All cranial nerves
Reading File
Finding Sources
Searching the Web
cranial nerves overview anatomy function mnemonic
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have excellent, comprehensive data from Gray's Anatomy for Students. Let me compile the full answer.
Here is a complete overview of all 12 cranial nerves, sourced from Gray's Anatomy for Students.
The 12 Cranial Nerves
There are 12 pairs of cranial nerves (CN I-XII), all part of the peripheral nervous system. They exit the cranial cavity through foramina or fissures in the skull. All except CN XI (accessory nerve) originate from the brain. They innervate structures in the head and neck; the vagus nerve (X) additionally descends into the thorax and abdomen.
Mnemonic for names: Oh, Oh, Oh, To Touch And Feel Very Good, Very Appreciated Heaven
Mnemonic for type (S = Sensory, M = Motor, B = Both): Some Say Marry Money But My Brother Says Bad Business Marry Money
Types of Fibers (Functional Components)
| Abbreviation | Type | Function | Cranial Nerves |
|---|---|---|---|
| GSA | General Somatic Afferent | Touch, pain, temperature | V, VII, IX, X |
| GVA | General Visceral Afferent | Sensory from viscera | IX, X |
| SA | Special Afferent | Smell, taste, vision, hearing, balance | I, II, VII, VIII, IX, X |
| GSE | General Somatic Efferent | Motor to voluntary skeletal muscles | III, IV, VI, XII |
| GVE | General Visceral Efferent | Motor to smooth muscle, heart, glands (parasympathetic) | III, VII, IX, X |
| BE | Branchial Efferent | Motor to pharyngeal arch-derived muscles | V, VII, IX, X, XI |
(Gray's Anatomy for Students, p. 1033)
CN I - Olfactory Nerve
- Type: Sensory (SA)
- Exit: Cribriform plate of ethmoid bone
- Function: Smell (olfaction)
- Notes: Axons of olfactory receptor cells in the nasal mucosa; not a true nerve but a brain tract extension
CN II - Optic Nerve
- Type: Sensory (SA)
- Exit: Optic canal
- Function: Vision
- Notes: Also technically an extension of the brain (surrounded by meninges); damage causes visual field defects
CN III - Oculomotor Nerve
- Type: Motor (GSE + GVE)
- Exit: Superior orbital fissure
- Function:
- GSE: Innervates superior rectus, inferior rectus, medial rectus, inferior oblique, and levator palpebrae superioris muscles
- GVE (parasympathetic): Innervates sphincter pupillae (pupil constriction) and ciliary muscle (accommodation) via ciliary ganglion
- Lesion: Ptosis, "down and out" eye, dilated pupil (CN III palsy)
CN IV - Trochlear Nerve
- Type: Motor (GSE)
- Exit: Superior orbital fissure
- Function: Innervates the superior oblique muscle (depresses and intorts the adducted eye)
- Notes: Only cranial nerve to exit from the dorsal aspect of the brainstem; smallest cranial nerve
CN V - Trigeminal Nerve
- Type: Mixed (GSA + BE)
- Exit: Three divisions:
- V1 (Ophthalmic) - Superior orbital fissure
- V2 (Maxillary) - Foramen rotundum
- V3 (Mandibular) - Foramen ovale
- Function:
- GSA: Sensation from face, scalp, cornea, nasal/oral mucosa, teeth, sinuses, dura mater
- BE: Muscles of mastication (masseter, temporalis, pterygoids), tensor tympani, tensor veli palatini, mylohyoid, anterior belly of digastric
- Notes: Carries parasympathetic fibers from CN III, VII, IX to target glands (hitchhiking)
CN VI - Abducens Nerve
- Type: Motor (GSE)
- Exit: Superior orbital fissure
- Function: Innervates the lateral rectus muscle (abduction of the eye)
- Lesion: Horizontal diplopia; eye deviated medially at rest
CN VII - Facial Nerve
- Type: Mixed (GSA + SA + GVE + BE)
- Exit: Stylomastoid foramen (enters via internal acoustic meatus, gives branches in facial canal first)
- Function:
- GSA: Sensation from part of external acoustic meatus and auricle
- SA: Taste from anterior 2/3 of tongue (via chorda tympani)
- GVE (parasympathetic): Lacrimal gland, submandibular and sublingual glands, mucous membranes of nasal cavity and palate (via pterygopalatine and submandibular ganglia)
- BE: Muscles of facial expression, scalp, stapedius, stylohyoid, posterior belly of digastric
- Lesion: UMN (contralateral lower face weakness) vs. LMN (Bell's palsy - entire ipsilateral face)
CN VIII - Vestibulocochlear Nerve
- Type: Sensory (SA)
- Exit: Internal acoustic meatus (does not exit the skull proper)
- Function:
- Vestibular division: Balance and equilibrium (semicircular canals, utricle, saccule)
- Cochlear division: Hearing (organ of Corti)
- Lesion: Sensorineural hearing loss, vertigo, tinnitus
CN IX - Glossopharyngeal Nerve
- Type: Mixed (GVA + SA + GSA + GVE + BE)
- Exit: Jugular foramen
- Function:
- GVA: Sensory from carotid body/sinus, posterior 1/3 of tongue, palatine tonsils, oropharynx, mucosa of middle ear, mastoid air cells
- SA: Taste from posterior 1/3 of tongue
- GVE (parasympathetic): Parotid salivary gland via otic ganglion
- BE: Stylopharyngeus muscle (only muscle directly innervated)
- Mediates the gag reflex (afferent limb)
CN X - Vagus Nerve
- Type: Mixed (GSA + GVA + SA + GVE + BE)
- Exit: Jugular foramen
- Function:
- GSA: Larynx, laryngopharynx, auricle, external acoustic meatus, posterior cranial fossa dura
- GVA: Aortic arch chemoreceptors and baroreceptors, esophagus, bronchi, lungs, heart, foregut and midgut viscera
- SA: Taste from epiglottis and pharynx
- GVE (parasympathetic): Smooth muscle and glands of pharynx, larynx, thoracic and abdominal viscera (foregut/midgut)
- BE: Palatoglossus, muscles of soft palate (except tensor veli palatini), pharynx (except stylopharyngeus), and larynx
- Notes: The most widely distributed cranial nerve; critical for cardiac, respiratory, and GI function
CN XI - Accessory Nerve
- Type: Motor (BE)
- Exit: Jugular foramen
- Function: Innervates sternocleidomastoid (SCM) and trapezius muscles
- Notes: Unique - its spinal roots arise from C1-C5 anterior horn cells; enters cranial cavity through foramen magnum before exiting via jugular foramen
- Lesion: Weakness turning head (SCM) and shoulder shrug (trapezius)
CN XII - Hypoglossal Nerve
- Type: Motor (GSE)
- Exit: Hypoglossal canal
- Function: Innervates hyoglossus, genioglossus, styloglossus, and all intrinsic tongue muscles
- Lesion: Tongue deviates toward the side of the lesion (ipsilateral) on protrusion
Parasympathetic Cranial Nerves (GVE) - Summary
Four cranial nerves carry parasympathetic fibers. Fibers from III, VII, and IX relay in named ganglia before being distributed via CN V branches to target organs:
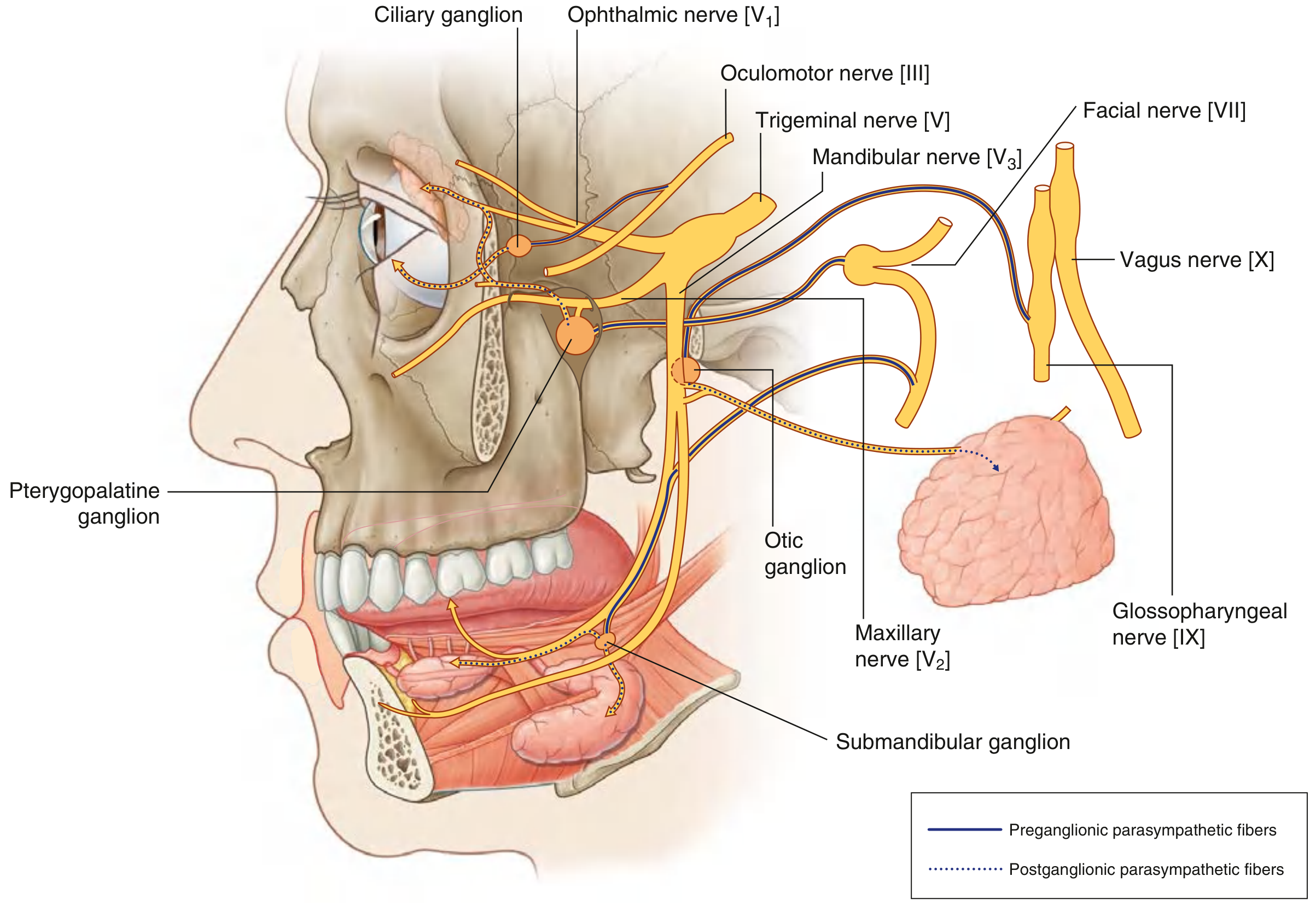
| CN | Ganglion | Target |
|---|---|---|
| III | Ciliary ganglion | Pupillary sphincter, ciliary muscle |
| VII | Pterygopalatine ganglion | Lacrimal gland, nasal/palatine glands |
| VII | Submandibular ganglion | Submandibular and sublingual glands |
| IX | Otic ganglion | Parotid gland |
| X | Terminal ganglia (in/near organs) | Thoracic and abdominal viscera |
(Gray's Anatomy for Students, p. 987)
Quick Reference Table
| # | Name | Type | Exit | Key Function |
|---|---|---|---|---|
| I | Olfactory | Sensory | Cribriform plate | Smell |
| II | Optic | Sensory | Optic canal | Vision |
| III | Oculomotor | Motor | Superior orbital fissure | Eye movement (SR, IR, MR, IO, LPS), pupil constriction |
| IV | Trochlear | Motor | Superior orbital fissure | Superior oblique (depression + intorsion) |
| V | Trigeminal | Both | SOF / F. rotundum / F. ovale | Face sensation; muscles of mastication |
| VI | Abducens | Motor | Superior orbital fissure | Lateral rectus (abduction) |
| VII | Facial | Both | Stylomastoid foramen | Facial expression; taste ant. 2/3 tongue; lacrimal/salivary glands |
| VIII | Vestibulocochlear | Sensory | Internal acoustic meatus | Hearing + balance |
| IX | Glossopharyngeal | Both | Jugular foramen | Taste/sensation post. 1/3 tongue; parotid gland; gag reflex (afferent) |
| X | Vagus | Both | Jugular foramen | Parasympathetics to thorax/abdomen; phonation; gag reflex (efferent) |
| XI | Accessory | Motor | Jugular foramen | SCM + trapezius |
| XII | Hypoglossal | Motor | Hypoglossal canal | Tongue movements |
How loopdiuretics are ototoxic
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
loop diuretics ototoxicity mechanism stria vascularis endocochlear potential NKCC1
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC6002634
Reading File
Reading File
Excellent - I now have a complete picture from multiple authoritative sources. Here is the full answer:
Loop Diuretics and Ototoxicity
The Target: Stria Vascularis
The cochlea maintains a unique ionic environment essential for hearing. The stria vascularis - a highly vascularized epithelium lining the lateral wall of the cochlear duct - is responsible for:
- Secreting endolymph (high K⁺, low Na⁺ fluid) into the scala media
- Generating the endocochlear potential (EP) - a standing +80 to +90 mV DC potential that powers mechanotransduction in outer hair cells
This +90 mV EP is the "battery" of the cochlea. When it collapses, hair cell transduction fails and hearing is lost.
Step-by-Step Mechanism
Step 1 - NKCC Inhibition in the Stria Vascularis
Loop diuretics (furosemide, ethacrynic acid, bumetanide) block the Na⁺-K⁺-2Cl⁻ cotransporter (NKCC1/NKCC2) in the marginal and dark cells of the stria vascularis - the same pump they block in the thick ascending limb of the loop of Henle in the kidney.
This cotransporter is critical for:
- Pumping K⁺ into the stria vascularis cells
- Maintaining the high endolymphatic K⁺ concentration
- Sustaining the electrochemical gradient that generates the EP
(National Kidney Foundation Primer on Kidney Diseases, p. 119)
Step 2 - Secondary Enzyme Disruption
The drugs also interfere with:
- Na⁺/K⁺-ATPase (reduced activity)
- Adenylate cyclase (impaired cAMP signaling)
- Mg²⁺-ATPase and succinate dehydrogenase (mitochondrial respiration impaired)
These effects may be secondary consequences of the primary ischemic/ionic insult rather than direct drug actions. (PMC6002634)
Step 3 - Vascular Ischemia (most recent evidence)
The current leading hypothesis is that the earliest in vivo effect of loop diuretics is actually vasoconstriction of strial blood vessels, not direct transporter inhibition:
- Loop diuretics activate the renin-angiotensin system in pericytes of strial arterioles
- This causes vasoconstriction of lateral wall vessels
- The resulting cochlear ischemia and anoxia causes the stria to become edematous (edematous spaces form within the strial epithelium)
- The secondary consequence is inhibition of Na⁺/K⁺-ATPase and NKCC due to anoxia
This explains why ethacrynic acid does not damage stria in vitro (no blood vessels) but is highly toxic in vivo. (Ototoxic effects and mechanisms of loop diuretics, PMC6002634)
Step 4 - Endocochlear Potential Collapse
Regardless of the initiating mechanism, the net result is:
- Loss of K⁺ secretion into endolymph
- Collapse of the endocochlear potential (from +90 mV toward 0 or negative values)
- Loss of the driving force for K⁺ entry into hair cells through mechanosensitive channels
- Failure of cochlear microphonic potential, summating potential, and compound action potential
- Clinical result: sensorineural hearing loss (SNHL), typically bilateral and symmetric
(Cummings Otolaryngology, p. Loop Diuretics section)
Why It's Usually Reversible
As long as the hair cells remain intact (which they do in isolated loop diuretic toxicity), the EP recovers once the drug is cleared. Cochlear microphonic potential amplitude recovers in parallel with EP restoration. This is why the SNHL from furosemide alone is usually transient and reversible.
Permanent deafness occurs only when:
- Hair cells are co-damaged (e.g., by aminoglycosides or cisplatin)
- Severe, sustained ischemia destroys the stria irreversibly
Risk Factors for Ototoxicity
| Risk Factor | Mechanism |
|---|---|
| Rapid IV bolus | High peak plasma levels → rapid strial ischemia |
| Renal failure | Reduced drug clearance → prolonged high plasma levels |
| Hypoalbuminemia | More free drug available (loop diuretics are protein-bound) |
| Concomitant aminoglycosides | Synergistic cochlear damage (tight junction disruption increases aminoglycoside uptake) |
| Concomitant cisplatin | Similar synergy; permanent hair cell loss |
| Ethacrynic acid | Greatest ototoxic risk among all loop diuretics |
(Brenner & Rector's The Kidney; Cummings Otolaryngology)
Ethacrynic Acid - Why the Worst?
Ethacrynic acid is structurally distinct from furosemide and bumetanide (no sulfonamide group). It has a greater ototoxic potential than other loop diuretics and is reserved only for patients allergic to sulfonamide-based agents. The exact reason for its greater toxicity is not fully explained but likely relates to more intense or prolonged strial ischemia, or additional direct cellular toxicity.
(Comprehensive Clinical Nephrology, 7th ed.)
Dose-Rate Dependency - Clinical Lesson
A classic clinical finding illustrates the mechanism beautifully:
In patients with severe heart failure given the same total dose (350-2000 mg) of furosemide:
- Slow infusion over 8 hours → no ototoxicity
- Same dose as IV bolus → reversible deafness in 25%
(Brenner & Rector's The Kidney, p. OTOTOXICITY section)
The guideline is therefore: furosemide IV infusions should be given at <4 mg/min to prevent peak plasma concentrations from reaching the toxic threshold (~50 mg/mL).
Summary Diagram
Loop diuretic → Strial pericyte renin-angiotensin activation
↓
Vasoconstriction of strial arterioles
↓
Strial ischemia + anoxia
↓
Inhibition of NKCC1 + Na/K-ATPase in marginal/dark cells
↓
↓ K⁺ secretion into endolymph
↓
↓ Endocochlear potential (+90 mV → ~0 mV)
↓
Failure of hair cell mechanotransduction
↓
Sensorineural hearing loss (usually reversible)
This is a shared conversation. Sign in to Orris to start your own chat.