A 23 year old male patient present with the complaint of polypsia and polyuria for 10 days symptom only occurs when he rest or sleep . It costly disturbance in every 1 hour polyuria
Reading File
Finding Sources
Finding Sources
Searching the Web
polyuria polydipsia only during sleep rest positional diabetes insipidus diagnosis
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Excellent. Now I have very rich information. Let me compile the full clinical analysis for this case.
Clinical Analysis: 23-Year-Old Male with Polyuria & Polydipsia - Only During Rest/Sleep
The Key Diagnostic Clue
The defining feature of this case is that polydipsia and polyuria occur exclusively during rest or sleep, with polyuria every 1 hour at night. This points specifically to Nocturnal Polyuria - and the pattern of symptoms restricted entirely to recumbency/sleep is a hallmark of a specific underlying mechanism.
Most Likely Diagnosis: Nocturnal Polyuria
The textbook classification of nocturia causes is essential here:
| Nocturia Category | Underlying Conditions |
|---|---|
| Nocturnal Polyuria | Excessive nighttime fluid intake, Peripheral edema, Obstructive Sleep Apnea, Diabetes mellitus, Congestive heart failure |
| Diminished bladder capacity | Bladder/ureteral calculi, neurogenic bladder, detrusor overactivity, prostatic obstruction |
| Global (24-hour) polyuria | Primary polydipsia, Diabetes insipidus, Diabetes mellitus |
Since this patient's symptoms occur ONLY at rest/sleep, global polyuria (diabetes insipidus, DM) is less likely - those would cause symptoms throughout the day too. The fact that he is completely asymptomatic when awake and active makes nocturnal polyuria the correct category.
- Campbell-Walsh Wein Urology, p. 3504
Top Differential Diagnoses in Order of Probability
1. Obstructive Sleep Apnea (OSA) with Nocturnal Polyuria - HIGH PRIORITY
This is the most clinically relevant diagnosis to exclude even in a 23-year-old.
Mechanism: OSA causes hypoxia → pulmonary vasoconstriction → increased right atrial transmural pressure → elevated Atrial Natriuretic Peptide (ANP) → inhibition of ADH/AVP → massive nocturnal water and sodium diuresis. The patient voids every 1 hour precisely because ANP surges with each apnea event.
Ask specifically about: snoring, witnessed apneas, obesity, daytime sleepiness.
- Campbell-Walsh Wein Urology, p. 3504
2. Peripheral Edema / Dependent Fluid Redistribution (Postural)
When a patient lies down, edema fluid from dependent parts (legs) is redistributed into the central circulation → increased venous return → ANP release → natriuresis and water diuresis. Common in:
- Venous insufficiency
- Early heart failure
- Nephrotic syndrome
This is the classic "positional" mechanism: symptoms only when recumbent because that is when fluid redistributes.
3. Primary Polydipsia / Psychogenic Polydipsia with Habitual Nighttime Drinking
Though less likely since there is no daytime component, excessive nighttime fluid intake before bed should be clarified on history.
4. Partial/Nocturnal Central Diabetes Insipidus (Rare)
In very rare cases, partial CDI or a hypothalamic lesion can manifest predominantly or exclusively at night, but this would typically have some daytime symptoms too. A 23-year-old with a 10-day history raises concern for an acquired cause (pituitary tumor, craniopharyngioma, post-traumatic, sarcoidosis, Langerhans cell histiocytosis).
5. Restless Legs Syndrome / Sleep Disorder causing incidental nighttime voiding
The textbook notes that restless legs syndrome is an identified risk factor for nocturia.
Pathophysiology Framework
Normal circadian physiology: In persons under 25, nocturnal urine volume (NUV) is only ~14% of total daily urine. At night, AVP normally rises (circadian peak), reducing urine output. In nocturnal polyuria, this circadian AVP rise is blunted or overridden by ANP.
Key regulators:
-
AVP increased by: high serum osmolality, hypovolemia, angiotensin II
-
AVP inhibited by: natriuretic peptides (ANP, BNP), PGE2, hypercalcemia, hypokalemia, lithium
-
Result of low AVP at night = large volumes of dilute urine during sleep hours
-
Campbell-Walsh Wein Urology, p. 3504
Diagnostic Approach
Step 1: History
- Is he awakened by urge to void, or does he void because he is already awake? (92% are awakened by urge)
- Snoring, witnessed apneas, daytime sleepiness (OSA screen)
- Fluid intake habits - what and how much does he drink before bed?
- Any ankle swelling, dyspnea, cardiac symptoms (edema-redistribution)
- Any recent head trauma, visual changes, headaches (central DI etiology)
- Medications (lithium causes nephrogenic DI)
Step 2: 24-Hour Voiding Diary / Frequency-Volume Chart
This is the most valuable objective instrument - document time, volume, and whether symptoms occur day or night. Calculate:
- Nocturnal Urine Volume (NUV) = all nocturnally voided volumes + first morning void
- Nocturia Index (Ni) = NUV / Maximum Voided Volume (MVV)
- If Ni > 1, nocturnal polyuria is confirmed
Step 3: Initial Labs
- Fasting blood glucose (rule out DM)
- Serum electrolytes, serum osmolality, BUN/creatinine
- Urine osmolality (spot) and specific gravity
Step 4: Based on results:
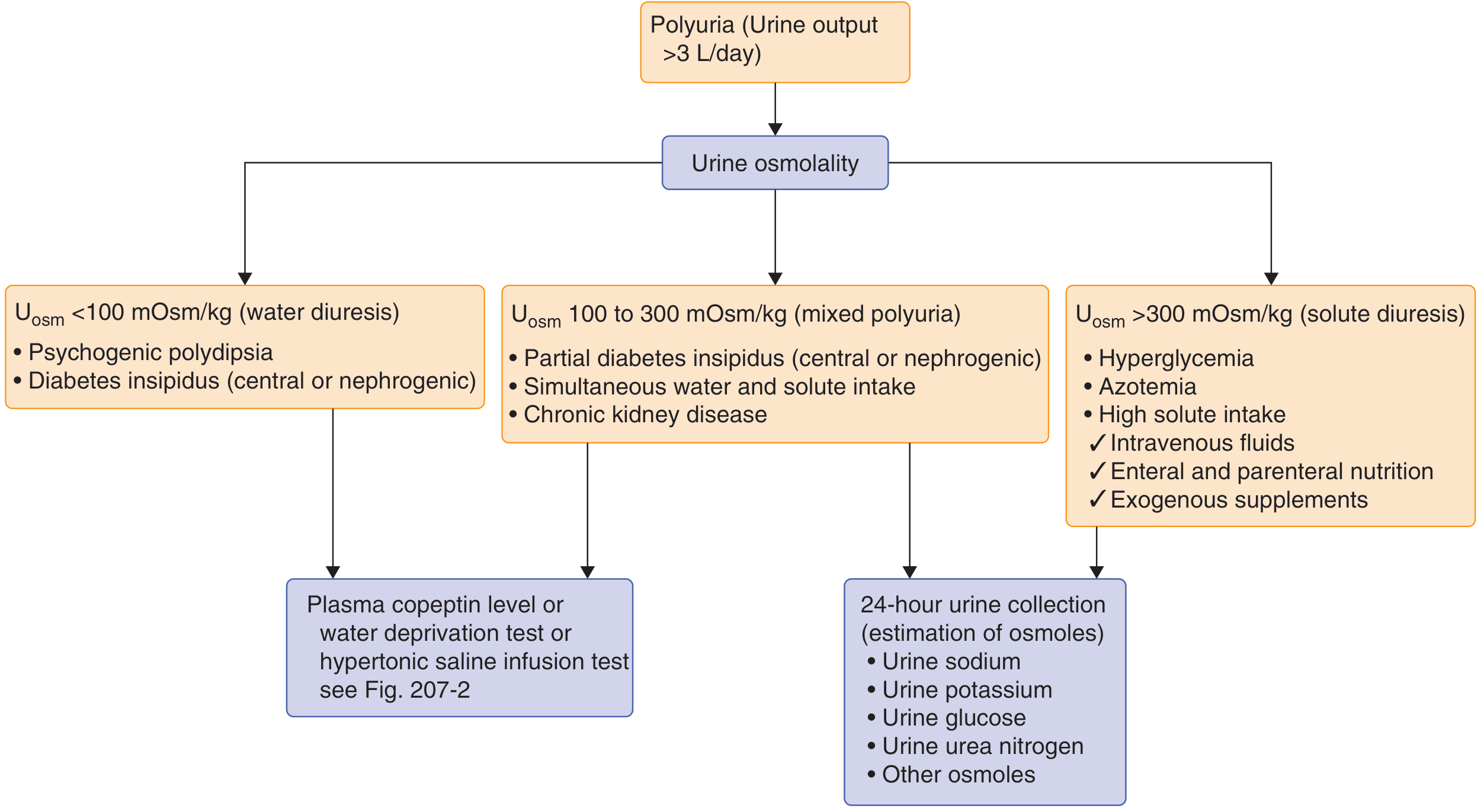
| Urine Osmolality | Direction |
|---|---|
| <100 mOsm/kg (water diuresis) | Water deprivation test / copeptin / hypertonic saline → differentiate DI vs primary polydipsia |
| 100-300 mOsm/kg | Partial DI vs chronic kidney disease |
| >300 mOsm/kg (solute diuresis) | 24-hour urine for glucose, Na, K, urea |
- Goldman-Cecil Medicine, p. 1205
Step 5: Sleep Study (Polysomnography)
If OSA suspected - this is the key test in a young male with nocturia without obvious cause.
Management (Once Diagnosis Confirmed)
| Diagnosis | Treatment |
|---|---|
| OSA | CPAP - resolves nocturnal polyuria completely by eliminating ANP surges |
| Central DI | Desmopressin (DDAVP) - synthetic AVP analogue; intranasal or oral |
| Nephrogenic DI | Thiazide diuretics, low-sodium diet, NSAIDs |
| Edema redistribution | Compression stockings, afternoon diuretic dose, treat underlying cause |
| Excessive evening fluid intake | Behavioral restriction of fluids 2-3 hours before sleep |
| Nocturnal polyuria without OSA/DI | Desmopressin (evening dose) |
Summary for This Patient
Age 23, male, 10-day history, symptoms ONLY at rest/sleep, voiding every 1 hour at night:
The most important diagnoses to pursue are:
- OSA - even in young males, especially if overweight/snorer; most treatable cause
- Dependent edema/venous redistribution - examine legs for pitting edema
- If neither found: evaluate for partial/nocturnal DI with water deprivation test or plasma copeptin
The 10-day duration in a young male also raises concern for an acquired central cause (hypothalamic/pituitary lesion), so if DI is confirmed, MRI brain with pituitary protocol is mandatory to rule out craniopharyngioma, Langerhans cell histiocytosis, germinoma, or other mass lesions.
This is a shared conversation. Sign in to Orris to start your own chat.