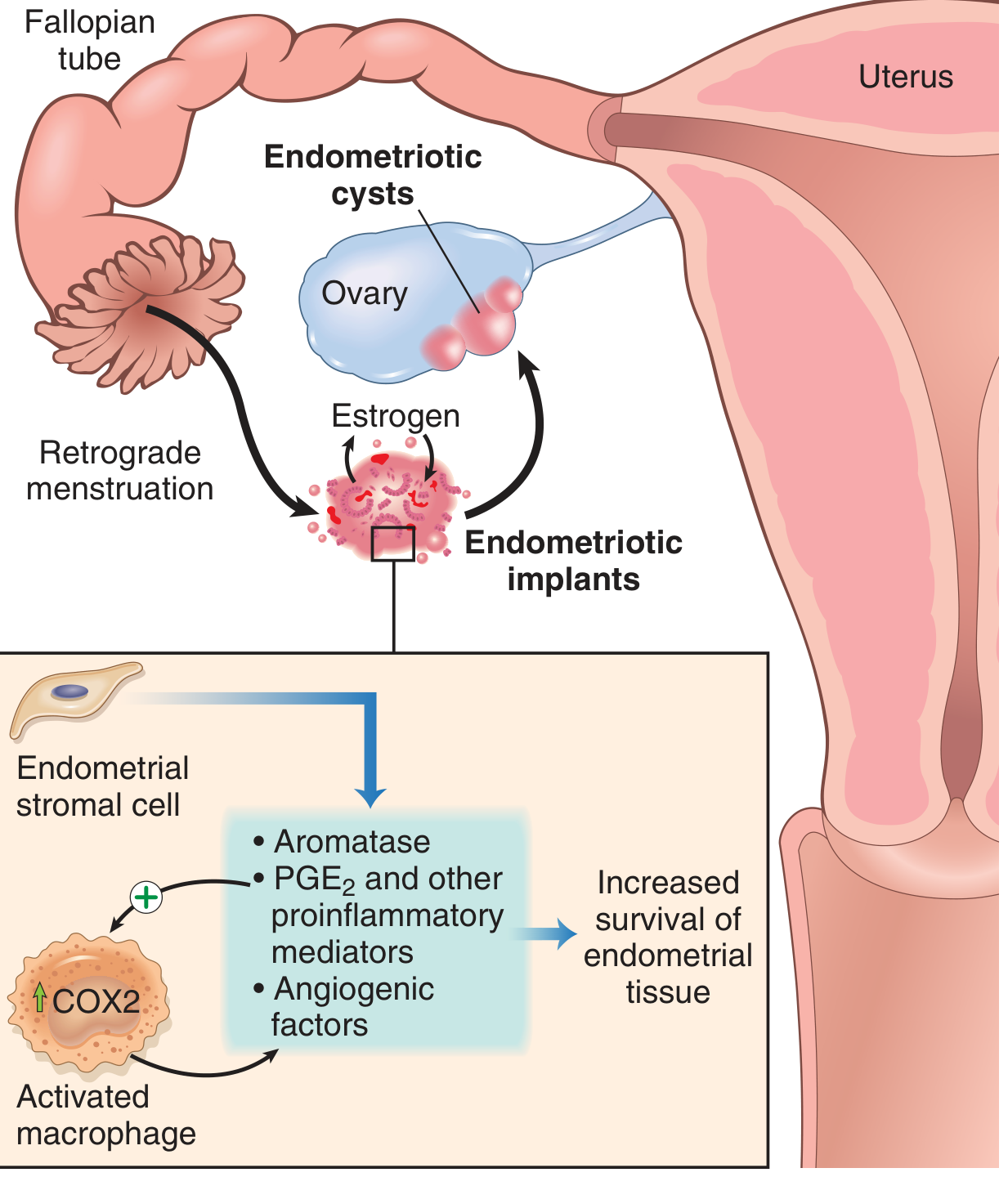
Pathogenesis of endometriosis: retrograde menstruation seeds implants; endometrial stromal cells and activated macrophages produce aromatase, PGE2, and angiogenic factors that sustain implant survival. - Robbins & Kumar Basic Pathology
| Theory | Mechanism |
|---|---|
| Regurgitation (Sampson's) | Retrograde menstruation via the fallopian tubes deposits endometrial tissue at ectopic pelvic sites - the most widely accepted |
| Benign metastasis | Haematogenous/lymphatic spread explains distant lesions (lung, bone, brain) |
| Coelomic metaplasia | Mesothelium of the pelvis/abdomen (from which Mullerian ducts derive) undergoes endometrial differentiation |
| Extrauterine stem cell | Bone marrow stem/progenitor cells differentiate into endometrial tissue |
Molecular drivers at implant level
Once established, endometriotic implants differ from eutopic endometrium:
- Elevated PGE2 and VEGF (proinflammatory, angiogenic)
- Recruited macrophages with upregulated COX-2 amplify the inflammatory loop
- High aromatase in stromal cells -> local estrogen production -> promotes implant survival
- Elevated matrix metalloproteinases (MMP) facilitating tissue invasion
Types of Endometriosis
Three main subtypes (Robbins):
- Superficial peritoneal endometriosis - small implants on peritoneal surface
- Ovarian endometriosis (endometriomas) - cystic masses filled with old haemorrhage ("chocolate cysts"), 3-5 cm, reported in 17-44% of women with endometriosis
- Deep infiltrating endometriosis (DIE) - tissue >5 mm beneath the peritoneum; involves uterosacral ligaments, vagina, bowel, bladder, ureters; highest risk of malignant transformation
Sites of Involvement
Common (pelvic):
- Ovaries
- Uterosacral ligaments
- Pouch of Douglas
- Fallopian tubes
- Serosal surfaces and peritoneum
Bowel:
- Sigmoid colon and rectosigmoid are most common
- Small bowel loops, caecum also affected
- Serosal implants invade the muscularis propria - causes fibrosis, wall contraction, mass effect; mucosal surface usually remains intact
Distant (rare):
- Lungs - recurrent haemoptysis or pneumothoraces at time of menstruation
- Periumbilical tissues, laparotomy scars
Morphology
Macroscopic appearances:
- Classic "powder burn" or "gunshot" lesions: black, dark brown or bluish puckered nodules/cysts containing old haemorrhage, surrounded by fibrosis
- Atypical/"subtle" lesions: red implants (petechial, vesicular, flame-like), serous/clear vesicles, white plaques, yellow-brown peritoneal discolouration
- Endometriomas - ovarian cysts with thick, tar-like fluid ("chocolate cysts"); densely adherent to the peritoneum of the ovarian fossa and posterolateral uterus

Ovarian endometriosis: sectioned ovary showing large endometriotic ("chocolate") cyst. - Robbins & Kumar Basic Pathology
Microscopic diagnosis: requires both endometrial glands AND stroma at the ectopic site.
Laparoscopic Appearances
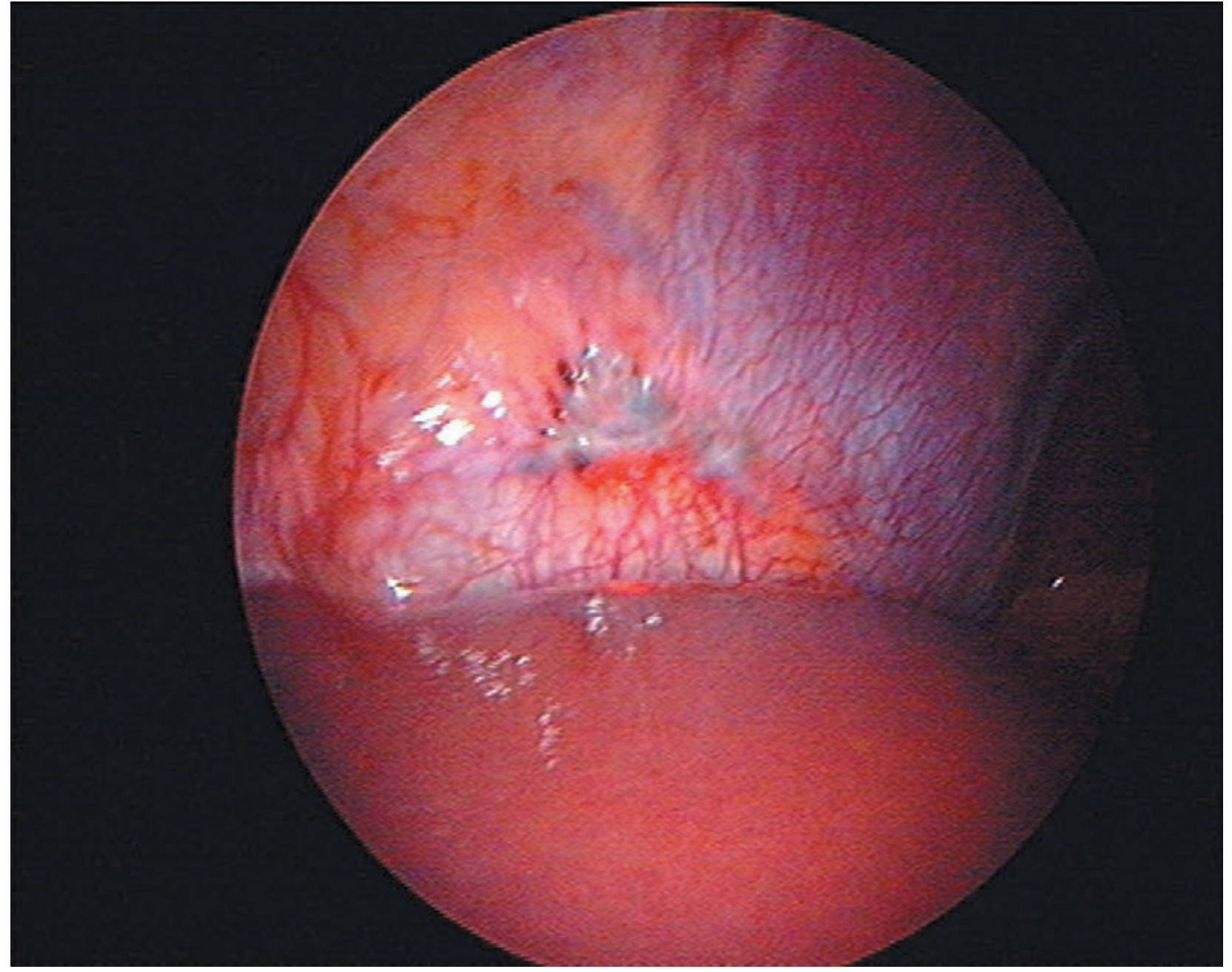
Endometriosis on the peritoneal surface of the diaphragm - a rare but recognised distant site. - Bailey and Love's
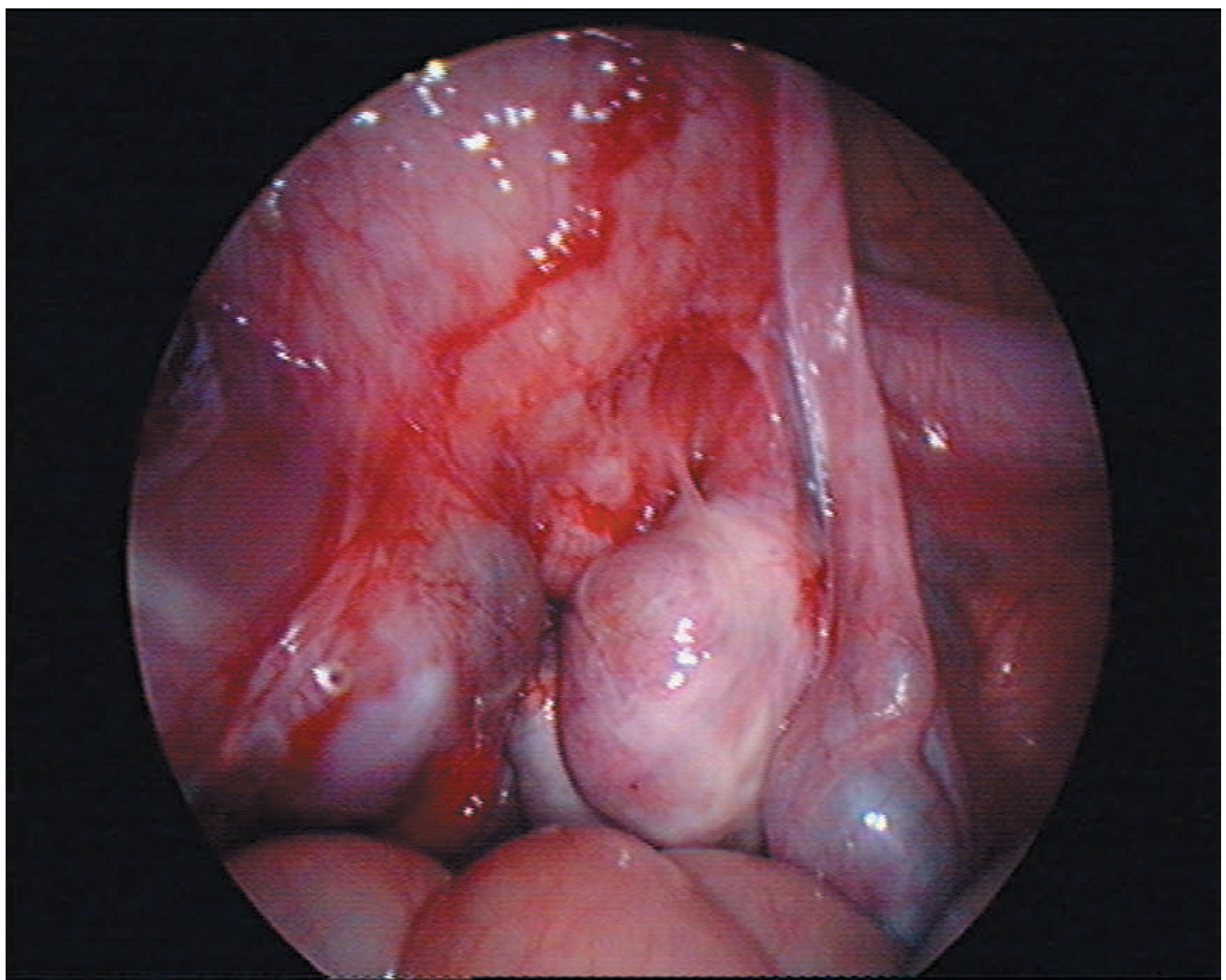
Bilateral ovarian endometriosis with pelvic adhesions. Note the marked distortion of pelvic anatomy. - Bailey and Love's
Clinical Features
Symptoms
| Domain | Symptoms |
|---|---|
| Pain | Dysmenorrhoea, chronic pelvic pain, deep dyspareunia, dyschezia (pain on defaecation), dysuria |
| Cyclical | Haematuria, rectal bleeding (haematochezia), haemoptysis (if thoracic) |
| Systemic | Fatigue |
| Reproductive | Infertility (presenting complaint in 30-40% of patients) |
- Pain is the most common symptom
- Symptoms correlate poorly with disease extent - significant disease may be asymptomatic
- Each symptom has overlapping differentials (IBS, interstitial cystitis, etc.)
Examination Findings (suggestive)
- Pelvic tenderness
- Fixed retroverted uterus
- Tender uterosacral ligaments
- Enlarged ovaries
- Deeply infiltrating nodules in the pouch of Douglas or uterosacral ligaments
- Visible blue-domed cystic lesions in the posterior fornix (vaginal DIE)
- Digital rectal examination: rectosigmoid involvement, lateral/dorsal extension (hypogastric vessel/nerve involvement)
- Note: examination may be entirely normal
Diagnosis
Gold standard: Laparoscopy with histological confirmation
Non-invasive imaging
| Modality | What it detects |
|---|---|
| Transvaginal/transrectal ultrasound | Reliable only for severe disease - endometriomas and deep pelvic endometriosis |
| MRI | Detects haemosiderin deposits in abdominal organs; shows low-signal fibrotic plaques; can demonstrate obliteration of the pouch of Douglas and rectosigmoid involvement |
| Sigmoidoscopy | Assesses level of bowel involvement; important for preoperative planning (distance from anal verge affects surgical risk) |
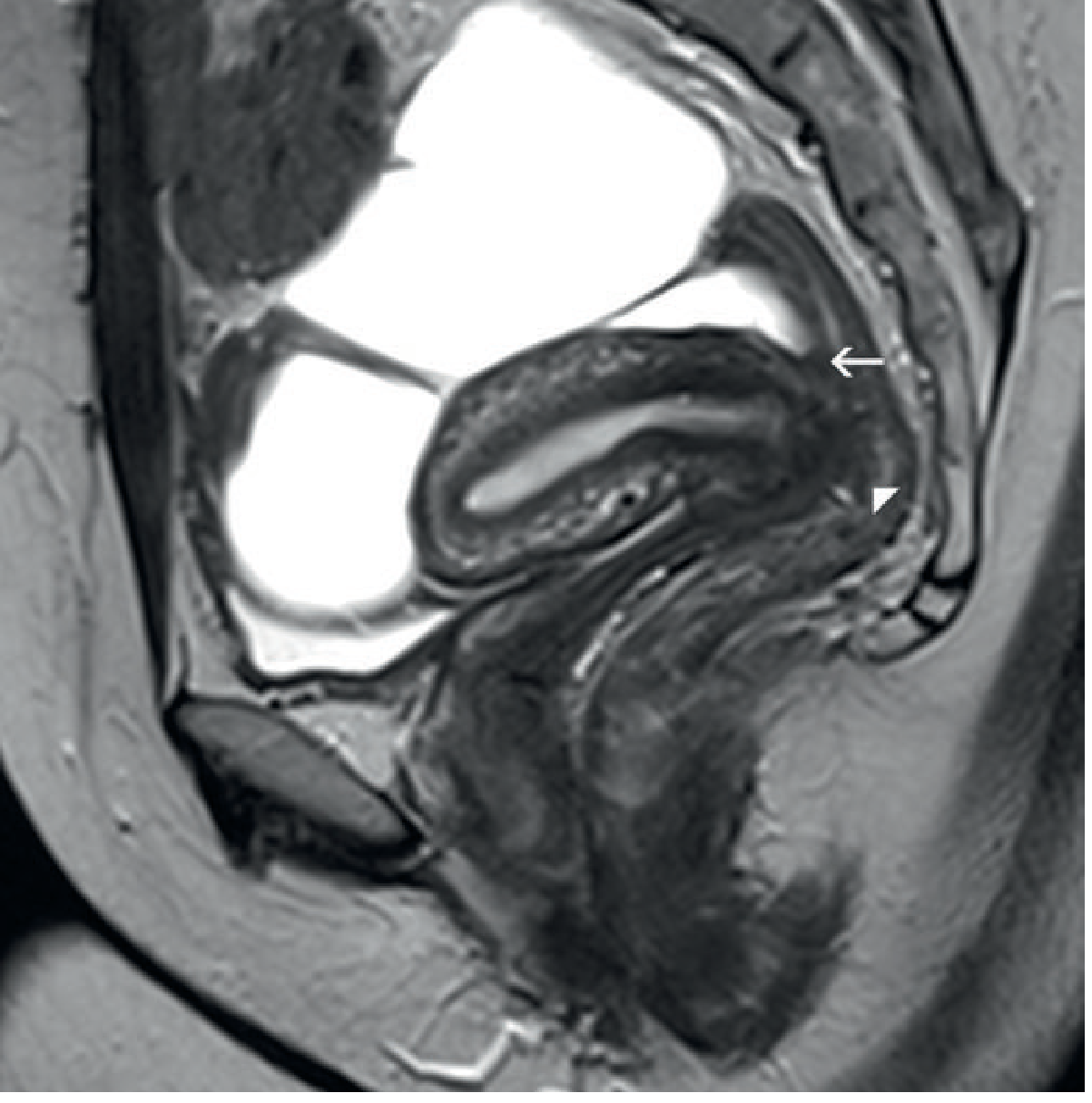
MRI pelvis (sagittal T2): low-signal nodularity obliterating the pouch of Douglas (arrow) with tethering of the rectal wall to a deep rectovaginal endometriotic nodule (arrowhead). Absence of submucosal anterior rectal wall oedema suggests full-thickness infiltration is not yet present. - Grainger & Allison's Diagnostic Radiology
Classification
- Various operative classification systems exist (e.g., rASRM staging)
- Poor correlation between classification/disease extent and symptom severity
Management
Treatment options are limited because the underlying cause remains uncertain. Management is guided by symptoms, desire for fertility, and disease extent.
1. Conservative (Watchful waiting)
- Appropriate for asymptomatic or mildly symptomatic women
2. Medical Management
| Drug class | Examples | Mechanism |
|---|---|---|
| Simple analgesia | NSAIDs, paracetamol | Symptom control |
| Combined hormonal contraceptives | OCP | Suppress cyclical stimulation |
| Progestogens | Norethisterone, desogestrel | Suppresses endometrial activity |
| Levonorgestrel IUS | Mirena | Local progestogenic effect |
| GnRH agonists + add-back HRT | Leuprorelin + oestrogen/progestogen | Hypoestrogenic state suppresses disease; add-back minimises bone loss and menopause symptoms |
| COX-2 inhibitors | Celecoxib | Targets PGE2 pathway |
| Aromatase inhibitors | Letrozole | Reduces local oestrogen production in implants |
- GnRH agonists are effective but have significant side effects (hot flushes, bone density loss)
- Costly drugs may require prolonged courses
- Women often require multiple treatments
3. Surgical Management
Minimally invasive (laparoscopic):
- Ablation or excision of endometriotic lesions
- Laparoscopic surgery is preferred over open approaches
Key surgical considerations:
- Proximity of disease to the ureter - risk of ureteric stricture, hydronephrosis, renal dysfunction
- Distance of bowel lesions from the anal verge: low rectal lesions (5-8 cm from anal verge) carry higher risk of anastomotic leak and transient neurogenic bladder dysfunction
- Repeat surgery increases risk: ureterolysis risk of ureteral ischaemia; repeated bowel shavings reduce bowel wall integrity (risk of fistula)
- Bowel integrity can be tested intraoperatively (air insufflation in water, methylene blue per rectum)
- Ureteral stents for bladder endometriosis near the trigone (removed at ~6 weeks); catheter for 8-10 days post-cystectomy
Definitive surgery:
- Hysterectomy + bilateral salpingo-oophorectomy + total excision of all endometriotic disease = best chance of cure, reserved for women who have completed their family
Complications and Risks
- Laparoscopic complications: bowel, bladder, ureteric injury (2 in 1000 women); risk higher with DIE
- Tubo-ovarian abscess (rare, from infected endometrioma)
- Bowel resection: risk of faecal peritonitis
Associations and Complications
- Infertility - 30-40% of patients present with this
- Malignant transformation - uncommon but recognised; mainly from DIE; endometrioid and clear cell carcinoma of the ovary are the most associated histological types
- Bowel obstruction (from fibrosis/adhesions)
- Hydronephrosis (ureteric involvement)
Recent Evidence (2024-2026)
- Fibrosis in endometriosis (Vissers et al., Hum Reprod Update 2024, PMID 39067455): Systematic review highlighting fibrosis as a key driver of disease progression and pain in endometriosis - a potential therapeutic target distinct from the current hormonal approach.
- Exercise as adjunct therapy (Xie et al., PLoS One 2025, PMID 39946383): Meta-analysis showing physical activity is effective and safe for improving pain and quality of life in women with endometriosis.
Summary Table
| Feature | Detail |
|---|---|
| Prevalence | 5-10% of reproductive-age women |
| Pathogenesis | Retrograde menstruation (most likely); also metastasis, metaplasia, stem cells |
| Diagnosis gold standard | Laparoscopy + histology (glands + stroma) |
| Most common symptom | Pain (dysmenorrhoea, deep dyspareunia, chronic pelvic pain) |
| Key examination finding | Fixed retroverted uterus, tender uterosacral ligaments |
| Best imaging for DIE | MRI (bowel/deep disease); TVS (endometriomas) |
| Medical Rx | Progestogens, LNG-IUS, GnRH agonists +/- add-back, aromatase inhibitors |
| Definitive surgery | Hysterectomy + BSO + excision of all disease |
| Malignant risk | Mainly DIE - endometrioid/clear cell ovarian carcinoma |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed.; Robbins & Kumar Basic Pathology; Grainger & Allison's Diagnostic Radiology; Murray & Nadel's Textbook of Respiratory Medicine
Menstrual cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have everything I need for comprehensive notes. Let me compile them.
The Menstrual Cycle - Clinical Notes
Overview
The normal menstrual cycle is a highly coordinated interplay between the hypothalamus, anterior pituitary, ovary, and uterus (endometrium). Its purpose is to produce an optimal environment for pregnancy; if pregnancy does not occur, the cycle resets.
- Average cycle length: 28 days (normal range: 26-34 days)
- Cycle variation is almost entirely due to variation in the follicular phase; the luteal phase is relatively constant (~14 days)
- Day 1 = first day of menstrual bleeding
- Average duration of flow: 4-6 days; average blood loss: ~30 mL
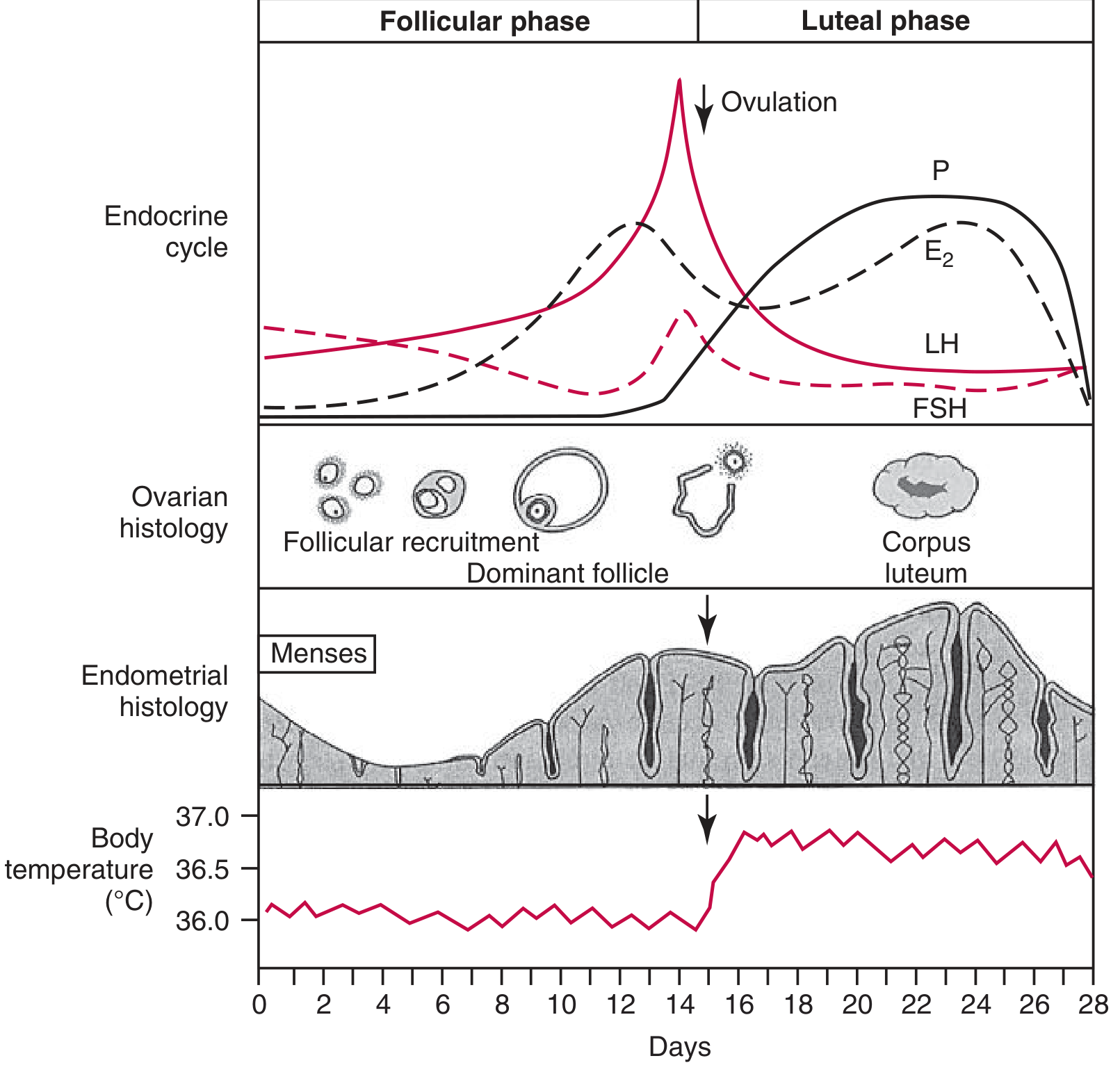
Hormonal, ovarian, endometrial, and basal body temperature changes across the normal menstrual cycle. - Tietz Textbook of Laboratory Medicine, 7th Ed.
The Hypothalamic-Pituitary-Ovarian (HPO) Axis
Hypothalamus
The hypothalamus is a small neural structure at the base of the brain above the optic chiasm, below the third ventricle. It produces pituitary-releasing factors including:
- GnRH (gonadotropin-releasing hormone) - controls LH and FSH
- CRH - controls ACTH
- GHRH - controls GH
- TRH - controls TSH
The anterior pituitary has no direct arterial blood supply - it receives hypothalamic factors exclusively via the portal vessels descending from the median eminence. This location is outside the blood-brain barrier, enabling bidirectional feedback.
Gonadotropin-Releasing Hormone (GnRH)
- A decapeptide produced by neurons in the arcuate nucleus of the hypothalamus
- GnRH neurons originate embryologically in the olfactory pit and migrate to the hypothalamus
- Secreted in a pulsatile fashion into the portal circulation
- Pulse frequency governs the LH:FSH ratio: high frequency favours LH, low frequency favours FSH
- GnRH has a self-priming effect: each dose potentiates the response to subsequent doses
- Continuous (non-pulsatile) GnRH administration causes pituitary desensitisation and gonadotropin suppression - the basis of GnRH agonist therapy
Feedback Loops
| Loop | Mechanism |
|---|---|
| Long loop | Circulating ovarian hormones (E2, androgens) feed back on hypothalamic steroid receptors |
| Short loop | Pituitary hormones feed back to the hypothalamus |
| Ultrashort loop | Hypothalamic secretions feed back on the hypothalamus itself |
Two hypothalamic feedback centres:
- Tonic negative feedback centre (basal medial hypothalamus) - responds to low/baseline E2 and to progesterone+E2 in the luteal phase
- Cyclic positive feedback centre (anterior hypothalamus) - activated by the high pre-ovulatory E2 surge -> triggers the LH surge
The Phases of the Menstrual Cycle
Phase 1: Follicular Phase (Days 1-14) = Proliferative Phase
Dominant hormone: Oestrogen (17β-Estradiol)
Trigger: In the last few days of the previous luteal phase, falling E2/progesterone/inhibin A from the regressing corpus luteum removes negative feedback, allowing FSH to rise.
Sequence of events:
- Days 1-5 (early follicular): Rising FSH recruits a cohort of antral follicles. LH begins to rise around mid-follicular phase.
- Days 5-7: A single dominant follicle is selected - the one with the most FSH receptors and richest estrogenic microenvironment. All others undergo atresia.
- Progressive E2 rise: The dominant follicle produces increasing E2, which:
- Causes negative feedback → FSH falls
- Stimulates endometrial proliferation
- Causes cervical mucus to become copious, watery, and elastic ("ferning" pattern)
- Pre-ovulatory (Day ~13): E2 reaches a critical threshold (peak ~250-400 pg/mL) → switches from negative to positive feedback on the hypothalamus → LH surge triggered
Two-Cell, Two-Gonadotropin Theory (Follicular Steroidogenesis)
This is the fundamental mechanism of follicular oestrogen production:
| Cell type | Gonadotropin | Product |
|---|---|---|
| Theca cells | LH | Androgens (androstenedione) |
| Granulosa cells | FSH | Aromatise androgens → Oestrogens |
- Granulosa cells lack early enzymes in the steroidogenic pathway and need androgen substrate from theca cells
- Theca cells lack aromatase and need granulosa cells to complete oestrogen synthesis
- FSH + local E2 further stimulate FSH receptor expression and granulosa cell proliferation
- Increasing ovarian inhibin B also suppresses FSH to create a competitive environment
Clinical note: Androgen excess (e.g., PCOS) suppresses FSH → blocks dominant follicle emergence → chronic anovulation
Ovulation (Day ~14)
Trigger: The LH Surge
- Preovulatory E2 peak activates the cyclic positive feedback centre → increased GnRH pulse frequency + increased pituitary sensitivity to GnRH → LH surge
- LH surge onset occurs 16-58 hours before ovulation in 90% of women; LH peak occurs 3-36 hours before ovulation
- A smaller FSH surge also occurs at midcycle (triggered by progesterone), thought to stimulate plasminogen activator and increase granulosa cell LH receptors
- LH surge triggers:
- Completion of meiosis I in the oocyte (previously arrested at prophase I)
- Prostaglandin release and proteolytic enzyme activation → follicular wall rupture
- Ovulation of the secondary oocyte + first polar body
- Androgens also peak at midcycle
Phase 2: Luteal Phase (Days 14-28) = Secretory Phase
Dominant hormone: Progesterone (also oestrogen, but progesterone predominates)
Formation of the corpus luteum:
- The ruptured follicle is transformed into the corpus luteum (luteinisation)
- Granulosa and theca cells hypertrophy and accumulate lipid-containing yellow pigment (lutein)
- Progesterone production increases 10-20× to peak ~8 days after the LH surge (day ~22)
- E2 also rises again from the corpus luteum
Hormonal effects:
- Progesterone + E2 exert negative feedback on both the hypothalamic tonic centre and pituitary → LH and FSH are suppressed
- A low level of LH is still needed to sustain corpus luteum function
If no fertilisation (no hCG):
- Corpus luteum regresses (~day 24-26)
- E2 and progesterone fall
- Endometrium is shed (menstruation)
- Falling E2 → removes negative feedback → FSH begins to rise → next cycle begins
If fertilisation occurs:
- Trophoblast produces hCG (structurally homologous to LH, binds LH receptors)
- hCG rescues the corpus luteum → progesterone continues to rise
- Sustained progesterone maintains the endometrium for implantation
Endometrial Changes
| Phase | Endometrial Changes | Driving Hormone |
|---|---|---|
| Menstruation (Days 1-4) | Shedding of functional layer; spiral artery vasospasm | Fall in E2 + P |
| Proliferative (Days 5-14) | Endometrial growth; gland and stroma proliferation; elongation of spiral arteries | Oestrogen (E2) |
| Secretory (Days 15-28) | Proliferation slows; glands become tortuous, accumulate glycogen vacuoles; stroma becomes oedematous; spiral arteries elongate and coil; increased mucus secretions | Progesterone |
Endometrial Layers
- Stratum functionale - shed at menstruation; regenerates each cycle
- Stratum basale - permanent layer; source of regeneration
Cervical Mucus Changes
| Phase | Mucus character | "Ferning" |
|---|---|---|
| Follicular (high E2) | Copious, watery, elastic, thin | Yes - channels form allowing sperm penetration |
| Luteal (high P) | Scant, thick, non-elastic | No - impenetrable to sperm |
Basal Body Temperature (BBT)
- Progesterone has a mild thermogenic effect
- BBT rises ~0.3-0.5°C after ovulation and remains elevated throughout the luteal phase
- The transient dip just before the rise corresponds to the E2 peak at ovulation
- BBT charts can retrospectively confirm ovulation
Hormone Summary Across the Cycle
| Hormone | Early Follicular | Pre-Ovulatory | Luteal | At Menstruation |
|---|---|---|---|---|
| FSH | Rising | Falls after LH surge (small midcycle peak) | Low (suppressed) | Rises again (next cycle trigger) |
| LH | Low, rising | Surge (day ~13-14) | Low (suppressed) | Low |
| E2 | Rising | Peak (~250-400 pg/mL) | Moderate (second rise) | Falls |
| Progesterone | Very low | Begins to rise post-LH surge | Peak (~day 21-22) | Falls |
| Inhibin B | Rises with follicle | - | - | - |
| Inhibin A | Low | - | Peaks in mid-luteal | Falls |
Key Reference Values
| Hormone | Follicular phase | Midcycle peak | Luteal phase |
|---|---|---|---|
| E2 | < 50 pg/mL early; rising to 250-400 pg/mL | 250-400 pg/mL | Moderate |
| Progesterone | < 1 ng/mL | Begins to rise | Peak ~10-20 ng/mL (~day 21) |
| FSH | 3-10 IU/L | Small surge | Low |
| LH | 2-15 IU/L | Surge: 22-105 IU/L | Low |
A mid-luteal progesterone > 3 ng/mL (or ideally >5-10 ng/mL) confirms ovulation
Inhibins and Other Modulators
- Inhibin B - produced by granulosa cells of small/medium follicles; suppresses FSH in follicular phase
- Inhibin A - produced mainly by the dominant follicle and corpus luteum; suppresses FSH in mid-late luteal phase
- Activin - stimulates FSH secretion (opposing inhibin)
- IGF-1 - amplifies FSH and LH actions in the follicle
Clinical Correlates
| Condition | Mechanism |
|---|---|
| Anovulation | Disrupted LH surge; FSH insufficiency; androgen excess (PCOS) |
| PCOS | Androgen excess → FSH suppression → no dominant follicle → chronic anovulation |
| Luteal phase defect | Insufficient progesterone from corpus luteum → poor endometrial preparation |
| Hypothalamic amenorrhoea | Loss of pulsatile GnRH (low weight, stress, exercise) → low LH/FSH |
| GnRH agonist therapy | Continuous GnRH → pituitary desensitisation → medically-induced hypogonadism |
| Ovulation induction | Exogenous FSH/LH or clomiphene (blocks E2 negative feedback → increases FSH) |
| Menopause | Ovarian follicle depletion → no E2/inhibin → very high FSH and LH |
Sources: Berek & Novak's Gynecology; Tietz Textbook of Laboratory Medicine, 7th Ed.; Costanzo Physiology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.