Tracheal stenosis from scooty brown
Reading File
Finding Sources
Searching the Web
tracheal stenosis "Scooty Brown" OR "Scotti Brown" OR "Scott Brown" eponym classification
Reading File
Searching the Web
Scott-Brown's otolaryngology tracheal stenosis classification causes management
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. "Scooty Brown" is a voice-recognition/phonetic corruption of Scott-Brown's (Scott-Brown's Otorhinolaryngology Head & Neck Surgery). Here is the full answer:
Tracheal Stenosis - Scott-Brown's Otorhinolaryngology
(Note: "Scooty Brown" = Scott-Brown's Otorhinolaryngology Head & Neck Surgery, the classic ENT reference text. All content below is from that textbook.)
Overview
Laryngotracheal stenosis (LTS) is abnormal narrowing of the laryngotracheal complex causing breathlessness (particularly on exertion), retention of pulmonary secretions, cough, voice changes, and sometimes dysphagia. The narrowest site in adults is the glottis; in infants it is the subglottis.
Aetiology (National Centre for Airway Reconstruction - 600 consecutive referrals)
| Cause | Proportion |
|---|---|
| Acquired LTS (post-intubation/tracheostomy) | 50.3% (34.3% subglottic, 16% tracheal) |
| Bilateral vocal cord mobility impairment | 16.67% |
| Wegener's granulomatosis (GPA) | 10.0% |
| Idiopathic subglottic stenosis | 8.67% |
| Supraglottic stenosis (incl. sarcoid) | 5.70% |
| Previous papillomatosis / glottic web / tracheomalacia | <3% each |
Post-intubation LTS is the most common cause. Risk factors include duration of ventilation, tube sizing, excessive cuff pressures, orogastric secretion irritation, infection, immune disturbance, and individual healing biology.
Post-tracheostomy stenosis is a less common variant - usually from overtube sizing and stomal injury. Note that early tracheostomy does NOT reduce incidence of stenosis vs. prolonged ET intubation; it just makes glottic involvement less likely.
Other acquired causes: Wegener's granulomatosis (GPA - cANCA positive in ~80%), sarcoidosis, amyloidosis, inflammatory bowel disease, tuberculosis (10-37% of pulmonary TB develops endobronchial disease), fungal infections, HPV/papillomatosis.
Idiopathic LTS: Mucosal and submucosal hypertrophy sparing cartilage; almost exclusively in women.
Diagnosis
Symptoms: Exertional dyspnoea is cardinal (patients reduce activity to compensate). Chronic airway obstruction is frequently misdiagnosed as asthma or COPD.
Examination: Severity of stridor, chest recession, BMI, neck scars. Fibre-optic nasal endoscopy assesses vocal cord mobility and degree of stenosis.
Investigations:
- CT - defines location and severity; beware underestimation if scan cuts miss the apex of stenosis, and overestimation if secretions overlie it
- Spirometry and flow-volume loops - essential to quantify severity and monitor response to treatment
Characteristic Flow-Volume Loops
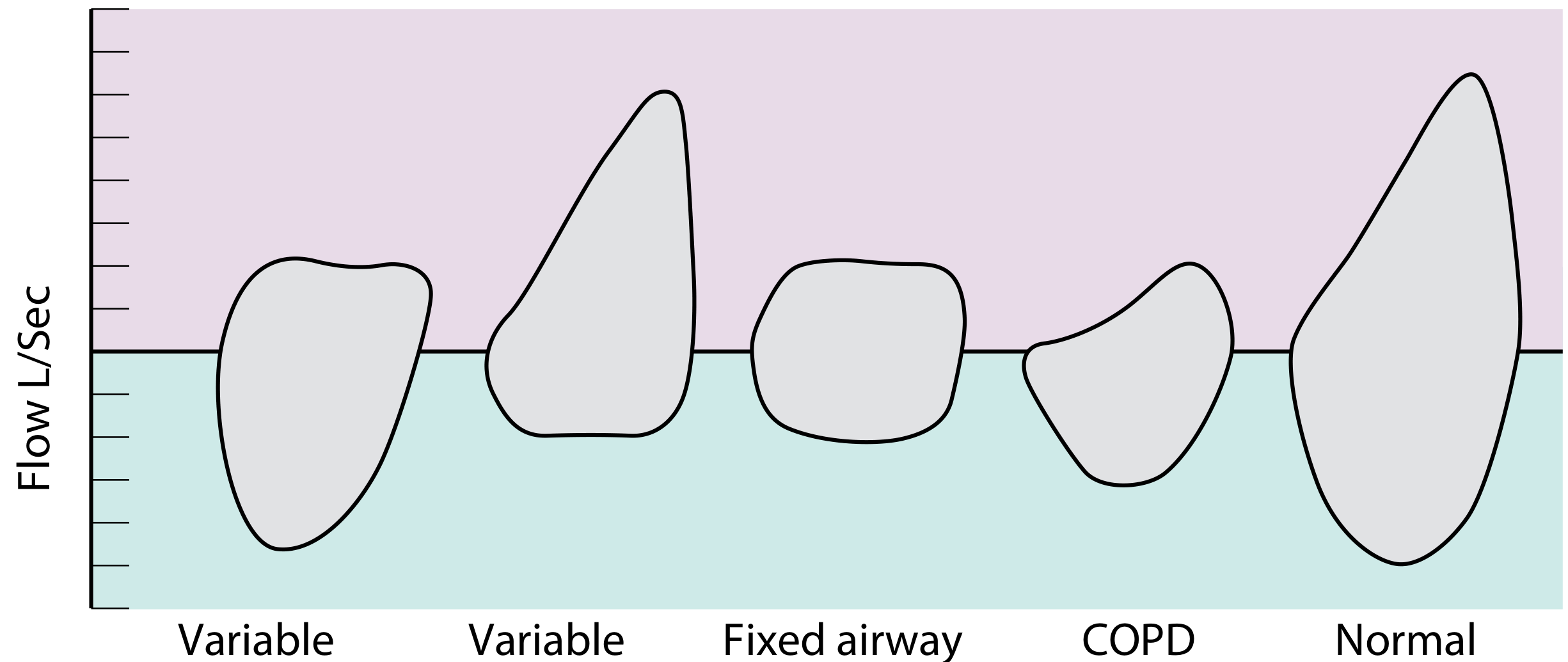
Left to right: soft intrathoracic stenosis (variable), soft extrathoracic stenosis (variable), fixed laryngeal/tracheal stenosis (classic "box" pattern), COPD, normal.
- Fixed tracheal stenosis produces a plateau (box shape) on BOTH the inspiratory and expiratory limbs
- Variable extrathoracic - plateau only on inspiration
- Variable intrathoracic - plateau only on expiration
Endoscopy remains the gold standard for characterising the stenosis and directing therapy. The key endoscopic question is: is the cartilaginous framework intact?
Classification - Myer-Cotton Grading System
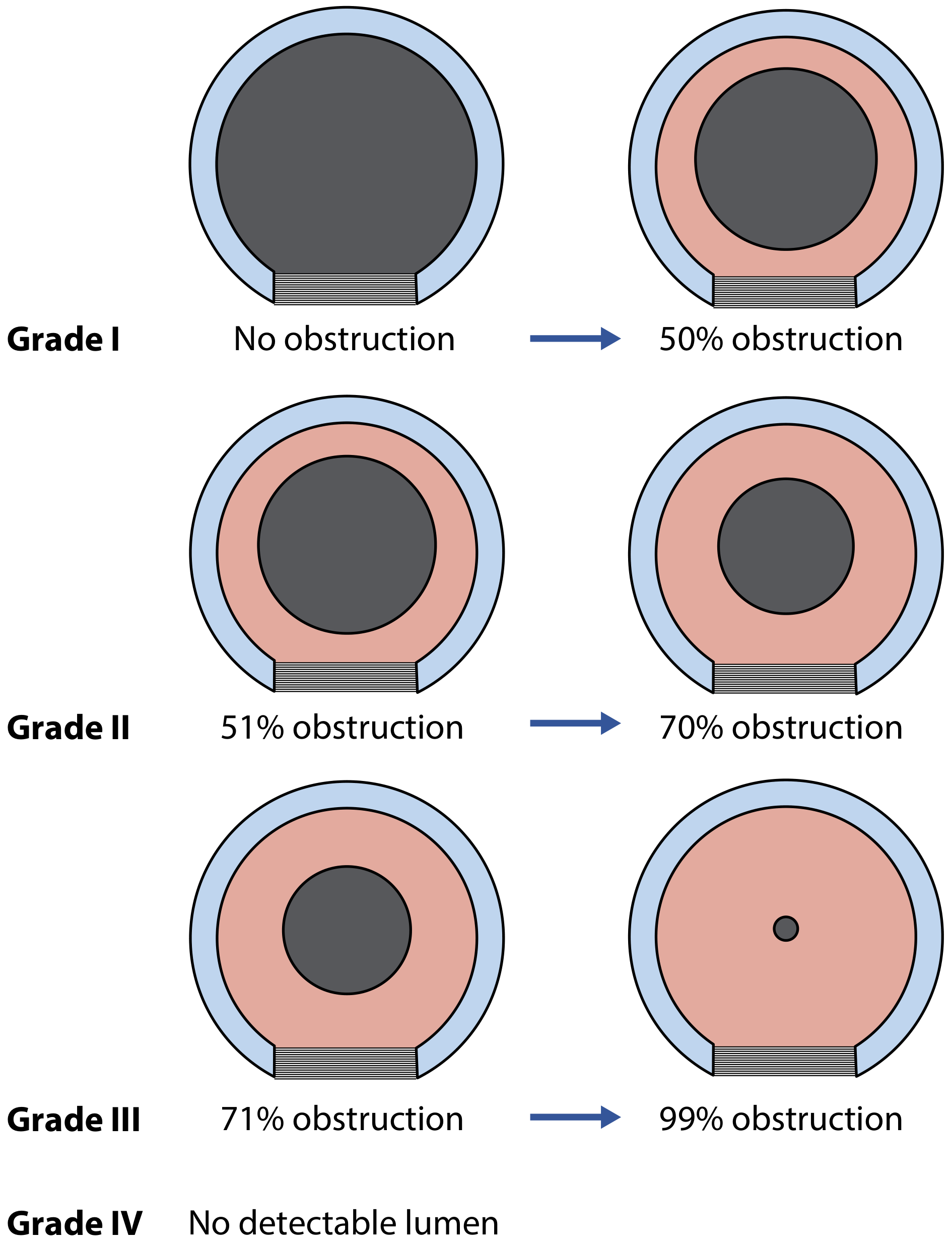
| Grade | Degree of Obstruction |
|---|---|
| Grade I | 0-50% obstruction |
| Grade II | 51-70% obstruction |
| Grade III | 71-99% obstruction |
| Grade IV | No detectable lumen |
Management
Endoscopic Approach (for inflammatory/fibro-inflammatory lesions with intact cartilage)
- Intralesional steroid injection - up to 3 ml Depo-Medrone (40 mg/ml) injected into the stenosis
- CO2 laser radial cuts - 3-4 radial cuts at 8-10 watts using operating microscope
- Balloon dilation - to size of adjacent normal airway using a pulmonary balloon dilator
For mature fibrotic lesions with intact cartilage: radial laser cuts + balloon dilation + topical mitomycin-C (MMC, 1 mg/ml for 3 min). MMC is an antifibrotic from Streptomyces caespitosus that inhibits scar formation.
- If more than 3 endoscopic interventions are required without success, consider open surgery.
Open Surgery (for cartilage damage or failed endoscopic treatment)
- Tracheal resection and end-to-end anastomosis - definitive treatment for most short-segment isolated tracheal stenosis. Suitable for 1-4 cm lesions, not high subglottic, in operable patients.
- Cricotracheal resection - for subglottic and high tracheal stenosis
- Laryngotracheal reconstruction (LTR) - when cartilage needs rebuilding (uses costal cartilage or other grafts)
- Augmentation with buccal mucosa graft - for refractory cases; keratinocytes provide antifibrotic activity
Airway Stenting (palliation only)
Indications: long-length stenosis, failed repair, inoperable patient, or patient preference.
- Silicone stents - easier to remove but higher migration risk; require GA and rigid bronchoscopy for placement. Lower biofouling in upper trachea.
- Metal (wire) stents - can be placed under local anaesthesia but: prone to obstruction with granulation tissue, metal fatigue, fracture, and permanent fixation if not removed within first few weeks. Colonised by Staphylococcus aureus and Pseudomonas aeruginosa.
Key point: Stents are NOT a good long-term solution for LTS - they are prone to migration, fouling, and (for metal stents) fragmentation and granulation. Uncovered metal stents should only be used in patients with short life expectancy.
Disease-Specific Treatment
- GPA (Wegener's): Systemic immunosuppression (cyclophosphamide + steroids) as primary therapy; endoscopic intervention (steroid injection + CO2 laser + balloon dilation) for local stenosis. Subglottic involvement in ~25%.
- Sarcoidosis / amyloidosis / IBD-associated: Immunosuppression + endobronchial interventions; surgery for refractory cases.
- TB stenosis: Anti-TB treatment with adjunctive endobronchial procedures.
Key Points (from Scott-Brown's)
- The most common cause of LTS is ICU intubation and ventilation
- Early tracheostomy does not reduce LTS incidence; it reduces glottic involvement
- Systemic inflammatory disease LTS (GPA, sarcoid) should be managed endoscopically where possible, avoiding tracheostomies and stents
- If the cartilaginous framework is damaged, endoscopic surgery will not restore a normal airway - open resection or LTR is required
- Prevention is critical: appropriate tube sizing, monitoring cuff pressures (<30 cm H2O), early tracheostomy in prolonged ventilation, and early recognition and treatment of airway injuries
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 76 - Laryngotracheal Stenosis, pp. 1122-1135
This is a shared conversation. Sign in to Orris to start your own chat.