Endometriosis
Reading File
Finding Sources
Searching PubMed
"endometriosis"[MeSH Terms] AND "diagnosis OR treatment"
Reading File
Reading File
Reading File
Searching PubMed
"endometriosis"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content. Let me compile the full, detailed answer.
Endometriosis
Definition
Endometriosis is defined by the presence of endometrial glands and stroma in locations outside the uterus. It occurs in approximately 5-10% of women of reproductive age, and in nearly half of women with infertility. It is frequently multifocal.
- Robbins & Kumar Basic Pathology, p. 689
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 1602
Types
There are three main types:
| Type | Description |
|---|---|
| Superficial peritoneal endometriosis | Lesions on pelvic peritoneal surfaces |
| Ovarian endometriosis (endometrioma) | Cysts filled with old blood ("chocolate cysts") |
| Deep infiltrating endometriosis (DIE) | Tissue >5 mm beneath the peritoneum; involves uterosacral ligaments, vagina, bowel, bladder, ureters |
Risk of malignant transformation is mainly confined to deep infiltrating endometriosis (ovarian endometrioid and clear-cell carcinomas). There is also an association with non-Hodgkin's lymphoma.
Pathogenesis
The exact mechanism remains uncertain. Four leading theories are proposed:
-
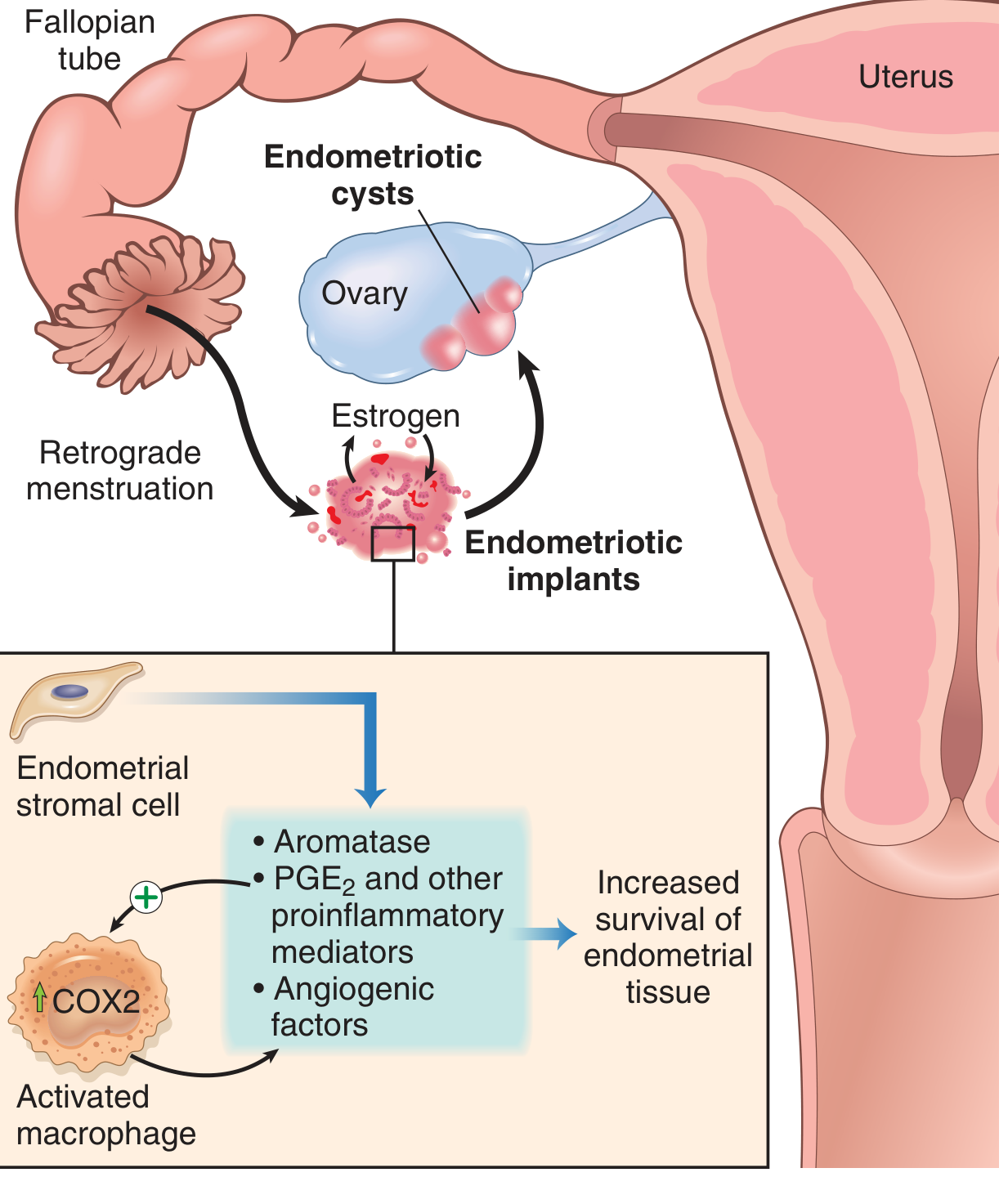
Regurgitation (Sampson) theory - retrograde flow of menstrual endometrium through the fallopian tubes implants at ectopic pelvic sites. This is the most widely accepted mechanism.
-
Benign metastasis theory - endometrial tissue spreads to distant sites (bone, lung, brain) via blood vessels and lymphatics.
-
Metaplastic theory - coelomic epithelium (pelvic mesothelium), which shares embryological origin with the müllerian ducts, undergoes metaplastic differentiation into endometrium. This explains thoracic and other distant sites.
-
Extrauterine stem/progenitor cell theory - bone marrow-derived stem cells differentiate into ectopic endometrial tissue.
Once implanted, endometriotic tissue is not simply "misplaced endometrium" - it exhibits distinct biology: elevated aromatase (local estrogen synthesis), increased PGE2, VEGF, and matrix metalloproteinases (MMPs), some secreted by recruited activated macrophages. This creates a self-sustaining pro-inflammatory, pro-angiogenic, estrogen-dependent microenvironment.
Common Sites
- Ovaries (most common)
- Pouch of Douglas
- Uterosacral ligaments
- Fallopian tubes
- Pelvic peritoneum
- Rectosigmoid colon (12-37% of cases have GI involvement)
- Less commonly: periumbilical tissues, laparotomy scars, diaphragm, pleura, lungs (causing catamenial haemoptysis or recurrent pneumothoraces)
Morphology
Lesions appear grossly as red-brown nodules ranging from microscopic to 1-2 cm. Classic descriptions include:
- "Powder burn" or "gunshot" lesions - black, dark brown, or bluish puckered nodules with surrounding fibrosis
- Red/flame-like lesions - atypical vesicular or haemorrhagic implants
- White plaques - scarring lesions
- Endometriomas ("chocolate cysts") - ovarian cysts 3-5 cm filled with thick dark brown fluid (degenerated blood); found in 17-44% of women with endometriosis; densely adherent to the peritoneal ovarian fossa
Widespread lesions cause fibrous adhesions that obliterate the pouch of Douglas and distort pelvic anatomy.
Histologically: diagnosis requires both endometrial glands AND stroma at the ectopic site.

Clinical Features
Symptoms
- Dysmenorrhoea (pain related to menstruation) - most common pain symptom
- Chronic pelvic pain (cyclical and non-cyclical)
- Deep dyspareunia (pain during intercourse)
- Dyschezia (pain on opening the bowels)
- Dysuria
- Infertility - presenting complaint in 30-40% of patients
- Haematuria, rectal bleeding (haematochezia)
- Fatigue
- Recurrent haemoptysis / pneumothorax (thoracic endometriosis)
A significant proportion of women remain asymptomatic. No single symptom or set of symptoms reliably predicts endometriosis, as many overlap with IBS or interstitial cystitis.
Disease Extent
Ranges from a few peritoneal lesions on normal-looking pelvic organs all the way to deep endometriosis with large endometriomas, extensive fibrosis of uterosacral ligaments, and adhesion-related distortion of pelvic anatomy.
Diagnosis
Gold standard: laparoscopy with histological confirmation
- Non-invasive tools (transvaginal/transrectal ultrasound) can reliably detect only severe forms - endometriomas and deep pelvic endometriosis
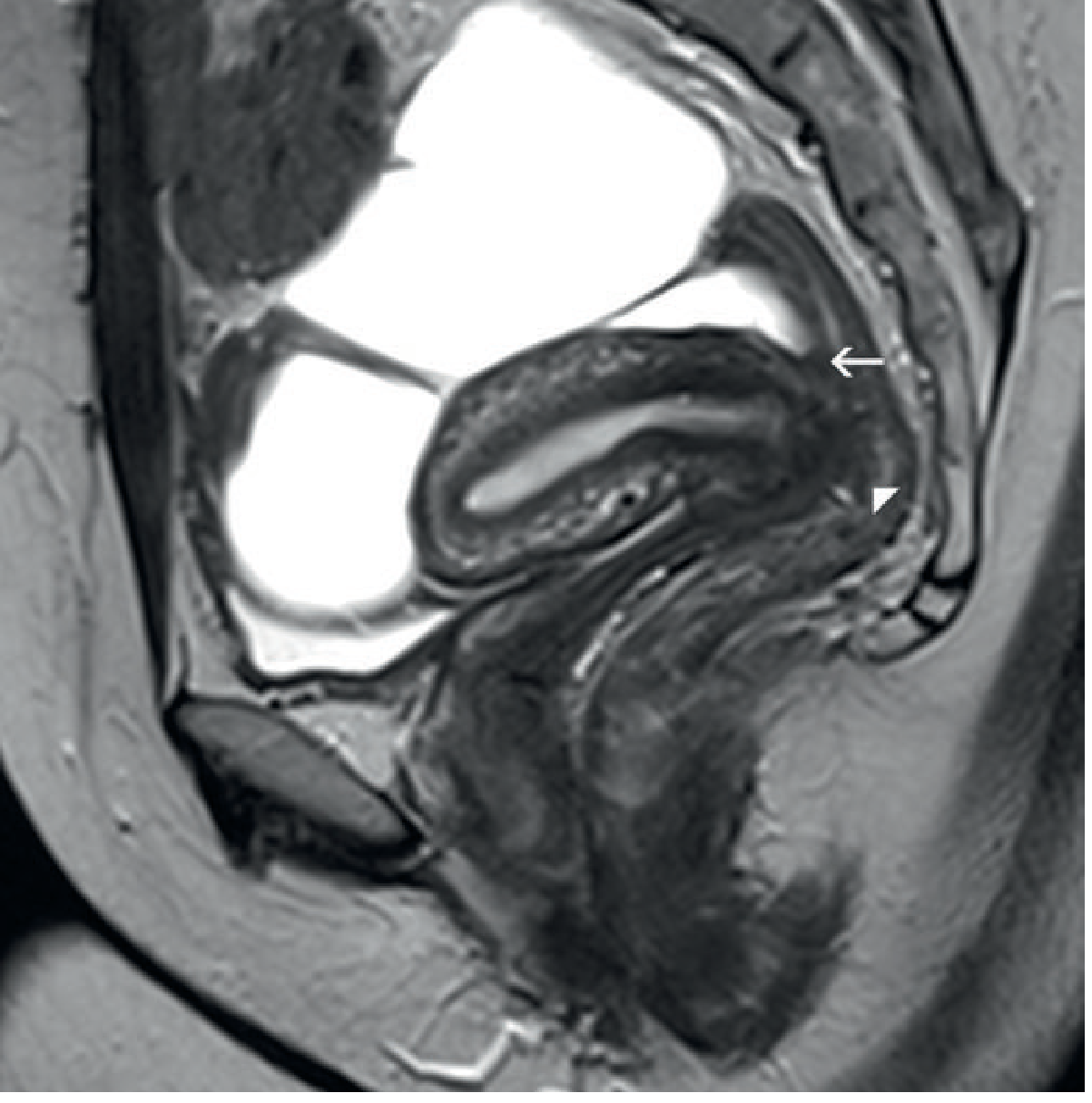
- MRI detects haemosiderin deposits and can demonstrate low-signal fibrotic plaques, obliteration of the pouch of Douglas, and involvement of the rectosigmoid
There is currently no internationally accepted classification system. The Endometriosis Fertility Index (EFI) has good predictive value for fecundity after surgical treatment. Note that disease severity on classification systems correlates poorly with symptom severity.
Management
Medical
| Category | Agents |
|---|---|
| NSAIDs / COX-2 inhibitors | First-line for pain |
| Aromatase inhibitors | Target local estrogen production |
| Combined oral contraceptives | Suppress ovarian cycle |
| Progestogens | Suppress endometrial activity |
| GnRH agonists/antagonists | Induce pseudo-menopause |
| Levonorgestrel-releasing IUS | Effective for pain and bleeding |
Surgical
- Laparoscopic excision or ablation of lesions - preferred approach
- Drainage/cystectomy for endometriomas
- For DIE: may require bowel resection, ureteric dissection, or partial cystectomy
- Hysterectomy (with/without bilateral salpingo-oophorectomy) - definitive treatment for women who have completed childbearing
- Surgery for infertility aims to restore normal anatomy
Fertility-Specific
- The EFI guides prognosis after surgery
- Assisted reproductive technology (IVF) is an option when surgery does not restore fertility
Complications & Associations
- Infertility (30-40% of cases)
- Increased risk of ovarian cancer (endometrioid and clear-cell subtypes)
- Non-Hodgkin's lymphoma association
- Bowel obstruction, ureteric obstruction from DIE
- Recurrent pneumothoraces (catamenial pneumothorax) from thoracic disease
- Fibrous adhesions leading to chronic pelvic pain and anatomical distortion
Recent Evidence (PubMed, 2024-2026)
- A 2024 systematic review (PMID 39067455) highlights the central role of fibrosis in endometriosis pathogenesis and as a potential therapeutic target, beyond the traditional estrogen-focused model.
- A 2025 systematic review and meta-analysis (PMID 39946383) found that physical activity and exercise are safe and beneficial for women with endometriosis, improving pain and quality of life.
- A 2025 systematic review (PMID 39373298) confirms persistent diagnostic delay of 5-12 years across regions, driven by symptom normalisation, misdiagnosis, and limited access to laparoscopy.
Sources: Robbins & Kumar Basic Pathology, p. 689 | Bailey and Love's Short Practice of Surgery 28th Ed., p. 1602-1603 | Grainger & Allison's Diagnostic Radiology, p. 591
This is a shared conversation. Sign in to Orris to start your own chat.