hello
why proteus shows swarming motility
Proteus mirabilis swarming motility mechanism flagella differentiation
Swarming Motility in Proteus mirabilis
What is Swarming?
The Core Mechanism: Swimmer → Swarmer Cell Differentiation
| Feature | Swimmer Cell | Swarmer Cell |
|---|---|---|
| Length | ~2 µm | 60-80 µm |
| Flagella | 4-10 | Thousands (hyperflagellated) |
| Nucleoids | Normal, separated | Multinucleated (no septation) |
| Environment | Liquid | Solid/semi-solid surfaces |
Step-by-Step: How Swarming is Triggered
-
Surface sensing - When flagellar rotation is physically inhibited by a solid surface (increased viscosity/resistance), the bacterium "senses" it is on a solid surface. This impedance of flagellar rotation acts as the trigger signal.
-
Gene upregulation - The master regulator operon flhDC is upregulated. This drives overexpression of flagellin genes, resulting in massive flagella synthesis. Hundreds to thousands of flagella are produced.
-
Cell elongation - Cell division is suppressed (septation is inhibited), but DNA replication continues. This creates long, multinucleated cells.
-
Collective migration - Swarmer cells align and move together in coordinated waves, propelled by their bundled flagella.
-
Consolidation - After a period of migration, swarmer cells consolidate back into swimmer cells. The cycle then repeats, creating the characteristic concentric ring (bull's-eye) pattern on agar plates.
Other Signals That Regulate Swarming
- Putrescine (a polyamine) acts as an extracellular signal; its biosynthesis genes (speA, speB) are needed for timely swarmer differentiation
- Quorum sensing - Cell density signals contribute to coordinating the collective migration
- Surface wetness - A thin fluid film on the surface is required for flagellar function
Why Does it Matter Clinically?
- Swarming is directly linked to virulence - swarmer cells co-express urease, hemolysin, and fimbriae at higher levels
- It facilitates catheter-associated UTIs (CAUTIs) - Proteus can literally swarm up urinary catheters to reach the bladder and upper urinary tract
- Swarmer cells can invade epithelial cells in vitro
- The urease produced (very potent compared to other Enterobacteriaceae) alkalinizes urine and contributes to struvite/urinary stone formation
Laboratory Recognition
- On agar plates: spreading, concentric ring growth (bull's-eye pattern) that can overgrow other organisms in culture, delaying isolation of other pathogens - a common frustration for microbiologists
- Distinct ammoniac odor due to urease activity
- Lactose-negative, H₂S positive, indole-negative (P. mirabilis) or indole-positive (P. vulgaris)
tell me why alchol causes acute pancreatitis
alcohol induced acute pancreatitis pathophysiology mechanism 2024
How Alcohol Causes Acute Pancreatitis
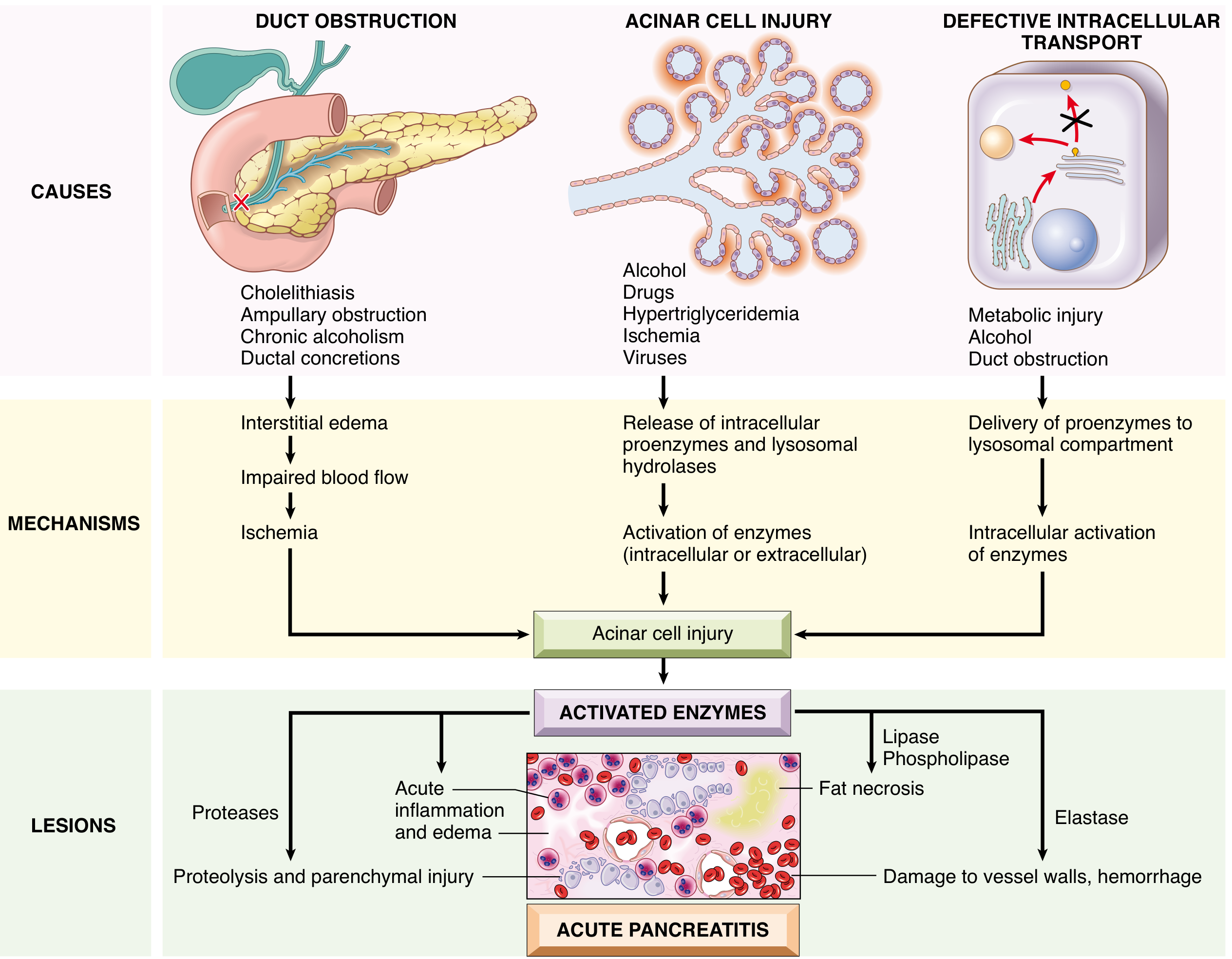
The Central Event: Premature Trypsin Activation
Mechanism 1: Duct Obstruction
- Alcohol causes transient spasm of the sphincter of Oddi (the muscle at the papilla of Vater), increasing intraductal pressure
- Chronic alcohol consumption leads to the secretion of protein-rich pancreatic juice that is prone to forming inspissated protein plugs - these physically obstruct small pancreatic ducts
- Obstruction raises intrapancreatic ductal pressure → enzyme-rich fluid leaks into the interstitium → lipase (secreted in active form) causes local fat necrosis → "danger signals" trigger leukocyte infiltration and microvascular leak → edema → ischemic injury to acinar cells
Mechanism 2: Direct Acinar Cell Injury (Toxic/Metabolic)
- Ethanol is metabolized in acinar cells via oxidative (alcohol dehydrogenase/CYP2E1) and non-oxidative pathways, generating toxic metabolites:
- Acetaldehyde - directly damages cell membranes and mitochondria
- Fatty acid ethyl esters (FAEEs) - non-oxidative metabolites that are cytotoxic
- Reactive oxygen species (ROS) - cause lipid peroxidation and membrane damage
- This oxidative stress damages mitochondria, which raises intracellular calcium (Ca²⁺)
- Elevated intracellular Ca²⁺ is a critical trigger: normally low Ca²⁺ allows trypsin to self-inactivate (autoinhibition), but when Ca²⁺ rises, this protection is lost and trypsin auto-activation is favored
- Activated trypsin then sets off a proteolytic cascade activating elastase, phospholipase A₂, etc., causing autodigestion
Mechanism 3: Defective Intracellular Transport (Lysosomal Co-localization)
- Alcohol promotes the aberrant fusion of lysosomes and zymogen granules within acinar cells
- Lysosomal hydrolases (especially cathepsins) then come in contact with trypsinogen and activate it intracellularly
- This bypasses the normal secretory pathway and results in enzyme activation before reaching the duodenum
The Final Cascade: What the Activated Enzymes Do
| Activated Enzyme | Damage Caused |
|---|---|
| Trypsin / Proteases | Protein degradation, parenchymal injury, coagulation pathway activation |
| Elastase | Digests vessel walls → hemorrhage |
| Phospholipase A₂ | Destroys cell membranes; damages alveolar surfactant (→ ARDS) |
| Lipase | Fat necrosis (chalky white deposits - calcium saponification) |
Why Don't All Alcoholics Get Pancreatitis?
- CLDN2 gene variant (claudin-2, a tight junction protein on X chromosome) - nearly doubles risk in males with alcoholic pancreatitis
- Mutations in PRSS1, SPINK1, CFTR increase susceptibility when combined with alcohol
- Smoking potentiates alcohol-induced pancreatic microcirculatory damage
explain me whole renal physiology from standard physiology textbook
Renal Physiology - Complete Overview
1. Functional Anatomy of the Nephron
- Glomerulus (~200 µm) - a tuft of capillaries inside Bowman's capsule
- Bowman's capsule - collects the filtrate
- Proximal convoluted tubule (PCT)
- Loop of Henle (descending thin limb → ascending thin → ascending thick limb)
- Distal convoluted tubule (DCT)
- Collecting duct (cortical → medullary → duct of Bellini → renal pelvis)
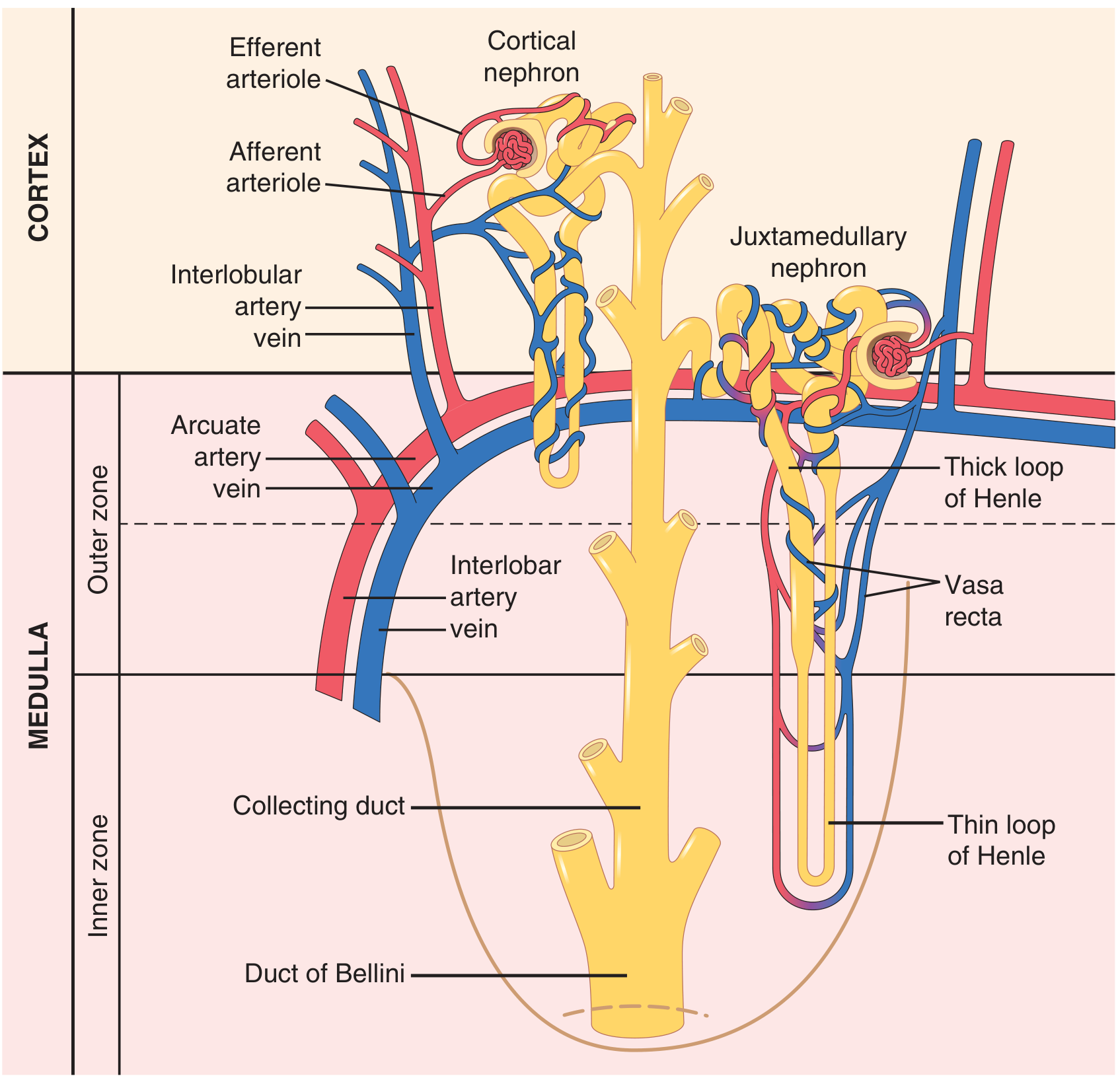
Two types of nephrons:
| Type | Location | Loop of Henle | Role |
|---|---|---|---|
| Cortical nephrons (~75%) | Outer cortex | Short, barely enters medulla | General filtration |
| Juxtamedullary nephrons (~25%) | Near corticomedullary junction | Long, dips deep into medulla | Urine concentration via countercurrent |
Blood Supply (critical to understand):
- Renal artery → interlobar → arcuate → interlobular arteries → afferent arteriole
- Afferent arteriole → glomerular capillaries → efferent arteriole
- Efferent arteriole → peritubular capillaries (cortex) and vasa recta (medulla)
- Peritubular capillaries → interlobular veins → renal vein
The presence of two capillary beds in series (glomerular + peritubular) is unique to the kidney and fundamental to its physiology.
2. The Three Core Renal Processes
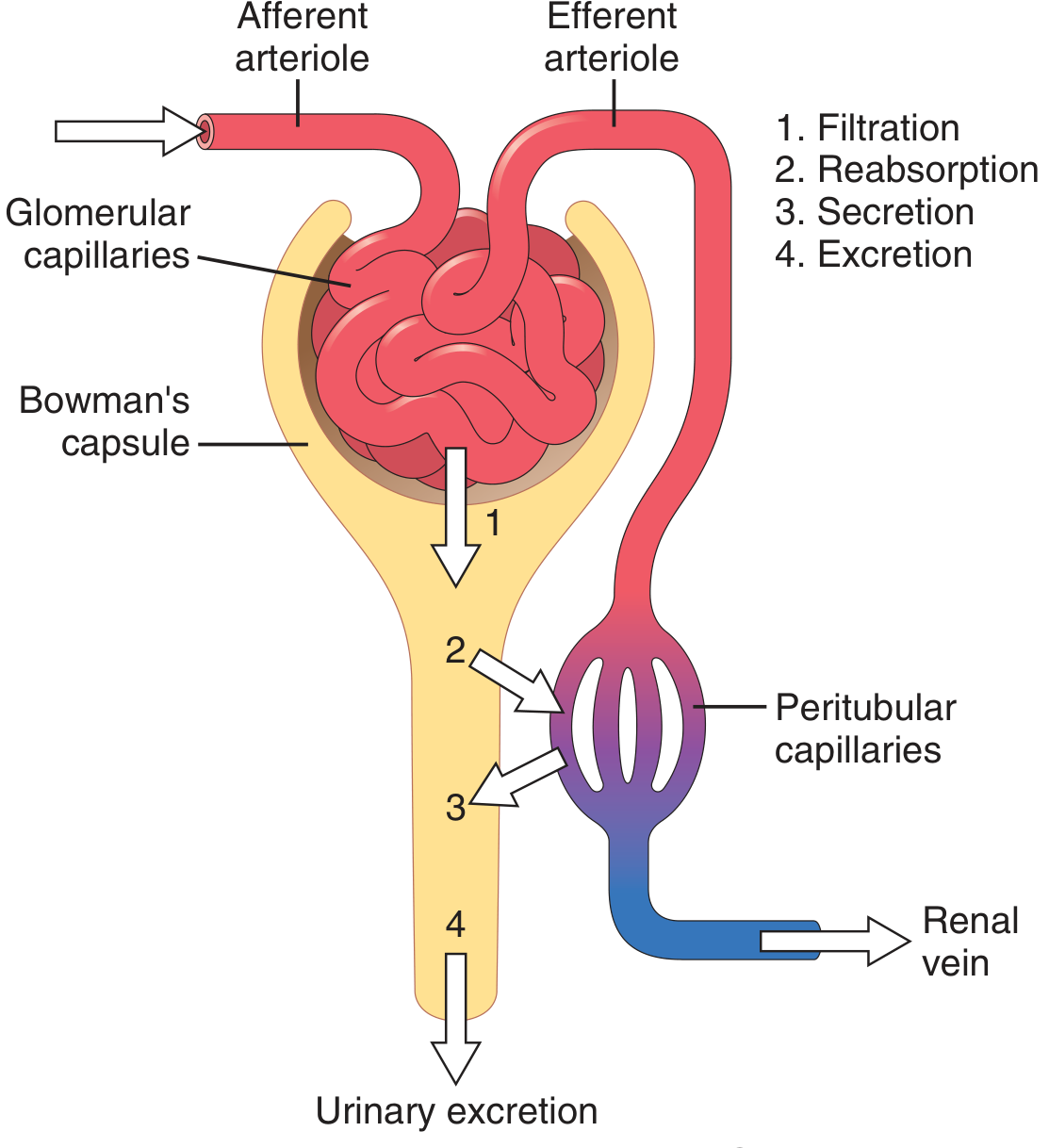
Urinary Excretion = Filtration - Reabsorption + Secretion
3. Glomerular Filtration
What is Filtered?
GFR - Glomerular Filtration Rate
- Normal GFR = 125 mL/min (180 L/day filtered!)
- Of this, only ~1.5 L/day is excreted as urine - meaning >99% of filtrate is reabsorbed
Starling Forces Governing Filtration
| Force | Value | Direction |
|---|---|---|
| Glomerular capillary hydrostatic pressure (Pgc) | ~60 mmHg | Promotes filtration |
| Bowman's capsule hydrostatic pressure (Pbs) | ~18 mmHg | Opposes filtration |
| Glomerular oncotic pressure (πgc) | ~32 mmHg | Opposes filtration |
| Net filtration pressure | ~10 mmHg | Net = promotes filtration |
Factors that Alter GFR:
- Increased afferent arteriole dilation (e.g., prostaglandins, ANP)
- Increased blood pressure (within autoregulatory range)
- Decreased plasma oncotic pressure
- Afferent arteriole constriction (sympathetic activity, angiotensin II at high doses)
- Efferent arteriole dilation (ACE inhibitors - reduce efferent constriction)
- Increased Bowman's capsule pressure (urinary obstruction)
- Decreased Kf (glomerular disease)
Renal Autoregulation
- Myogenic mechanism - stretch of afferent arteriole wall → vasoconstriction
- Tubuloglomerular feedback (TGF) - macula densa senses NaCl delivery; if high → afferent arteriole constricts → reduces GFR
Measuring GFR - Clearance Concept
Clearance = (Urine concentration × Urine flow) / Plasma concentration = U×V/P
4. Tubular Reabsorption and Secretion
Proximal Convoluted Tubule (PCT)
- Basolateral Na⁺/K⁺-ATPase is the primary engine - pumps 3 Na⁺ out, 2 K⁺ in, maintaining low intracellular Na⁺
- This creates a gradient driving Na⁺ into the cell from the lumen via:
- Na⁺-glucose cotransporter (SGLT2) - reabsorbs glucose with Na⁺ (site of action of SGLT2 inhibitors)
- Na⁺-amino acid cotransporters
- Na⁺/H⁺ antiporter (couples Na⁺ entry with H⁺ secretion → HCO₃⁻ reabsorption)
- Water follows passively through aquaporin-1 (AQP1) channels (PCT is always water permeable)
- The reabsorption here is isosmotic - fluid remains at 300 mOsm/L
- All filtered glucose is normally reabsorbed (normal plasma glucose ~100 mg/dL)
- Transport maximum (Tm) for glucose ≈ 375 mg/min
- Renal threshold for glucose ≈ plasma glucose of 180-200 mg/dL
- Above this: glucosuria occurs (e.g., in diabetes mellitus)
Loop of Henle
| Segment | Na⁺/Solute | Water | Net Effect |
|---|---|---|---|
| Thin descending limb | No active transport | Permeable (AQP1) | Fluid becomes hypertonic (water leaves) |
| Thin ascending limb | Some passive NaCl out | Impermeable | Fluid dilutes slightly |
| Thick ascending limb | Active Na⁺/K⁺/2Cl⁻ cotransport (NKCC2) | Impermeable | Fluid becomes hypotonic (~100 mOsm/L); medulla becomes concentrated |
The thick ascending limb is the diluting segment - it pumps out solute without water. This is the site of action of loop diuretics (furosemide), which block NKCC2.
Distal Convoluted Tubule (DCT)
- Reabsorbs Na⁺ and Cl⁻ via NaCl cotransporter (NCC) - blocked by thiazide diuretics
- Begins to become regulated (responds to aldosterone in late DCT)
- Early DCT: water impermeable - continues dilution
- Fluid entering DCT is ~100 mOsm/L (hypotonic)
Collecting Duct (CD) - the "fine-tuning" segment
- Reabsorb Na⁺ via ENaC (epithelial sodium channels) on apical membrane
- Secrete K⁺ via ROMK channels
- Regulated by aldosterone (increases ENaC and K⁺-ATPase expression)
- Water reabsorption regulated by ADH/vasopressin (inserts AQP2 on apical membrane)
- Secrete H⁺ (via H⁺-ATPase) → important for acid-base regulation
- Reabsorb HCO₃⁻
5. Concentration and Dilution of Urine
The Countercurrent Multiplier (Loop of Henle)
- Active NaCl pumping out of the thick ascending limb (impermeable to water) → deposits solute into medullary interstitium
- Urea recycling - urea diffuses out of the inner medullary collecting duct into the interstitium (especially in the presence of ADH), adding ~500 mOsm/L to the inner medulla
- The descending limb (permeable to water) equilibrates with the hypertonic interstitium - water leaves, fluid inside becomes concentrated
- The cycle multiplies the gradient with each loop - hence "multiplier"
The Countercurrent Exchanger (Vasa Recta)
How ADH Controls Final Urine Concentration
- Collecting duct is water-impermeable
- Hypotonic fluid (100 mOsm/L) coming from DCT passes through without losing water
- Dilute urine is produced (as low as 50 mOsm/L)
- ADH binds V2 receptors on principal cells → activates adenylyl cyclase → ↑ cAMP → PKA activation → AQP2 vesicles fuse with apical membrane
- Collecting duct becomes highly water permeable
- Water rushes out into the hypertonic medullary interstitium
- Concentrated urine is produced (up to 1200-1400 mOsm/L)
This is the basis of diabetes insipidus - absent ADH (central DI) or non-functioning V2 receptors (nephrogenic DI) → massive dilute urine output.
6. Hormonal Regulation of Kidney Function
Renin-Angiotensin-Aldosterone System (RAAS)
| Step | Where | What Happens |
|---|---|---|
| Low BP / low Na delivery to macula densa / sympathetic activity | Juxtaglomerular (JG) cells | Release renin |
| Renin acts on angiotensinogen (liver) | Plasma | → Angiotensin I |
| ACE (lung endothelium) | Plasma | → Angiotensin II |
| Ang II → adrenal cortex | Zona glomerulosa | → releases aldosterone |
| Aldosterone → collecting duct principal cells | Kidney | ↑ ENaC + Na⁺/K⁺-ATPase → ↑ Na⁺ reabsorption, ↑ K⁺ excretion |
| Ang II also acts directly on PCT | PCT | ↑ Na⁺/H⁺ antiporter → ↑ Na⁺ reabsorption |
ADH (Vasopressin)
- Produced in hypothalamus (supraoptic and paraventricular nuclei), released from posterior pituitary
- Stimulated by: ↑ plasma osmolarity, ↓ blood volume
- Actions: Water retention (collecting duct AQP2), vasoconstriction (V1 receptor)
Atrial Natriuretic Peptide (ANP)
- Released by atria when stretched (high blood volume)
- Effects: ↑ GFR (dilates afferent, constricts efferent arteriole), ↓ renin, ↓ aldosterone, ↓ ADH
- Net: Natriuresis + diuresis → reduces blood volume
Parathyroid Hormone (PTH)
- Increases Ca²⁺ reabsorption in DCT
- Decreases phosphate reabsorption in PCT
- Stimulates 1α-hydroxylase in kidney (activates Vitamin D → 1,25-(OH)₂D₃)
7. Renal Handling of Specific Substances
| Substance | Filtered | PCT | Loop | DCT/CD | Net |
|---|---|---|---|---|---|
| Sodium | Yes | 65-70% reabsorbed | 25% (thick ALH) | ~5% (regulated) | <1% excreted |
| Glucose | Yes | 100% reabsorbed (Tm-limited) | - | - | 0 excreted normally |
| Potassium | Yes | 65% reabsorbed | 25% reabsorbed | Secreted (aldosterone) | Variable |
| Urea | Yes | 50% reabsorbed | Secreted (thin) | Reabsorbed (IMCD) | ~50% excreted |
| Creatinine | Yes | Not reabsorbed | - | Small secretion | ~100% excreted |
| HCO₃⁻ | Yes | 80-90% reabsorbed | ~5% | Final regulation | Minimal excretion |
| H⁺ | - | Secreted (Na/H antiporter) | - | Secreted (H⁺-ATPase) | Acid-base balance |
| Phosphate | Yes | 85% reabsorbed (PTH inhibits) | - | - | 15% excreted |
| Calcium | Yes | 65% passive | 25% (TAL) | Active (PTH) | <2% excreted |
8. Renal Control of Acid-Base Balance
-
HCO₃⁻ reabsorption - PCT reabsorbs ~80-90% via Na⁺/H⁺ antiporter. H⁺ secreted reacts with filtered HCO₃⁻ → H₂CO₃ → CO₂ + H₂O (carbonic anhydrase) → CO₂ enters cell → reformed as HCO₃⁻ → basolateral exit to blood. Net: HCO₃⁻ is "reclaimed."
-
Titratable acid excretion - H⁺ secreted in collecting duct combines with HPO₄²⁻ → H₂PO₄⁻, which is excreted. This excretes fixed acid.
-
Ammonium (NH₄⁺) excretion - PCT generates NH₃ from glutamine (glutaminase); NH₃ + H⁺ → NH₄⁺, which is trapped in the tubular lumen and excreted. This is the most important mechanism in chronic acidosis.
9. Renal Clearance - Key Values to Know
| Substance | Clearance | Meaning |
|---|---|---|
| Glucose | 0 mL/min | Fully reabsorbed |
| Sodium | ~0.9 mL/min | Mostly reabsorbed |
| Potassium | ~12 mL/min | Reabsorbed + some net secretion |
| Inulin | 125 mL/min | = GFR (gold standard) |
| Creatinine | ~140 mL/min | Slightly secreted, overestimates GFR |
| PAH (para-aminohippuric acid) | ~650 mL/min | = Renal plasma flow (RPF); fully secreted |
10. Summary: Flow of Fluid Through the Nephron
Plasma → Glomerular filtration → Bowman's capsule (300 mOsm/L)
↓
PCT: isosmotic reabsorption (Na⁺, glucose, AA, HCO₃⁻, water) → 65-70% reabsorbed
↓
Descending LOH: water leaves → fluid concentrates to ~1200 mOsm at tip
↓
Ascending LOH (thin): NaCl passively diffuses out, no water → dilutes slightly
↓
Thick ALH: active NaCl pump, NO water → fluid dilutes to ~100 mOsm
↓
DCT: further NaCl reabsorption (NCC), starts aldosterone response
↓
Collecting duct:
+ ADH → AQP2 inserted → water reabsorbed → concentrated urine (up to 1200 mOsm)
- ADH → water stays → dilute urine (~50-100 mOsm)
+ Aldosterone → more Na⁺ reabsorbed, K⁺ secreted
↓
Final urine → renal pelvis → ureter → bladder → excreted
Create a comprehensive study guide PDF on renal physiology with diagrams and tables
ls /home/daytona/workspace/ 2>/dev/null && mkdir -p /home/daytona/workspace/rena…
~/renal-physiology-guide/create_pdf.py
#!/usr/bin/env python3
"""
Comprehensive Renal Physiology Study Guide PDF
Generated with ReportLab
"""
import json, subprocess, base64, os
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
PageBreak, HRFlowable, Image, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus.flowables import HRFlowable
from reportlab.graphics.shapes import Drawing, Rect, String, Line, Arrow, Polygon, Circle
from reportlab.graphics import renderPDF
from reportlab.graphics.shapes import Drawing, Rect, String, Line, Group
from io import BytesIO
# ─────────────────────────────────────────────────────────
# Colour Palette
# ─────────────────────────────────────────────────────────
NAVY = colors.HexColor("#1a3a5c")
TEAL = colors.HexColor("#2980b9")
LIGHT_BLUE= colors.HexColor("#d6eaf8")
GOLD = colors.HexColor("#f39c12")
ORANGE = colors.HexColor("#e67e22")
GREEN = colors.HexColor("#27ae60")
LIGHT_GREEN = colors.HexColor("#d5f5e3")
RED = colors.HexColor("#c0392b")
LIGHT_RED = colors.HexColor("#fadbd8")
PURPLE = colors.HexColor("#8e44ad")
LIGHT_PURPLE = colors.HexColor("#e8daef")
GRAY = colors.HexColor("#7f8c8d")
LIGHT_GRAY= colors.HexColor("#f2f3f4")
WHITE = colors.white
DARK = colors.HexColor("#2c3e50")
# ─────────────────────────────────────────────────────────
# Page setup
# ─────────────────────────────────────────────────────────
OUTPUT = "/home/daytona/workspace/renal-physiology-guide/Renal_Physiology_Study_Guide.pdf"
PAGE_W, PAGE_H = A4
MARGIN = 2 * cm
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=MARGIN, rightMargin=MARGIN,
topMargin=2.2*cm, bottomMargin=2*cm,
title="Renal Physiology – Comprehensive Study Guide",
author="Orris Medical Education",
subject="Renal Physiology"
)
# ─────────────────────────────────────────────────────────
# Styles
# ─────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
def make_style(name, parent="Normal", **kwargs):
return ParagraphStyle(name, parent=styles[parent], **kwargs)
ST_TITLE = make_style("MyTitle", "Title", fontSize=26, textColor=NAVY,
spaceAfter=6, leading=32, alignment=TA_CENTER)
ST_SUBTITLE = make_style("MySubtitle","Normal", fontSize=13, textColor=TEAL,
spaceAfter=4, alignment=TA_CENTER, italic=True)
ST_H1 = make_style("H1", "Heading1", fontSize=15, textColor=WHITE,
spaceAfter=6, spaceBefore=14, leading=18)
ST_H2 = make_style("H2", "Heading2", fontSize=12, textColor=NAVY,
spaceAfter=4, spaceBefore=10, leading=15)
ST_H3 = make_style("H3", "Heading3", fontSize=10.5, textColor=TEAL,
spaceAfter=3, spaceBefore=6, leading=13)
ST_BODY = make_style("Body", "Normal", fontSize=9.5, leading=14,
spaceAfter=4, alignment=TA_JUSTIFY)
ST_BULLET = make_style("Bullet", "Normal", fontSize=9.5, leading=13,
spaceAfter=2, leftIndent=14, bulletIndent=4)
ST_BOX = make_style("Box", "Normal", fontSize=9, leading=13,
spaceAfter=2, leftIndent=6, textColor=DARK)
ST_CAPTION = make_style("Caption", "Normal", fontSize=8.5, italic=True,
textColor=GRAY, alignment=TA_CENTER, spaceAfter=4)
ST_KEY = make_style("Key", "Normal", fontSize=9.5, textColor=RED,
leading=13, spaceAfter=2, leftIndent=14,
fontName="Helvetica-Bold")
ST_FORMULA = make_style("Formula", "Normal", fontSize=10,
textColor=NAVY, fontName="Helvetica-Bold",
alignment=TA_CENTER, spaceAfter=6, spaceBefore=4)
# ─────────────────────────────────────────────────────────
# Helper: section header with coloured band
# ─────────────────────────────────────────────────────────
def section_header(text, color=NAVY, num=""):
label = f"{num} {text}" if num else text
p = Paragraph(f"<font color='white'><b>{label}</b></font>", ST_H1)
t = Table([[p]], colWidths=[PAGE_W - 2*MARGIN])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), color),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING",(0,0),(-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS", [4]),
]))
return t
def sub_header(text, color=TEAL):
p = Paragraph(f"<b>{text}</b>", ST_H2)
return p
def key_point(text):
return Paragraph(f"<b>★</b> {text}", ST_KEY)
def bullet(text, indent=0):
style = ParagraphStyle("bul", parent=ST_BULLET, leftIndent=14+indent*12)
return Paragraph(f"• {text}", style)
def body(text):
return Paragraph(text, ST_BODY)
def formula(text):
return Paragraph(text, ST_FORMULA)
def spacer(h=0.3):
return Spacer(1, h*cm)
def hr(color=TEAL, thickness=0.5):
return HRFlowable(width="100%", thickness=thickness, color=color, spaceAfter=4, spaceBefore=4)
# ─────────────────────────────────────────────────────────
# Helper: styled table
# ─────────────────────────────────────────────────────────
def make_table(header, rows, col_widths=None, header_color=NAVY, alt_color=LIGHT_BLUE):
data = [[Paragraph(f"<b><font color='white'>{h}</font></b>", ST_BOX) for h in header]]
for i, row in enumerate(rows):
data.append([Paragraph(str(c), ST_BOX) for c in row])
if col_widths is None:
avail = PAGE_W - 2*MARGIN
col_widths = [avail / len(header)] * len(header)
t = Table(data, colWidths=col_widths, repeatRows=1)
style = [
("BACKGROUND", (0,0), (-1,0), header_color),
("ROWBACKGROUNDS", (0,1), (-1,-1), [WHITE, alt_color]),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#bdc3c7")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]
t.setStyle(TableStyle(style))
return t
# ─────────────────────────────────────────────────────────
# Helper: info box
# ─────────────────────────────────────────────────────────
def info_box(title, lines, bg=LIGHT_BLUE, border=TEAL):
content = [Paragraph(f"<b>{title}</b>", ST_H3)]
for l in lines:
content.append(Paragraph(f"• {l}", ST_BOX))
t = Table([[content]], colWidths=[PAGE_W - 2*MARGIN])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("BOX", (0,0), (-1,-1), 1.5, border),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING",(0,0),(-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING",(0,0), (-1,-1), 10),
]))
return t
# ─────────────────────────────────────────────────────────
# Diagram helpers (pure ReportLab Drawing objects)
# ─────────────────────────────────────────────────────────
def nephron_flow_diagram():
"""Simple flow diagram of nephron segments"""
d = Drawing(480, 200)
segments = [
("Bowman's\nCapsule", 0, TEAL, "300 mOsm"),
("PCT", 90, GREEN, "~300 mOsm\n65% reabs."),
("Loop of\nHenle", 180, ORANGE,"100 mOsm\n(exit)"),
("DCT", 270, PURPLE,"~100 mOsm"),
("Collecting\nDuct", 360, RED, "50-1400\nmOsm"),
]
for (label, x, col, osm) in segments:
# box
d.add(Rect(x+2, 60, 78, 70, fillColor=col, strokeColor=WHITE, strokeWidth=1.5, rx=6, ry=6))
# label
for i, line in enumerate(label.split("\n")):
d.add(String(x+41, 115 - i*12, line, fontSize=8, fillColor=WHITE,
textAnchor="middle", fontName="Helvetica-Bold"))
# osmolarity below
for i, line in enumerate(osm.split("\n")):
d.add(String(x+41, 52 - i*11, line, fontSize=7.5, fillColor=col,
textAnchor="middle"))
# arrow between boxes
if x < 360:
d.add(Line(x+82, 95, x+90, 95, strokeColor=GRAY, strokeWidth=1.5))
d.add(Polygon([x+88, 99, x+88, 91, x+94, 95], fillColor=GRAY, strokeColor=GRAY))
# Labels at top
d.add(String(240, 185, "Nephron Segment Flow & Osmolarity",
fontSize=11, textAnchor="middle", fontName="Helvetica-Bold", fillColor=NAVY))
d.add(String(240, 170, "(Numbers = approximate tubular fluid osmolarity)",
fontSize=8, textAnchor="middle", fillColor=GRAY))
return d
def starling_forces_diagram():
"""Starling forces at the glomerulus"""
d = Drawing(480, 160)
# Glomerulus circle
d.add(Circle(120, 80, 55, fillColor=colors.HexColor("#f5cba7"),
strokeColor=ORANGE, strokeWidth=2))
d.add(String(120, 78, "Glomerular", fontSize=9, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=DARK))
d.add(String(120, 66, "Capillary", fontSize=9, textAnchor="middle", fillColor=DARK))
# Forces arrows and labels
forces = [
# (x1,y1,x2,y2, label, value, color, direction)
(180, 80, 300, 80, "Pgc (hydrostatic)", "60 mmHg", GREEN, "→ promotes"),
(120, 140, 120, 170, "Pbs (capsule P)", "18 mmHg", RED, "↑ opposes"),
(60, 80, -30, 80, "πgc (oncotic)", "32 mmHg", PURPLE, "← opposes"),
]
# Net
d.add(Rect(310, 50, 160, 65, fillColor=LIGHT_GREEN, strokeColor=GREEN, strokeWidth=1.5, rx=4, ry=4))
d.add(String(390, 105, "NET FILTRATION", fontSize=9, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=GREEN))
d.add(String(390, 91, "PRESSURE", fontSize=9, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=GREEN))
d.add(String(390, 77, "60 - 18 - 32", fontSize=10, textAnchor="middle", fillColor=DARK))
d.add(String(390, 63, "= ~10 mmHg", fontSize=11, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=NAVY))
# Force labels on left
labels = [
(10, 148, "Pgc = 60 mmHg (promotes filtration)", GREEN),
(10, 134, "Pbs = 18 mmHg (opposes filtration)", RED),
(10, 120, "pgc = 32 mmHg (opposes filtration)", PURPLE),
]
for (x, y, txt, col) in labels:
d.add(String(x, y, txt, fontSize=8, fillColor=col))
d.add(String(240, 10, "Starling Forces at the Glomerulus",
fontSize=10, textAnchor="middle", fontName="Helvetica-Bold", fillColor=NAVY))
return d
def countercurrent_diagram():
"""Simplified countercurrent multiplier"""
d = Drawing(480, 230)
d.add(String(240, 218, "Countercurrent Multiplier – Osmolarity Gradient",
fontSize=10, textAnchor="middle", fontName="Helvetica-Bold", fillColor=NAVY))
# Cortex / Medulla labels
d.add(Rect(0, 150, 480, 60, fillColor=colors.HexColor("#fef9e7"),
strokeColor=GOLD, strokeWidth=1))
d.add(String(10, 192, "CORTEX", fontSize=9, fontName="Helvetica-Bold", fillColor=GOLD))
d.add(Rect(0, 0, 480, 150, fillColor=colors.HexColor("#eaf2ff"),
strokeColor=TEAL, strokeWidth=1))
d.add(String(10, 8, "MEDULLA (inner)", fontSize=9, fontName="Helvetica-Bold", fillColor=TEAL))
# Descending limb (left column, water permeable)
dl_x = 120
d.add(Rect(dl_x, 10, 50, 195, fillColor=colors.HexColor("#aed6f1"),
strokeColor=TEAL, strokeWidth=1.5))
d.add(String(dl_x+25, 205, "DESC.", fontSize=8, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=TEAL))
d.add(String(dl_x+25, 195, "LIMB", fontSize=8, textAnchor="middle", fillColor=TEAL))
# osmolarity values descending
osm_vals = [(190, "300"), (160, "600"), (130, "900"), (100, "1200"), (70, "1200")]
for (y, val) in osm_vals:
d.add(String(dl_x+25, y, val, fontSize=8, textAnchor="middle", fillColor=NAVY))
# Ascending limb (right column, impermeable to water)
al_x = 200
d.add(Rect(al_x, 10, 50, 195, fillColor=colors.HexColor("#a9dfbf"),
strokeColor=GREEN, strokeWidth=1.5))
d.add(String(al_x+25, 205, "ASC.", fontSize=8, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=GREEN))
d.add(String(al_x+25, 195, "LIMB", fontSize=8, textAnchor="middle", fillColor=GREEN))
osm_asc = [(185, "100"), (158, "300"), (128, "600"), (98, "900"), (68, "1200")]
for (y, val) in osm_asc:
d.add(String(al_x+25, y, val, fontSize=8, textAnchor="middle", fillColor=DARK))
d.add(String(al_x+25, 45, "Active NaCl", fontSize=7, textAnchor="middle", fillColor=GREEN))
d.add(String(al_x+25, 35, "pump (NKCC2)", fontSize=7, textAnchor="middle", fillColor=GREEN))
d.add(String(al_x+25, 25, "NO water", fontSize=7, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=RED))
# Collecting duct
cd_x = 300
d.add(Rect(cd_x, 10, 50, 195, fillColor=colors.HexColor("#f9ebea"),
strokeColor=RED, strokeWidth=1.5))
d.add(String(cd_x+25, 205, "COLL.", fontSize=8, textAnchor="middle",
fontName="Helvetica-Bold", fillColor=RED))
d.add(String(cd_x+25, 195, "DUCT", fontSize=8, textAnchor="middle", fillColor=RED))
for (y, val) in [(185,"1200"),(130,"ADH→"), (110,"water"), (90,"leaves")]:
d.add(String(cd_x+25, y, val, fontSize=8, textAnchor="middle", fillColor=RED))
# Medullary gradient arrow
d.add(String(400, 190, "300", fontSize=9, fillColor=NAVY, fontName="Helvetica-Bold"))
d.add(String(400, 100, "900", fontSize=9, fillColor=NAVY, fontName="Helvetica-Bold"))
d.add(String(400, 20, "1200", fontSize=9, fillColor=NAVY, fontName="Helvetica-Bold"))
d.add(Line(420, 185, 420, 25, strokeColor=NAVY, strokeWidth=2))
d.add(Polygon([416,25, 424,25, 420,15], fillColor=NAVY, strokeColor=NAVY))
d.add(String(435, 100, "mOsm/L\ngradient", fontSize=8, fillColor=NAVY))
return d
def raas_diagram():
"""RAAS cascade"""
d = Drawing(480, 200)
d.add(String(240, 190, "Renin-Angiotensin-Aldosterone System (RAAS)",
fontSize=10, textAnchor="middle", fontName="Helvetica-Bold", fillColor=NAVY))
steps = [
("Low BP / Low Na+\nSymp. activity", 20, 130, TEAL),
("RENIN\n(JG cells)", 110, 130, NAVY),
("Angiotensin I", 200, 130, GRAY),
("Angiotensin II\n(ACE, lung)", 290, 130, ORANGE),
("ALDOSTERONE\n(adrenal cortex)", 380, 130, RED),
]
for i, (label, x, y, col) in enumerate(steps):
lines = label.split("\n")
box_h = 12 * len(lines) + 14
d.add(Rect(x, y - box_h//2, 82, box_h,
fillColor=col, strokeColor=WHITE, strokeWidth=1, rx=4, ry=4))
for j, ln in enumerate(lines):
d.add(String(x+41, y + (len(lines)-1)*6 - j*12,
ln, fontSize=7.5, textAnchor="middle",
fillColor=WHITE, fontName="Helvetica-Bold"))
if i < len(steps)-1:
d.add(Line(x+84, y, x+92, y, strokeColor=GRAY, strokeWidth=1.5))
d.add(Polygon([x+90, y+3, x+90, y-3, x+96, y],
fillColor=GRAY, strokeColor=GRAY))
# Effects of Ang II and Aldosterone
d.add(Rect(200, 30, 170, 60, fillColor=LIGHT_GREEN, strokeColor=GREEN, strokeWidth=1, rx=4))
effects = ["Na+ reabsorption (PCT, CD)",
"K+ secretion (CD)",
"Blood volume & BP"]
d.add(String(285, 87, "NET EFFECTS:", fontSize=8,
textAnchor="middle", fontName="Helvetica-Bold", fillColor=GREEN))
for i, e in enumerate(effects):
d.add(String(285, 75 - i*11, f"+ {e}", fontSize=7.5,
textAnchor="middle", fillColor=DARK))
return d
# ─────────────────────────────────────────────────────────
# Build PDF content
# ─────────────────────────────────────────────────────────
story = []
# ══════════════════════ COVER PAGE ══════════════════════
story.append(spacer(2))
# Coloured banner
banner = Table([[Paragraph("<font color='white'><b>RENAL PHYSIOLOGY</b></font>",
ParagraphStyle("bn", fontSize=30, alignment=TA_CENTER, leading=36))]],
colWidths=[PAGE_W - 2*MARGIN])
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("TOPPADDING", (0,0), (-1,-1), 22),
("BOTTOMPADDING", (0,0), (-1,-1), 22),
("ROUNDEDCORNERS", [8]),
]))
story.append(banner)
story.append(spacer(0.4))
story.append(Paragraph("Comprehensive Study Guide", ST_SUBTITLE))
story.append(Paragraph("Based on Guyton & Hall | Ganong's | Costanzo Physiology", ST_SUBTITLE))
story.append(spacer(0.6))
toc_items = [
("1", "Functional Anatomy of the Nephron"),
("2", "Glomerular Filtration & GFR"),
("3", "Tubular Reabsorption & Secretion"),
("4", "Loop of Henle & Countercurrent Mechanism"),
("5", "Urine Concentration & Dilution (ADH)"),
("6", "Hormonal Regulation (RAAS, ANP, PTH)"),
("7", "Renal Handling of Key Substances"),
("8", "Acid–Base Balance"),
("9", "Renal Clearance"),
("10", "Quick-Reference Tables & Key Values"),
]
toc_data = [[Paragraph(f"<b>{n}.</b> {t}", ST_BODY)] for n, t in toc_items]
toc_table = Table(toc_data, colWidths=[PAGE_W - 2*MARGIN])
toc_table.setStyle(TableStyle([
("ROWBACKGROUNDS", (0,0), (-1,-1), [WHITE, LIGHT_BLUE]),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 14),
("BOX", (0,0), (-1,-1), 1, TEAL),
]))
story.append(Paragraph("<b>Contents</b>", ST_H2))
story.append(toc_table)
story.append(spacer(1))
source_box = Table([[Paragraph(
"<b>Primary Sources:</b> Guyton & Hall Textbook of Medical Physiology 14E • "
"Ganong's Review of Medical Physiology 26E • Costanzo Physiology 7E • "
"Brenner & Rector's The Kidney",
ParagraphStyle("src", fontSize=8.5, textColor=GRAY, alignment=TA_CENTER)
)]], colWidths=[PAGE_W - 2*MARGIN])
source_box.setStyle(TableStyle([
("BOX", (0,0), (-1,-1), 0.5, GRAY),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
]))
story.append(source_box)
story.append(PageBreak())
# ══════════════════════ SECTION 1: ANATOMY ══════════════════════
story.append(section_header("1. Functional Anatomy of the Nephron", NAVY, ""))
story.append(spacer(0.3))
story.append(body(
"Each kidney contains approximately <b>1 million nephrons</b>. The nephron is the "
"functional unit of the kidney. Each nephron consists of a renal corpuscle (glomerulus + "
"Bowman's capsule) and a renal tubule. The tubule drains sequentially through the "
"proximal convoluted tubule (PCT), loop of Henle, distal convoluted tubule (DCT), and "
"collecting duct system."
))
story.append(spacer(0.2))
story.append(sub_header("Types of Nephrons"))
story.append(make_table(
["Type", "Location", "Loop of Henle", "Key Role"],
[
["Cortical nephrons (~75%)",
"Outer cortex", "Short; barely enters medulla",
"General filtration; isoosmotic reabsorption"],
["Juxtamedullary nephrons (~25%)",
"Near corticomedullary junction", "Long; extends deep into medulla",
"Urine concentration via countercurrent mechanism"],
],
col_widths=[3.5*cm, 3.5*cm, 5*cm, 5.5*cm]
))
story.append(spacer(0.3))
story.append(sub_header("Blood Supply – The Two-Capillary-Bed System"))
story.append(body(
"Renal artery → interlobar arteries → arcuate arteries → interlobular arteries → "
"<b>afferent arteriole</b> → <b>glomerular capillaries</b> (high-pressure, filtration) → "
"<b>efferent arteriole</b> → <b>peritubular capillaries / vasa recta</b> (low-pressure, "
"reabsorption) → renal vein."
))
story.append(info_box("Why Two Capillary Beds Matter", [
"Glomerular capillaries: high hydrostatic pressure (~60 mmHg) drives filtration",
"Efferent arteriole resistance: fine-tunes GFR and peritubular reabsorption",
"Peritubular capillaries: low pressure + high oncotic pressure drives reabsorption",
"Vasa recta: countercurrent exchanger preserving medullary osmotic gradient",
], bg=LIGHT_BLUE, border=TEAL))
story.append(spacer(0.3))
story.append(sub_header("Nephron Flow Diagram"))
story.append(nephron_flow_diagram())
story.append(Paragraph(
"Fig 1. Simplified nephron segments with approximate tubular fluid osmolarity at each stage",
ST_CAPTION
))
story.append(PageBreak())
# ══════════════════════ SECTION 2: GFR ══════════════════════
story.append(section_header("2. Glomerular Filtration & GFR", TEAL, ""))
story.append(spacer(0.2))
story.append(key_point("Normal GFR = 125 mL/min = 180 L/day filtered. Only ~1.5 L excreted as urine – >99% reabsorbed!"))
story.append(spacer(0.2))
story.append(sub_header("The Filtration Barrier"))
story.append(body(
"The glomerular filtration barrier has three layers: <b>(1)</b> fenestrated capillary "
"endothelium (prevents cells), <b>(2)</b> glomerular basement membrane (GBM, blocks large "
"proteins), <b>(3)</b> podocytes with slit diaphragms (prevents albumin). Substances "
"freely filtered: electrolytes, glucose, urea, creatinine, amino acids. Proteins and "
"protein-bound molecules are retained."
))
story.append(spacer(0.2))
story.append(sub_header("Starling Forces – Net Filtration Pressure"))
story.append(starling_forces_diagram())
story.append(Paragraph("Fig 2. Starling forces governing net glomerular filtration pressure (~10 mmHg)", ST_CAPTION))
story.append(spacer(0.2))
story.append(make_table(
["Force", "Value", "Direction", "Altered by"],
[
["Glomerular capillary hydrostatic pressure (Pgc)", "~60 mmHg",
"Promotes filtration", "Afferent/efferent arteriole tone, BP"],
["Bowman's capsule hydrostatic pressure (Pbs)", "~18 mmHg",
"Opposes filtration", "Urinary obstruction, ureteral stones"],
["Glomerular oncotic pressure (pgc)", "~32 mmHg",
"Opposes filtration", "Plasma protein levels, filtration fraction"],
["Net filtration pressure", "~10 mmHg",
"Promotes filtration", "Sum of above"],
["GFR = Kf x NFP", "~125 mL/min",
"—", "Kf reduced in glomerular disease"],
],
col_widths=[5.5*cm, 2.5*cm, 3.5*cm, 5*cm]
))
story.append(formula("GFR = Kf × (Pgc – Pbs – πgc) = Kf × ~10 mmHg = ~125 mL/min"))
story.append(spacer(0.2))
story.append(sub_header("Renal Autoregulation (MAP 80–180 mmHg)"))
story.append(make_table(
["Mechanism", "Trigger", "Response"],
[
["Myogenic", "Stretch of afferent arteriole wall from ↑BP",
"Vasoconstriction of afferent arteriole → maintains GFR"],
["Tubuloglomerular feedback (TGF)", "Macula densa senses ↑NaCl delivery to DCT",
"ATP/adenosine → afferent arteriolar constriction → ↓GFR"],
],
col_widths=[4*cm, 6*cm, 6.5*cm]
))
story.append(spacer(0.2))
story.append(sub_header("Factors Altering GFR"))
story.append(make_table(
["Increases GFR", "Decreases GFR"],
[
["Afferent arteriole dilation (prostaglandins, ANP)",
"Afferent arteriole constriction (sympathetic NS, Ang II high dose)"],
["↑ Blood pressure (within autoregulation)",
"Efferent arteriole dilation (ACE inhibitors → ↓ efferent resistance)"],
["↓ Plasma oncotic pressure",
"↑ Bowman's capsule pressure (obstruction)"],
["Efferent arteriole constriction (low-dose Ang II)",
"↓ Kf (glomerulonephritis, diabetic nephropathy)"],
],
col_widths=[8*cm, 8.5*cm]
))
story.append(PageBreak())
# ══════════════════════ SECTION 3: TUBULAR FUNCTION ══════════════════════
story.append(section_header("3. Tubular Reabsorption & Secretion", GREEN, ""))
story.append(spacer(0.2))
story.append(formula("Urinary Excretion = Glomerular Filtration − Reabsorption + Secretion"))
story.append(spacer(0.2))
story.append(sub_header("Proximal Convoluted Tubule (PCT)"))
story.append(info_box("PCT Reabsorbs ~65–70% of Filtered Load", [
"Na+, Cl-, K+, HCO3-, water (all ~65-70%)",
"Glucose: ~100% (via SGLT1/SGLT2 cotransporters with Na+)",
"Amino acids: ~100% (via Na+-amino acid cotransporters)",
"Urea: ~50% (passive diffusion)",
"Reabsorption is ISOSMOTIC – fluid remains ~300 mOsm/L throughout PCT",
], bg=LIGHT_GREEN, border=GREEN))
story.append(spacer(0.2))
story.append(body(
"<b>Mechanism:</b> Basolateral Na+/K+-ATPase pumps 3 Na+ out and 2 K+ in, maintaining "
"low intracellular Na+. This gradient drives Na+ entry from lumen via: "
"(1) Na+-glucose cotransporter (SGLT2) – site of SGLT2 inhibitor action; "
"(2) Na+/H+ antiporter – couples Na+ entry with H+ secretion, reclaiming HCO3-; "
"(3) Na+-amino acid cotransporters. Water follows Na+ via AQP1 channels (always open)."
))
story.append(spacer(0.2))
story.append(key_point("Glucose Tm: Transport maximum ~375 mg/min. Renal threshold ~180 mg/dL plasma glucose → glucosuria in diabetes."))
story.append(spacer(0.2))
story.append(sub_header("Loop of Henle"))
story.append(make_table(
["Segment", "Na+/Solute Transport", "Water Permeability", "Net Effect on Fluid"],
[
["Thin descending limb", "No active transport; some Na+ entry",
"High (AQP1 present)", "Water leaves; fluid becomes HYPERTONIC (up to 1200 mOsm)"],
["Thin ascending limb", "Passive NaCl diffusion out",
"Impermeable", "Solute out, no water – slight dilution"],
["THICK ascending limb (TAL)", "Active Na+/K+/2Cl- cotransport (NKCC2) – FUROSEMIDE site",
"IMPERMEABLE (no AQP)", "Fluid dilutes to ~100 mOsm (DILUTING SEGMENT)"],
],
col_widths=[3.5*cm, 5*cm, 3.5*cm, 5*cm]
))
story.append(spacer(0.2))
story.append(sub_header("Distal Convoluted Tubule (DCT)"))
story.append(body(
"Reabsorbs Na+ and Cl- via the <b>NaCl cotransporter (NCC)</b> on the apical membrane – "
"this is the site of action of <b>thiazide diuretics</b>. The DCT is water-impermeable "
"in its early portion, continuing the dilution of tubular fluid. Late DCT responds to "
"aldosterone. Fluid enters DCT at ~100 mOsm/L."
))
story.append(spacer(0.2))
story.append(sub_header("Collecting Duct – Final Fine-Tuning"))
story.append(make_table(
["Cell Type", "Apical Transporter", "Hormone", "Function"],
[
["Principal cell", "ENaC (Na+ in), ROMK (K+ out), AQP2 (water)",
"Aldosterone (Na+); ADH (water)", "Na+ reabsorption, K+ secretion, water reabsorption"],
["Alpha-intercalated cell", "H+-ATPase (H+ out), Cl-/HCO3- exchanger",
"Acidosis stimulates", "H+ secretion; acid-base regulation"],
["Beta-intercalated cell", "Cl-/HCO3- exchanger (apical)",
"Alkalosis stimulates", "HCO3- secretion; acid-base regulation"],
],
col_widths=[3.5*cm, 5.5*cm, 3.5*cm, 4*cm]
))
story.append(PageBreak())
# ══════════════════════ SECTION 4: COUNTERCURRENT ══════════════════════
story.append(section_header("4. Loop of Henle & Countercurrent Mechanism", ORANGE, ""))
story.append(spacer(0.2))
story.append(body(
"The countercurrent system creates and maintains a <b>hyperosmotic renal medullary "
"interstitium</b> (up to 1200–1400 mOsm/L at the papillary tip vs. 300 mOsm/L in the "
"cortex). This gradient is the essential prerequisite for producing concentrated urine."
))
story.append(spacer(0.3))
story.append(countercurrent_diagram())
story.append(Paragraph(
"Fig 3. Countercurrent multiplier showing osmolarity values (mOsm/L) in each tubular segment",
ST_CAPTION
))
story.append(spacer(0.2))
story.append(sub_header("How the Gradient is Built – Four Factors"))
story.append(make_table(
["Factor", "Mechanism", "Contribution"],
[
["NKCC2 pump in thick ALH",
"Active Na+/K+/2Cl- transport out of the thick ascending limb (impermeable to water)",
"Primary driver – adds solute without water to medulla"],
["Urea recycling",
"Inner medullary collecting duct (with ADH) reabsorbs urea via UT-A1/UT-A3 transporters",
"Adds ~500 mOsm to inner medulla"],
["Thin descending limb",
"Water exits down osmotic gradient into hypertonic interstitium via AQP1",
"Concentrates tubular fluid delivered to bend"],
["Vasa recta (countercurrent exchanger)",
"Descending vasa recta takes up solute; ascending loses it back – hairpin arrangement",
"Prevents washout of medullary gradient"],
],
col_widths=[3.5*cm, 7*cm, 6*cm]
))
story.append(spacer(0.3))
story.append(info_box("Clinical Pearl", [
"Loop diuretics (furosemide, bumetanide) block NKCC2 in the thick ALH",
"This destroys the medullary concentration gradient",
"Collecting duct cannot concentrate urine even with maximal ADH → massive diuresis",
"Also causes K+ wasting (reduces K+ recycling in TAL driving ROMK secretion)",
], bg=LIGHT_RED, border=RED))
story.append(PageBreak())
# ══════════════════════ SECTION 5: ADH / CONCENTRATION ══════════════════════
story.append(section_header("5. Urine Concentration & Dilution (ADH)", PURPLE, ""))
story.append(spacer(0.2))
story.append(sub_header("ADH (Vasopressin) Mechanism"))
story.append(body(
"ADH is produced in the <b>supraoptic and paraventricular nuclei of the hypothalamus</b> "
"and released from the posterior pituitary. It acts via V2 receptors on collecting duct "
"principal cells → activates adenylyl cyclase → ↑cAMP → PKA → phosphorylation of "
"AQP2 vesicles → insertion of <b>aquaporin-2 (AQP2)</b> into the apical membrane → "
"collecting duct becomes water-permeable → water moves out into hypertonic medulla."
))
story.append(spacer(0.2))
story.append(make_table(
["Condition", "ADH Level", "Collecting Duct", "Urine Osmolarity", "Urine Volume"],
[
["Dehydration / ↑plasma osmolarity", "HIGH", "Permeable (AQP2 inserted)",
"Up to 1200–1400 mOsm/L", "Low (~500 mL/day)"],
["Overhydration / ↓plasma osmolarity", "LOW", "Impermeable (AQP2 absent)",
"As low as 50–100 mOsm/L", "High (up to 20 L/day)"],
],
col_widths=[4.5*cm, 2*cm, 4*cm, 4*cm, 3*cm]
))
story.append(spacer(0.2))
story.append(sub_header("Stimuli for ADH Release"))
story.append(make_table(
["Stimulus", "Sensor", "Effect"],
[
["↑ Plasma osmolarity (>280 mOsm)", "Osmoreceptors in anterior hypothalamus",
"Primary regulator – even 1–2% change triggers ADH"],
["↓ Blood volume/pressure", "Baroreceptors (carotid, atria)",
"Requires >8–10% volume loss; more potent override"],
["Nausea, pain, stress", "CNS", "Stimulate ADH even at normal osmolarity"],
["Alcohol", "Hypothalamus", "INHIBITS ADH → diuresis (hence frequent urination with alcohol)"],
],
col_widths=[5*cm, 5*cm, 6.5*cm]
))
story.append(spacer(0.2))
story.append(info_box("Diabetes Insipidus (DI) – Key Distinction", [
"Central DI: ADH not produced/released (hypothalamic/pituitary damage) → massive hypotonic polyuria",
"Nephrogenic DI: ADH present but collecting duct V2 receptors/AQP2 dysfunctional",
"SIADH: Excess ADH → water retention → dilutional hyponatremia → concentrated urine",
"Desmopressin (synthetic ADH) treats Central DI; corrects urine in CDI but not nephrogenic DI",
], bg=LIGHT_PURPLE, border=PURPLE))
story.append(PageBreak())
# ══════════════════════ SECTION 6: HORMONES ══════════════════════
story.append(section_header("6. Hormonal Regulation of Renal Function", RED, ""))
story.append(spacer(0.2))
story.append(sub_header("Renin-Angiotensin-Aldosterone System (RAAS)"))
story.append(raas_diagram())
story.append(Paragraph("Fig 4. RAAS cascade from renin release to aldosterone effects", ST_CAPTION))
story.append(spacer(0.2))
story.append(make_table(
["Step", "Location", "What Happens"],
[
["Renin release", "JG cells of afferent arteriole",
"Triggered by: ↓ BP (stretch), ↓ NaCl at macula densa, ↑ sympathetic (beta-1)"],
["Angiotensinogen → Ang I", "Liver (angiotensinogen) + plasma",
"Renin cleaves angiotensinogen to Ang I (inactive decapeptide)"],
["Ang I → Ang II", "Lung endothelium (ACE)",
"ACE converts Ang I to Ang II (active octapeptide). ACE inhibitors block here"],
["Ang II effects", "Multiple organs",
"(1) PCT: ↑ Na+/H+ antiporter → ↑ Na+ reabsorption; (2) Adrenal: → aldosterone; "
"(3) Vasoconstriction; (4) ↑ ADH; (5) Thirst"],
["Aldosterone", "Collecting duct principal cells",
"↑ ENaC and Na+/K+-ATPase → ↑ Na+ reabsorption, ↑ K+ secretion, water follows → ↑ BP"],
],
col_widths=[3.5*cm, 4*cm, 9*cm]
))
story.append(spacer(0.2))
story.append(sub_header("Other Key Hormones"))
story.append(make_table(
["Hormone", "Source", "Renal Action", "Net Effect"],
[
["ANP (Atrial Natriuretic Peptide)", "Atria (↑stretch)",
"Dilates afferent, constricts efferent → ↑GFR; ↓ renin; ↓ aldosterone; ↓ ADH",
"Natriuresis + diuresis → ↓ blood volume"],
["PTH (Parathyroid Hormone)", "Parathyroid glands",
"↑ Ca2+ reabsorption (DCT); ↓ phosphate reabsorption (PCT); "
"activates 1α-hydroxylase → active Vit D",
"↑ serum Ca2+, ↓ serum phosphate"],
["Dopamine", "Proximal tubule cells",
"↓ Na+/K+-ATPase and NHE3 in PCT; ↓ aldosterone",
"Natriuresis; used in low doses for renal protection"],
["Prostaglandins (PGE2)", "Renal medulla",
"Dilate afferent arteriole → maintain GFR; antagonize ADH in collecting duct",
"NSAIDs block → ↓ GFR, water retention"],
],
col_widths=[3.5*cm, 3.5*cm, 6.5*cm, 3*cm]
))
story.append(PageBreak())
# ══════════════════════ SECTION 7: SPECIFIC SUBSTANCES ══════════════════════
story.append(section_header("7. Renal Handling of Key Substances", NAVY, ""))
story.append(spacer(0.2))
story.append(make_table(
["Substance", "Filtered?", "PCT", "Loop of Henle", "DCT / CD", "Net Excretion"],
[
["Sodium (Na+)", "Yes", "65-70% reabsorbed (Na+/K+-ATPase, NHE3, SGLT)",
"25% TAL (NKCC2)", "~5% (aldosterone-regulated ENaC)", "<1%"],
["Glucose", "Yes", "~100% (SGLT1/2, Tm-limited)",
"–", "–", "0 (unless >Tm)"],
["Potassium (K+)", "Yes", "65% reabsorbed",
"25% reabsorbed (TAL via ROMK recycling)", "Secreted by principal cells (aldosterone)",
"Variable; ~15% normally"],
["Urea", "Yes", "~50% reabsorbed (passive)",
"Secreted (thin ALH)", "Reabsorbed (inner MCD, UT-A1 with ADH)", "~50%"],
["Creatinine", "Yes", "Minimal reabsorption",
"–", "Small secretion", "~100% of filtered"],
["Bicarbonate (HCO3-)", "Yes", "80-90% reabsorbed (NHE3 + carbonic anhydrase)",
"~5% TAL", "Final titration (intercalated cells)", "Very little (normal pH)"],
["Calcium (Ca2+)", "Yes (40% free)", "65% passive paracellular",
"25% (TAL – paracellular, driven by lumen +ve potential)",
"Active transcellular (PTH-stimulated)", "<2%"],
["Phosphate", "Yes", "85% reabsorbed (NaPi-IIa cotransporter – inhibited by PTH)",
"–", "–", "15% normally"],
["Uric acid", "Yes", "Reabsorbed AND secreted (net reabsorption 90%)",
"–", "–", "~10%"],
["H+ (acid)", "–", "Secreted (NHE3 → reclaims HCO3-)",
"–", "Secreted (H+-ATPase in intercalated cells)", "~80 mEq/day"],
],
col_widths=[2.8*cm, 1.5*cm, 4.2*cm, 3*cm, 3.5*cm, 2.5*cm]
))
story.append(PageBreak())
# ══════════════════════ SECTION 8: ACID-BASE ══════════════════════
story.append(section_header("8. Renal Acid–Base Balance", colors.HexColor("#6c3483"), ""))
story.append(spacer(0.2))
story.append(body(
"The kidneys are the <b>long-term</b> regulators of body pH (lungs handle short-term CO2). "
"Normal arterial pH = 7.35–7.45. The kidneys excrete ~80 mEq of fixed acid per day "
"through three mechanisms:"
))
story.append(spacer(0.2))
story.append(make_table(
["Mechanism", "Where", "How It Works", "Significance"],
[
["HCO3- Reabsorption", "PCT (~85%), TAL (~5%), CD",
"H+ secreted via NHE3 (PCT) reacts with filtered HCO3-; "
"carbonic anhydrase: H2CO3 → CO2+H2O; CO2 enters cell → reforms HCO3- → "
"exits basolaterally. NET: reclaims filtered bicarbonate",
"Not true acid excretion; reclaims bicarbonate buffer"],
["Titratable Acid (TA)", "Collecting duct",
"H+ secreted by H+-ATPase combines with HPO4(2-) → H2PO4(-), "
"which is excreted. Each H+ excreted regenerates 1 HCO3-",
"~30-40 mEq/day; limited by phosphate availability"],
["Ammonium (NH4+)", "PCT generates NH3; CD secretes into lumen",
"Glutamine → glutaminase → NH3 + H+ → NH4+ (trapped in lumen). "
"Medullary recycling amplifies delivery to collecting duct",
"~40-50 mEq/day; upregulated in chronic acidosis; most important buffer"],
],
col_widths=[3.5*cm, 2.5*cm, 7*cm, 3.5*cm]
))
story.append(spacer(0.2))
story.append(sub_header("Renal Compensation for Acid-Base Disorders"))
story.append(make_table(
["Disorder", "Primary Change", "Renal Compensation", "Time Course"],
[
["Metabolic Acidosis", "↓ HCO3-", "↑ H+ secretion; ↑ NH4+ production; ↑ HCO3- generation",
"Hours to days"],
["Metabolic Alkalosis", "↑ HCO3-", "↓ H+ secretion; ↑ HCO3- excretion (bicarbonaturia)",
"Hours to days"],
["Respiratory Acidosis", "↑ PaCO2", "↑ H+ secretion; ↑ NH4+; ↑ HCO3- reabsorption",
"2-5 days"],
["Respiratory Alkalosis", "↓ PaCO2", "↓ H+ secretion; ↑ HCO3- excretion",
"2-5 days"],
],
col_widths=[4*cm, 3*cm, 6.5*cm, 3*cm]
))
story.append(PageBreak())
# ══════════════════════ SECTION 9: CLEARANCE ══════════════════════
story.append(section_header("9. Renal Clearance", GREEN, ""))
story.append(spacer(0.2))
story.append(formula("Clearance (C) = (Urine concentration × Urine flow rate) ÷ Plasma concentration = U×V / P"))
story.append(body(
"<b>Clearance</b> represents the volume of plasma completely cleared of a substance per unit time. "
"Comparing a substance's clearance to inulin clearance (= GFR) reveals whether it is "
"reabsorbed, secreted, or neither."
))
story.append(spacer(0.2))
story.append(make_table(
["Substance", "Clearance (mL/min)", "Interpretation"],
[
["Glucose", "0", "Fully reabsorbed below Tm"],
["Sodium", "~0.9", "Mostly reabsorbed; <1% excreted"],
["Urea", "~70", "Partly reabsorbed (clearance < GFR)"],
["Inulin", "125", "= GFR (gold standard – filtered only, not absorbed/secreted)"],
["Creatinine", "~140", "Slightly > GFR (some tubular secretion)"],
["PAH", "~650", "= Renal Plasma Flow (RPF) – nearly fully secreted"],
],
col_widths=[4*cm, 4*cm, 8.5*cm]
))
story.append(spacer(0.2))
story.append(make_table(
["Derived Value", "Formula", "Normal Value"],
[
["GFR", "Inulin clearance = Uin×V / Pin", "~125 mL/min"],
["Renal Plasma Flow (RPF)", "PAH clearance = UPAH×V / PPAH", "~650 mL/min"],
["Renal Blood Flow (RBF)", "RPF / (1 - Hematocrit)", "~1200 mL/min (~20% cardiac output)"],
["Filtration Fraction (FF)", "GFR / RPF", "~0.19 (19%)"],
],
col_widths=[4.5*cm, 6.5*cm, 5.5*cm]
))
story.append(spacer(0.2))
story.append(info_box("Creatinine Clearance – Clinical Use", [
"Endogenous creatinine clearance ~140 mL/min (slight overestimate of GFR due to tubular secretion)",
"Cockcroft-Gault formula: CrCl = [(140 - age) x weight(kg)] / [72 x serum Cr(mg/dL)] (x 0.85 for females)",
"eGFR by CKD-EPI equation now preferred in clinical practice",
"CKD staging: G1 (>90), G2 (60-89), G3a (45-59), G3b (30-44), G4 (15-29), G5 (<15 mL/min/1.73m2)",
], bg=LIGHT_GREEN, border=GREEN))
story.append(PageBreak())
# ══════════════════════ SECTION 10: QUICK REFERENCE ══════════════════════
story.append(section_header("10. Quick-Reference Tables & Key Values", GOLD, ""))
story.append(spacer(0.2))
story.append(sub_header("Normal Renal Parameters"))
story.append(make_table(
["Parameter", "Normal Value"],
[
["GFR", "125 mL/min (180 L/day)"],
["Renal Plasma Flow (RPF)", "~650 mL/min"],
["Renal Blood Flow (RBF)", "~1200 mL/min (20-25% cardiac output)"],
["Filtration Fraction", "~19%"],
["Daily urine output", "1-2 L/day"],
["Urine osmolarity range", "50-1400 mOsm/L"],
["Plasma osmolarity", "275-295 mOsm/L"],
["Maximum urine concentration", "~1200-1400 mOsm/L (medullary tip)"],
["Normal serum creatinine", "0.6-1.2 mg/dL (men); 0.5-1.1 (women)"],
["Normal GFR threshold for glucosuria", "Plasma glucose >180-200 mg/dL"],
],
col_widths=[8*cm, 8.5*cm]
))
story.append(spacer(0.2))
story.append(sub_header("Diuretic Sites of Action"))
story.append(make_table(
["Diuretic Class", "Site", "Transporter Blocked", "Key Effects"],
[
["Carbonic anhydrase inhibitors\n(Acetazolamide)",
"PCT",
"Carbonic anhydrase → ↓ H+ secretion → ↓ HCO3- reclamation",
"Bicarbonaturia; metabolic acidosis; weak diuresis"],
["Osmotic diuretics\n(Mannitol)",
"PCT + Descending LOH",
"Not a transporter; limits passive water reabsorption",
"↑ urine volume; reduces cerebral edema"],
["Loop diuretics\n(Furosemide, Bumetanide)",
"Thick ascending LOH",
"NKCC2 (Na+/K+/2Cl-)",
"Most potent; destroys medullary gradient; Ca2+ and Mg2+ wasting; K+ wasting"],
["Thiazides\n(Hydrochlorothiazide)",
"Early DCT",
"NCC (Na+/Cl-)",
"Moderate diuresis; K+ wasting; Ca2+ RETENTION (useful in hypercalciuria/stones)"],
["K+-sparing diuretics\n(Spironolactone, Amiloride)",
"Collecting duct",
"Spiro: blocks aldosterone receptor; Amiloride: blocks ENaC",
"Weak diuresis; hyperkalemia risk; no K+ wasting"],
["V2 receptor antagonists\n(Tolvaptan – 'Vaptans')",
"Collecting duct",
"V2 receptor → blocks AQP2 insertion",
"Aquaresis (free water excretion); treats hyponatremia in SIADH/CHF"],
],
col_widths=[3.5*cm, 2.5*cm, 4.5*cm, 6*cm]
))
story.append(spacer(0.2))
story.append(sub_header("Tubular Transport Mechanisms Summary"))
story.append(make_table(
["Transporter", "Location", "Moves", "Blocked By"],
[
["Na+/K+-ATPase", "Basolateral (all segments)", "3Na+ out, 2K+ in", "Ouabain (experimentally)"],
["SGLT2 / SGLT1", "PCT apical", "Na+ + Glucose cotransport", "Gliflozins (SGLT2i – empagliflozin etc.)"],
["NHE3 (Na+/H+ antiporter)", "PCT apical", "Na+ in, H+ out", "Carbonic anhydrase inhibitors (indirectly)"],
["NKCC2", "Thick ALH apical", "Na+, K+, 2Cl- in", "Loop diuretics (furosemide)"],
["NCC", "DCT apical", "Na+, Cl- in", "Thiazides"],
["ENaC", "Collecting duct apical", "Na+ in", "Amiloride, spironolactone (indirectly)"],
["AQP1", "PCT + descending LOH", "Water (constitutive)", "Not regulated"],
["AQP2", "Collecting duct apical", "Water (regulated)", "Blocked by absence of ADH; tolvaptan"],
["H+-ATPase", "Intercalated cells apical", "H+ secretion", "—"],
],
col_widths=[3.5*cm, 4*cm, 4.5*cm, 4.5*cm]
))
story.append(PageBreak())
# ══════════════════════ BACK PAGE: MNEMONICS & PEARLS ══════════════════════
story.append(section_header("Clinical Pearls & Mnemonics", colors.HexColor("#1a5276"), ""))
story.append(spacer(0.2))
pearls = [
("GFR Memory Aid",
["180 L/day filtered, ~1.5 L excreted = 99%+ reabsorption",
"125 mL/min = normal adult GFR (memorize this number)",
"Creatinine clearance slightly overestimates GFR (tubular secretion adds ~10%)"]),
("Thick ALH = The 'Diluting Segment'",
["Pumps NaCl OUT (NKCC2), water stays in (impermeable)",
"Fluid exits at ~100 mOsm – HYPOTONIC despite being in hypertonic medulla",
"This is why loop diuretics are the most powerful – they destroy the gradient"]),
("Aldosterone vs. ADH",
["Aldosterone: controls Na+ (and hence VOLUME). 'Aldo controls Amount'",
"ADH: controls water (and hence OSMOLARITY). 'ADH controls dilution/concentration'",
"Both act on collecting duct but are independently regulated"]),
("ACE Inhibitors / ARBs & GFR",
["Block Ang II → dilate efferent arteriole → ↓ GFR",
"Beneficial in proteinuria (↓ glomerular hypertension) but dangerous in renal artery stenosis",
"Serum creatinine may rise 10-20% initially – acceptable and even expected"]),
("Potassium Handling Mnemonic",
["PCT + LOH = Reabsorb K+",
"DCT/CD principal cells = Secrete K+ (under aldosterone)",
"↑ aldosterone → ↑ K+ loss → hypokalemia",
"K+-sparing diuretics (spiro, amiloride) prevent this loss"]),
("Starling Forces Memory: '60 opposes 50'",
["Promoting filtration: Pgc = 60 mmHg",
"Opposing: Pbs (18) + pgc (32) = 50 mmHg",
"Net = 60 - 50 = 10 mmHg promoting filtration"]),
]
for (title, pts) in pearls:
bg = LIGHT_BLUE if pearls.index((title,pts)) % 2 == 0 else LIGHT_GREEN
story.append(info_box(title, pts, bg=bg, border=TEAL))
story.append(spacer(0.2))
# Footer note
story.append(hr(GRAY))
story.append(Paragraph(
"<i>Study Guide compiled from Guyton & Hall Textbook of Medical Physiology 14E, "
"Ganong's Review of Medical Physiology 26E, Costanzo Physiology 7E, and "
"Brenner & Rector's The Kidney. For educational use only.</i>",
ST_CAPTION
))
# ─────────────────────────────────────────────────────────
# Build
# ─────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT}")
print(f"Size: {os.path.getsize(OUTPUT):,} bytes")
cd /home/daytona/workspace/renal-physiology-guide && python3 create_pdf.py 2>&1
~/renal-physiology-guide/create_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/renal-physiology-guide/create_pdf.py'
cd /home/daytona/workspace/renal-physiology-guide && python3 create_pdf.py 2>&1
python3 -c " from pypdf import PdfReader r = PdfReader('/home/daytona/workspace/…
Renal Physiology Study Guide
PDF Document · PDF
- Colour-coded contents with all 10 sections listed
- Nephron types (cortical vs. juxtamedullary), blood supply, two-capillary-bed system
- Nephron flow diagram with osmolarity values at each segment
- Starling forces diagram with actual values (Pgc, Pbs, πgc)
- Factors increasing/decreasing GFR table
- Renal autoregulation (myogenic + TGF)
- PCT (Na+/K+-ATPase, SGLT2, NHE3, glucose Tm concept)
- Loop of Henle segment-by-segment table
- DCT and collecting duct cell types (principal, intercalated)
- Countercurrent multiplier diagram with mOsm/L values
- How the gradient is built (4 factors including urea recycling)
- Loop diuretic clinical pearl box
- ADH mechanism (V2 → cAMP → AQP2)
- With/without ADH comparison table
- DI vs. SIADH info box
- RAAS cascade diagram (JG cells → renin → Ang I → Ang II → aldosterone)
- ANP, PTH, dopamine, prostaglandins table
- Full table: Na+, glucose, K+, urea, creatinine, HCO3-, Ca2+, phosphate, H+
- Three acid excretion mechanisms; renal compensation table
- Clearance formula; inulin/PAH/creatinine values; CKD staging
- Normal renal parameters; diuretic sites of action (6 classes); all key transporters
- 6 high-yield memory aids for exams