Biophysical profile in antenatal monitoring
Reading File
Finding Sources
Finding Sources
Searching PubMed
"biophysical profile" AND "antenatal" AND fetal
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a thorough answer. Let me compile everything.
Biophysical Profile (BPP) in Antenatal Monitoring
The Biophysical Profile (BPP) is an ultrasound-based assessment of fetal well-being, originally designed to parallel the postnatal Apgar score. It relies on the principle that multiple parameters of well-being are better predictors of outcome than any single parameter - Creasy & Resnik's Maternal-Fetal Medicine, p. 719.
Physiological Basis
Fetal behavioral activities (breathing, movement, tone) are controlled by different CNS centers that are progressively inhibited by hypoxemia and acidosis in a predictable sequence:
- Fetal tone - earliest to appear in fetal development (~7-8 weeks), last to disappear with hypoxia (controlled by cortex/subcortex)
- Fetal movements - appear ~9 weeks, second to last lost
- Fetal breathing - appears ~20-21 weeks, second to disappear; most easily suppressed by hypoxemia
- Fetal heart rate (NST) - reflects autonomic nervous system maturity; lost early with acute compromise
- Amniotic fluid volume - a marker of chronic, not acute, compromise; oliguria from renal blood flow redistribution in the setting of uteroplacental insufficiency
This hierarchical suppression means the BPP can distinguish acute from chronic fetal compromise.
The Five Components
Each parameter scores 2 (normal) or 0 (abnormal) - maximum score is 10/10.
| Parameter | Normal (Score = 2) | Abnormal (Score = 0) |
|---|---|---|
| Nonstress Test (NST) | ≥2 accelerations of ≥15 bpm above baseline, lasting ≥15 sec within 20 min | Fewer than 2 adequate accelerations |
| Fetal Breathing Movements | ≥1 episode of rhythmic breathing lasting ≥30 sec within 30 min (some criteria use ≥20 sec) | Absent or <30 sec of breathing |
| Gross Body Movements | ≥3 discrete limb or trunk movements within 30 min | <3 movements |
| Fetal Tone | ≥1 episode of active extension with return to flexion of a limb or spine; opening/closing of the hand counts | Slow extension, no return to flexion, or absent movement |
| Amniotic Fluid Volume | ≥1 pocket of fluid measuring ≥2 cm in vertical axis (the 2×2 cm pocket, confirmed in two perpendicular planes) | No pockets, or largest pocket <2 cm |
- Textbook of Family Medicine 9e, p. 501
- Creasy & Resnik's Maternal-Fetal Medicine, pp. 719-720
The observation window is 30 minutes. A normal score is assigned if criteria are met at any point during that window.
Scoring and Management
| BPP Score | Interpretation | Predicted Perinatal Mortality | Management |
|---|---|---|---|
| 10/10, 8/8, 8/10 (AFV normal) | No evidence of fetal asphyxia | <1:1000 | No acute intervention; serial testing per indication-specific protocol |
| 8/10 with oligohydramnios | Chronic fetal compromise likely (unless PROM proven) | 89:1000 | Gestational-age dependent decision; exclude urinary tract anomaly; exclude undiagnosed PROM; consider steroids if preterm |
| 6/10 (AFV normal) | Equivocal; asphyxia not excluded | ~61:1000 (depends on progression) | Repeat test immediately. If repeat = 10/10 in two continuous 30-min periods, manage as 10/10. Persistent 6/10 at term: deliver. Preterm: repeat within 24 h; deliver if still <6/10 |
| 4/10 | Acute fetal asphyxia likely | ~91:1000 | Deliver (except extreme prematurity - individualize) |
| 2/10 | Severe acute asphyxia | 125:1000 | Deliver promptly |
| 0/10 | Strong suspicion of acute asphyxia | 600:1000 | Deliver promptly |
- Creasy & Resnik's Maternal-Fetal Medicine, p. 720
Amniotic Fluid Assessment - Key Details
The standard BPP technique uses the deepest vertical pocket (DVP):
- Normal: DVP 2-8 cm
- Oligohydramnios: DVP <2 cm
- Polyhydramnios: DVP >8 cm; if >12 cm, chromosomal/structural anomalies are more likely
The transducer is held vertical to the maternal abdomen and rotated 90° to confirm the pocket has true biplanar dimensions (the "2×2 pocket"). Pulsed Doppler is used when there is doubt about a true fluid pocket vs. umbilical cord.
Evidence from a meta-analysis of 4 RCTs (3,125 participants) found that using the AFI vs. DVP for surveillance increased the diagnosis of oligohydramnios (RR 2.33), induction rates (RR 2.1), and cesarean rates without improving neonatal outcomes. This suggests the DVP is superior to AFI for fetal surveillance - Creasy & Resnik's Maternal-Fetal Medicine, p. 720.
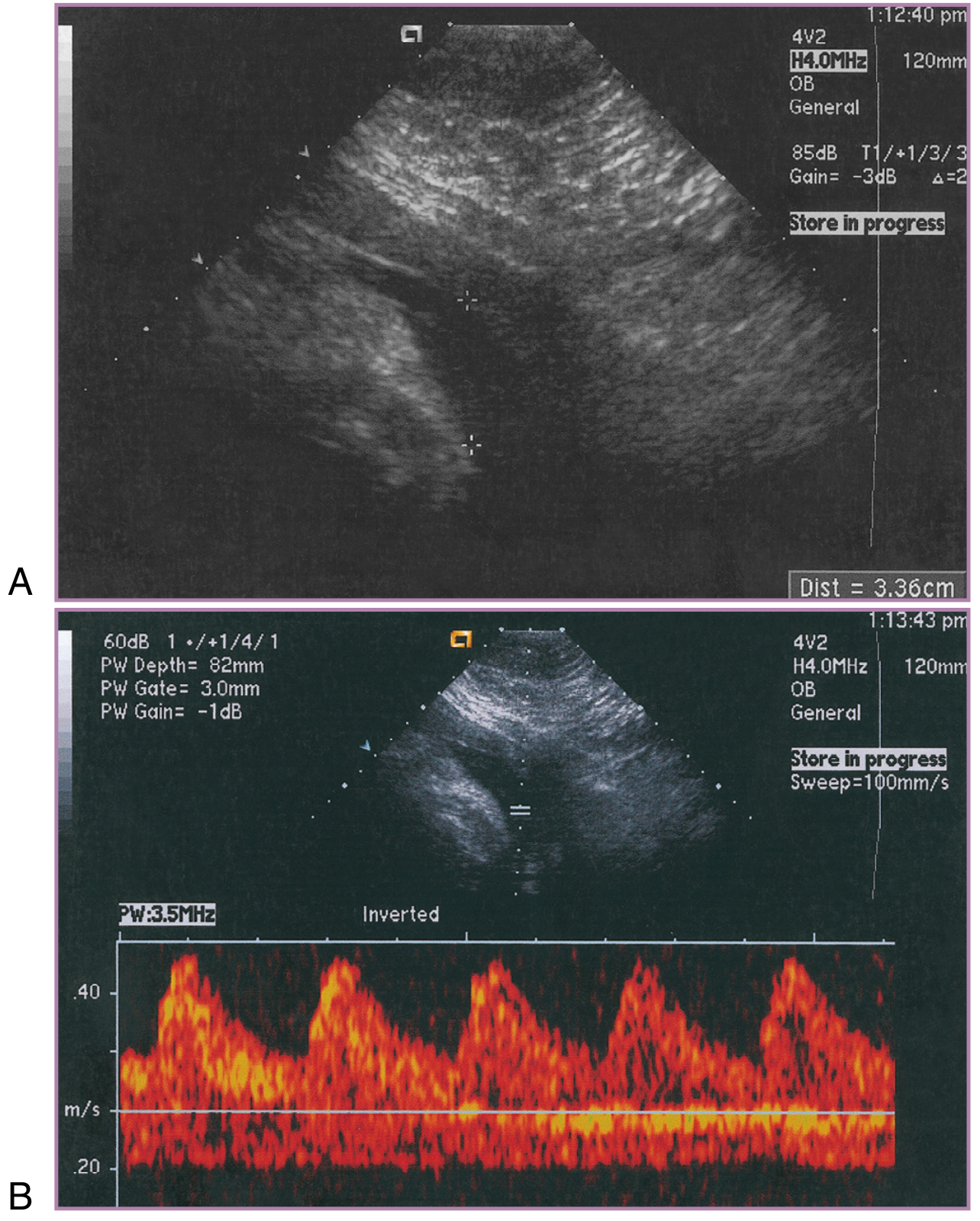
Figure: (A) Amniotic fluid pocket meeting the vertical pocket criteria. (B) Pulsed Doppler confirms this is an umbilical cord loop containing no measurable fluid - illustrating why Doppler verification matters.
Factors That Affect BPP Scoring
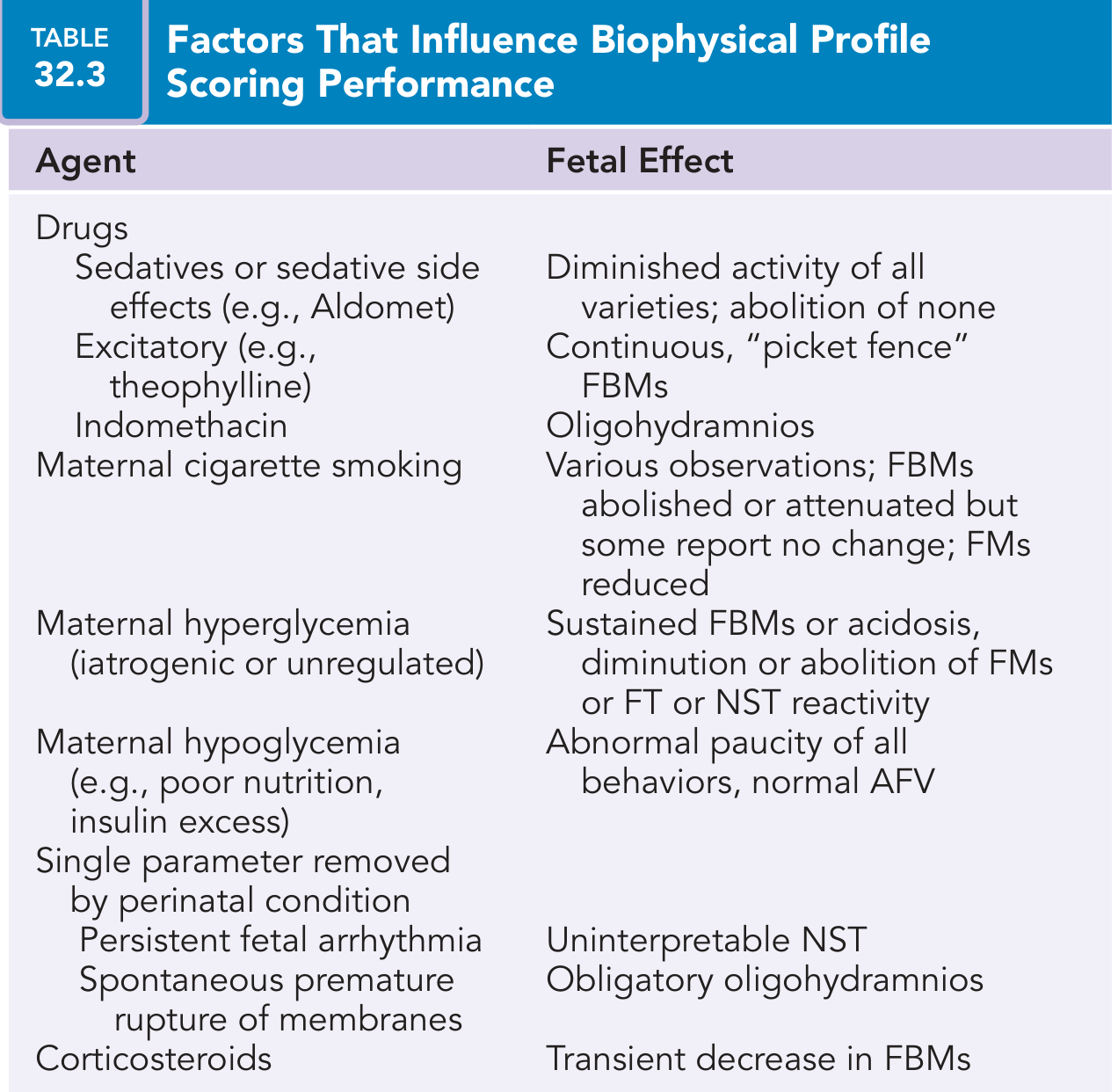
Key confounders:
- Sedatives (e.g., methyldopa): diminish all activity without abolishing any
- Theophylline: causes continuous "picket fence" fetal breathing movements
- Indomethacin: causes oligohydramnios
- Maternal cigarette smoking: reduces FBMs and fetal movements
- Maternal hyperglycemia: can cause sustained FBMs or, with acidosis, abolish FMs
- Maternal hypoglycemia: paucity of all behaviors with normal AFV
- Corticosteroids: transient decrease in FBMs (clinically important after antenatal steroid administration)
- Fetal arrhythmia: makes NST uninterpretable
- PPROM: obligatory oligohydramnios
A low score may also simply reflect a normal fetal sleep cycle or maternal CNS depressants - not fetal compromise.
Modified BPP (mBPP)
The modified BPP uses only two components:
- NST (short-term assessment of fetal acid-base status)
- Amniotic fluid index (AFI) (long-term marker of uteroplacental function)
It has proved to be as effective as the full BPP in assessing fetal well-being, is faster to perform, and identifies patients at increased risk for poor perinatal outcome and SGA infants - Textbook of Family Medicine 9e, p. 501.
Indications for BPP
- Post-dates pregnancy
- Fetal growth restriction (FGR)
- Hypertensive disorders (preeclampsia, chronic hypertension)
- Diabetes mellitus
- Decreased fetal movement (maternal perception)
- Prior stillbirth or adverse perinatal outcome
- Multiple gestation (especially when NST is abnormal or impractical, e.g., higher-order multiples)
- Preterm PROM (though continuous CTG monitoring is often preferred for identifying variable/late decelerations)
Summary Table: BPP at a Glance
| Feature | Detail |
|---|---|
| Components | NST, fetal breathing, body movement, tone, AFV |
| Scoring | 0 or 2 per variable; max 10 |
| Normal | 8/10 or 10/10 (with normal AFV) |
| Equivocal | 6/10 |
| Abnormal | ≤4/10 |
| Observation time | 30 minutes |
| Modified BPP | NST + AFI only |
| Preferred AFV method | DVP (superior to AFI for surveillance) |
The BPP remains one of the most widely used tools for antenatal fetal surveillance. A score of 8 or 10 with normal fluid is highly reassuring (predicted perinatal mortality <1/1000). A decreasing serial BPP score strongly correlates with worsening fetal acidemia and guides decisions about timing of delivery.
Apgar
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive response.
The Apgar Score
History and Purpose
The Apgar score was devised by Dr. Virginia Apgar in 1952 as a standardized, rapid method to assess the physical condition of newborns immediately after birth. The name is also a useful backronym - Appearance, Pulse, Grimace, Activity, Respiration - making it easy to remember the five components.
It serves two main purposes:
- Rapid assessment of the need for neonatal resuscitation
- Evaluation of the infant's response to resuscitation efforts
It is now considered negligence to omit Apgar scoring, especially for low birth weight babies - Park's Textbook of Preventive and Social Medicine, p. 621.
The Five Components
Each sign is scored 0, 1, or 2, giving a maximum total of 10.
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Heart Rate | Absent | <100 beats/min | ≥100 beats/min |
| Respiratory Effort | Absent | Irregular/slow/weak | Strong, crying |
| Muscle Tone | Flaccid/limp | Some flexion of extremities | Active movements, good flexion |
| Reflex Irritability (response to tactile stimulation) | No response | Grimace | Cough, sneeze, cry |
| Color (Appearance) | Blue/pale all over | Body pink, extremities blue (acrocyanosis) | Completely pink |
- Textbook of Family Medicine 9e, p. 501
- Tintinalli's Emergency Medicine, p. 716
Timing
- Assessed at 1 minute and 5 minutes after birth
- If the 5-minute score is <7, repeat at 5-minute intervals up to 20 minutes while resuscitation continues
- Resuscitation should never be delayed or interrupted to calculate the Apgar score
Score Interpretation
| Score | Interpretation | Action |
|---|---|---|
| 7-10 | Normal / No depression | Routine newborn care |
| 4-6 | Mild to moderate depression | Stimulation + supplemental O₂; close observation |
| 0-3 | Severe depression | Immediate resuscitation required |
Resuscitation guidance by 1-minute score (Morgan & Mikhail's Clinical Anesthesiology, p. 1660):
- Score 5-7 (mildly asphyxiated): Stimulation + 100% O₂ blown across the face
- Score 3-4 (moderately asphyxiated): Positive-pressure ventilation with mask and bag
- Score 0-2 (severely depressed): Immediate endotracheal intubation ± chest compressions
Clinical Significance
- A score of 0-3 at 5 minutes may correlate with neonatal death
- A persistently low Apgar score after 5 minutes despite active CPR is associated with increased morbidity and mortality - Creasy & Resnik's, p. 2766
- A low Apgar score alone cannot:
- Predict long-term neurologic outcome
- Establish whether a hypoxic event occurred in utero
- The combination of a low 5-minute score with other markers (e.g., cord pH, clinical signs of encephalopathy) is more meaningful
Factors That Affect the Apgar Score
The score can be artificially low or altered by factors unrelated to true asphyxia:
-
Gestational age (premature infants normally have lower tone, less reflex activity)
-
Maternal medications (opioids, sedatives, magnesium sulfate)
-
Neurologic conditions (neuromuscular disorders)
-
Cardiorespiratory conditions (congenital heart disease, diaphragmatic hernia)
-
Birth trauma
-
Infection/sepsis
-
Ongoing resuscitation itself (a baby being resuscitated cannot score full marks)
-
Textbook of Family Medicine 9e, p. 501
The Expanded Apgar Score
A modified version now includes a documentation section for resuscitative measures being performed at the time of scoring, acknowledging that a baby undergoing active resuscitation cannot achieve a perfect score on the traditional scale. This provides important context for interpreting low scores - Tintinalli's Emergency Medicine, p. 716.
Newborn Care Pathway Based on Apgar
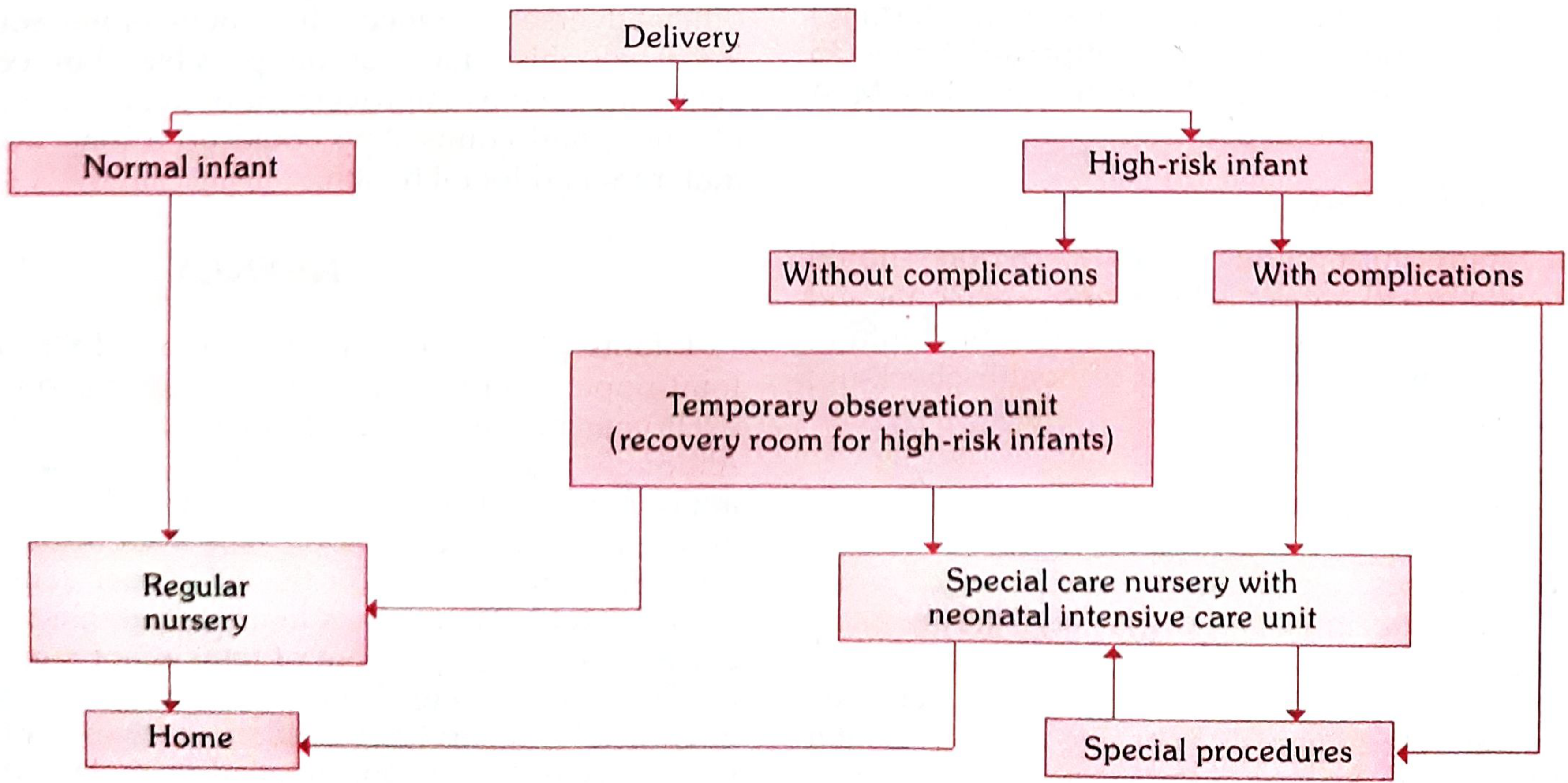
Normal infants proceed to the regular nursery and home. High-risk infants go to a temporary observation unit or directly to a special care nursery/NICU depending on the presence of complications.
Summary
| Feature | Detail |
|---|---|
| Devised by | Virginia Apgar, 1952 |
| Components | Heart rate, respirations, muscle tone, reflex irritability, color |
| Max score | 10 |
| Timing | 1 min and 5 min; repeat every 5 min up to 20 min if <7 |
| Normal | 7-10 |
| Equivocal | 4-6 |
| Severely depressed | 0-3 |
| Key limitation | Does not diagnose in-utero hypoxia or predict neurologic outcome alone |
?
It looks like your message came through as just "?" — could you clarify what you'd like to know?
Were you asking about:
- A specific aspect of the Apgar score (e.g., limitations, comparison with other scoring systems, resuscitation steps)?
- A new topic entirely?
- Something unclear from my previous answer?
Let me know and I'll help right away!
This is a shared conversation. Sign in to Orris to start your own chat.