Why trendelenburg gait is seen in dddh
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough explanation of why Trendelenburg gait is seen in DDH (Developmental Dysplasia of the Hip):
Trendelenburg Gait in DDH - Mechanism
Normal Gait - What Should Happen
During normal walking, every step involves a single-leg stance phase where the entire body weight is supported on one leg. For the pelvis to remain level (or tilt slightly toward the swing leg side), the hip abductors - primarily the gluteus medius - must contract strongly on the stance side. This muscle acts like a stabilizing cable pulling the pelvis down on the raised side.
Why DDH Disrupts This Mechanism
In DDH, multiple structural abnormalities converge to impair abductor function:
1. Proximal and Lateral Migration of the Femoral Head
When the femoral head is dislocated or subluxed out of the acetabulum, it migrates proximally and laterally. This is the central problem. The gluteus medius originates on the ilium and inserts into the greater trochanter of the femur. When the femoral head rides up, the greater trochanter also moves proximally.
2. Loss of Abductor Lever Arm (Most Important Reason)
The abductor force depends not just on muscle strength, but on its moment arm - the perpendicular distance from the hip joint center to the line of action of the muscle. In DDH:
- The femoral head (fulcrum) is displaced superiorly out of its normal acetabular position
- The distance between the origin (ilium) and insertion (greater trochanter) shortens because both ends approximate each other
- The muscle works in a shortened, slackened position with a reduced mechanical advantage
- As Firestein & Kelley's Textbook of Rheumatology explains: in coxa valga and high dislocations, there is a "decreased moment arm (D) for hip abductor force" - meaning the abductors must generate far more force to produce the same stabilizing moment
3. Abductor Muscle Insufficiency
Because the muscle is now operating at a mechanically disadvantaged length, it cannot generate enough torque to hold the pelvis level. When the patient stands on the affected leg, the abductors fail and the pelvis drops toward the contralateral (unaffected) side - this is the positive Trendelenburg sign.
4. Bilateral Involvement = Waddling Gait
As confirmed by the Color Atlas of Human Anatomy: "When abductor function is impaired on both sides (as in congenital dislocation of the hip), the patient develops a waddling gait (bilateral positive Trendelenburg sign)." This is the classic presentation of bilateral DDH in a walking-age child.
The Clinical Picture in DDH
Per Campbell's Operative Orthopaedics 15th Ed:
"In a child of walking age with an undetected dislocated hip, families often describe a 'waddling' type of gait, indicating dislocation of the femoral head and a Trendelenburg gait pattern."
| Feature | Mechanism |
|---|---|
| Pelvis drops to opposite side | Abductors cannot stabilize pelvis in single-leg stance |
| Reduced lever arm | Femoral head displaced proximally - abductor muscle shortened |
| Compensated Trendelenburg | Patient leans trunk toward affected side to shift CoM toward hip axis, reducing required abductor force |
| Bilateral waddling | Both hips affected, pelvis drops alternately on each step |
Compensated vs. Uncompensated Trendelenburg
Many DDH patients adopt a compensatory strategy: they lean the trunk laterally toward the stance limb (gluteus medius lurch). This shifts the body's center of mass closer to the hip joint axis, reducing the external moment the abductors must overcome. It minimizes the visible pelvic dip but is still abnormal gait.
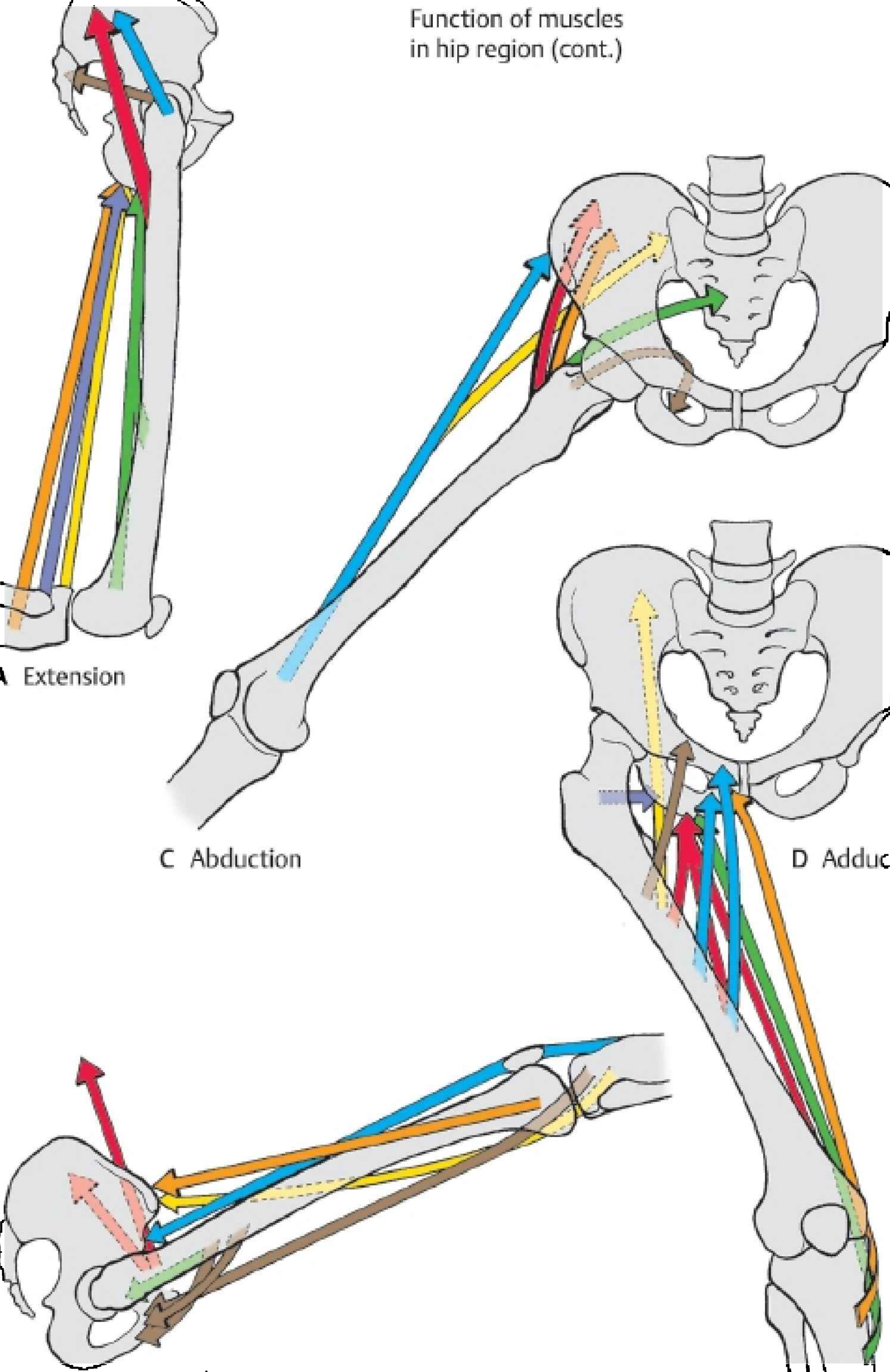
Diagram showing hip abductor muscle vectors - in DDH, proximal femoral head migration reduces the effective moment arm of these muscles.
Summary
Trendelenburg gait in DDH = dislocated femoral head → proximal migration of greater trochanter → shortened abductor muscle with reduced mechanical moment arm → gluteus medius insufficiency → pelvis cannot be stabilized in single-leg stance → pelvis drops to contralateral side on every step.
- Campbell's Operative Orthopaedics 15th Ed, p. 1404
- Color Atlas of Human Anatomy, p. 358-359
- Firestein & Kelley's Textbook of Rheumatology, p. 132
Wadlling gait in bilateral hip dislocation in ddh
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Here is a focused explanation of waddling gait in bilateral DDH:
Waddling Gait in Bilateral DDH
The Core Concept
Waddling gait is simply bilateral Trendelenburg gait happening alternately on each step. When both hips are dislocated, neither side can stabilize the pelvis - so the trunk lurches from side to side like a duck with every step.
Step-by-Step Mechanism
In unilateral DDH:
- Only one side has the dislocated hip and weak abductors
- Pelvis drops only to the normal side when standing on the affected leg
- Patient compensates by lurching the trunk toward the affected (dislocated) side to shift the center of mass - this is the Trendelenburg gait/lurch
In bilateral DDH - two things happen alternately:
| Step Phase | What Happens |
|---|---|
| Right leg stance | Left hip abductors fail (also dislocated) → pelvis sags to the left → trunk lurches RIGHT |
| Left leg stance | Right hip abductors fail (also dislocated) → pelvis sags to the right → trunk lurches LEFT |
| Result | Trunk swings right → left → right → left = waddling |
Why the Abductors Fail on BOTH Sides
In bilateral DDH, the same mechanism operates on each side:
- Both femoral heads are displaced proximally out of their acetabula
- The greater trochanter migrates upward on both sides, approximating toward the iliac origin of gluteus medius
- Both abductor muscles work in a shortened, mechanically disadvantaged position with reduced moment arm
- Neither can generate sufficient torque to hold the pelvis level in single-leg stance
As stated in S Das - A Manual on Clinical Surgery:
"The patient lurches on the affected side (Trendelenburg's gait) in unilateral congenital dislocation and coxa vara. This is to counteract the tendency of the pelvis to sink on the sound side when the leg of that side is raised off the ground. In bilateral congenital dislocation and bilateral coxa vara, the characteristic waddling gait is seen."
And from the Color Atlas of Human Anatomy:
"When abductor function is impaired on both sides (as in congenital dislocation of the hip), the patient develops a waddling gait (bilateral positive Trendelenburg sign)."
Why Compensation Fails in Bilateral DDH
In unilateral disease, the patient can lean toward the bad side to reduce abductor demand - the good side provides a stable base. In bilateral disease, there is no good side to lean on. As soon as the patient shifts weight to either leg, that hip's abductors also fail. The compensation cannot be sustained, producing the exaggerated side-to-side trunk swing of a true waddling gait.
Additional Features of Bilateral DDH Gait
- Hyperlordosis: Both femoral heads sit high → pelvis tilts forward → compensatory lumbar lordosis increases
- Perineal widening: Bilateral hip abduction contractures push the legs apart, widening the base of gait
- Short stride length: Both hips lack normal range, particularly extension
- Toe-out walking: External rotation deformity often present bilaterally
Summary Diagram
RIGHT step → Left abductors fail → Pelvis drops LEFT → Trunk lurches RIGHT
LEFT step → Right abductors fail → Pelvis drops RIGHT → Trunk lurches LEFT
↕ ↕
Continuous side-to-side trunk sway = WADDLING GAIT
The waddling gait in bilateral DDH is essentially two Trendelenburg gaits canceling each other's compensation - the result is a symmetrically abnormal, characteristic duck-like walk.
- S Das - A Manual on Clinical Surgery 13th Ed, p. 239
- Color Atlas of Human Anatomy, p. 358-359
This is a shared conversation. Sign in to Orris to start your own chat.