Behavioural observation audiometry is subjective or objective test
Reading File
Finding Sources
Finding Sources
Reading File
Behavioural Observation Audiometry (BOA) is a SUBJECTIVE test.
Here is a full breakdown:
Behavioural Observation Audiometry (BOA) - Subjective Test
Why It Is Subjective
BOA is classified as a subjective (behavioural) test because:
-
It relies on an observer's interpretation - the tester watches for changes in the child's behaviour (eye widening, eye blink, startle, altered sucking, arousal from sleep, limb movements) in response to a sound stimulus. There is no machine that objectively records a response.
-
No patient cooperation required - but the judgement of whether a response occurred rests entirely with the human observer (tester/distractor), making it inherently subjective.
-
Wide inter-tester variability - Scott-Brown's explicitly notes: "A wide variability in judgement of response between testers due to misinterpretation of random movements and a tendency to underestimate hearing thresholds has been demonstrated." - Scott-Brown's Otorhinolaryngology, Vol 2, p. 109
Contrast with Objective Tests
| Feature | BOA (Subjective) | Objective Tests (e.g., OAE, ABR/BERA) |
|---|---|---|
| Requires observer interpretation | Yes | No |
| Machine-recorded response | No | Yes |
| Patient cooperation needed | No (infant) | No |
| Bias possible | Yes (observer bias) | No |
| Age group | 0-6 months | Any age |
Key Details About BOA
- Developmental age: 0-6 months
- Responses observed: Eye widening, auropalpebral reflex (eye blink), startle, altered sucking, arousal from sleep, head turning (from 4-7 months)
- Stimuli used: Calibrated narrow-band warble tones, ling sounds, voice, or noisemakers; presented 15 cm from the ear, out of peripheral vision
- Reliability concern: Observer bias is a known limitation; video recording and blinded scoring have been tried to reduce this
- Current role: Largely superseded by electrophysiological techniques (ABR, OAE) for infants under 6 months, but BOA remains useful for:
- Verifying aided responses in infants
- Auditory neuropathy spectrum disorder (where ABR is unreliable)
- Older children with learning disabilities who cannot cooperate with other tests
Summary
BOA = Subjective test - it measures behavioural responses to sound and depends on observer interpretation, placing it firmly in the subjective audiometry category, alongside Visual Reinforcement Audiometry (VRA) and Pure Tone Audiometry (PTA).
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, Chapter 9
How does ABR (electrophysiological testing) differ from behavioral audiometry?
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough comparison of ABR vs behavioural audiometry, backed by textbook sources.
ABR (Electrophysiological) vs Behavioural Audiometry
The Core Distinction
| Feature | ABR / Electrophysiological | Behavioural Audiometry (BOA, VRA, PTA) |
|---|---|---|
| Test type | Objective | Subjective |
| What is measured | Electrical activity of auditory nerve & brainstem | Observed/voluntary behavioural response to sound |
| Patient cooperation | Not required | Required (or observer interpretation needed) |
| State of patient | Can be asleep, sedated, or under general anaesthesia | Must be awake and alert |
| Observer bias | None | Significant (especially in BOA) |
| Assesses full auditory system | No - only up to brainstem level | Yes - assesses the complete auditory system |
| Age suitability | Any age, including newborns | Varies (BOA: 0-6 months; VRA: 5-36 months; PTA: older children/adults) |
How ABR Works
Brainstem Auditory Evoked Potentials (BAEPs/ABR) are generated in the auditory nerve and brainstem after a brief acoustic stimulus (usually a sharp click). Surface electrodes placed on the scalp record the tiny electrical signals produced, which are only ~0.5 µV in amplitude. Because the signal is so faint, 1000-2000 responses must be averaged to resolve the waveform.
The normal ABR produces 5 waves (I-V) within the first 10 milliseconds, each corresponding to a different anatomical level:
| Wave | Anatomical Generator |
|---|---|
| I | Auditory nerve compound action potential (distal portion) |
| II | Proximal eighth nerve / cochlear nucleus |
| III | Lower pons - superior olive and trapezoid body |
| IV | Upper pons |
| V | Midbrain - up to the level of the inferior colliculus |
Here is what a normal ABR waveform looks like:
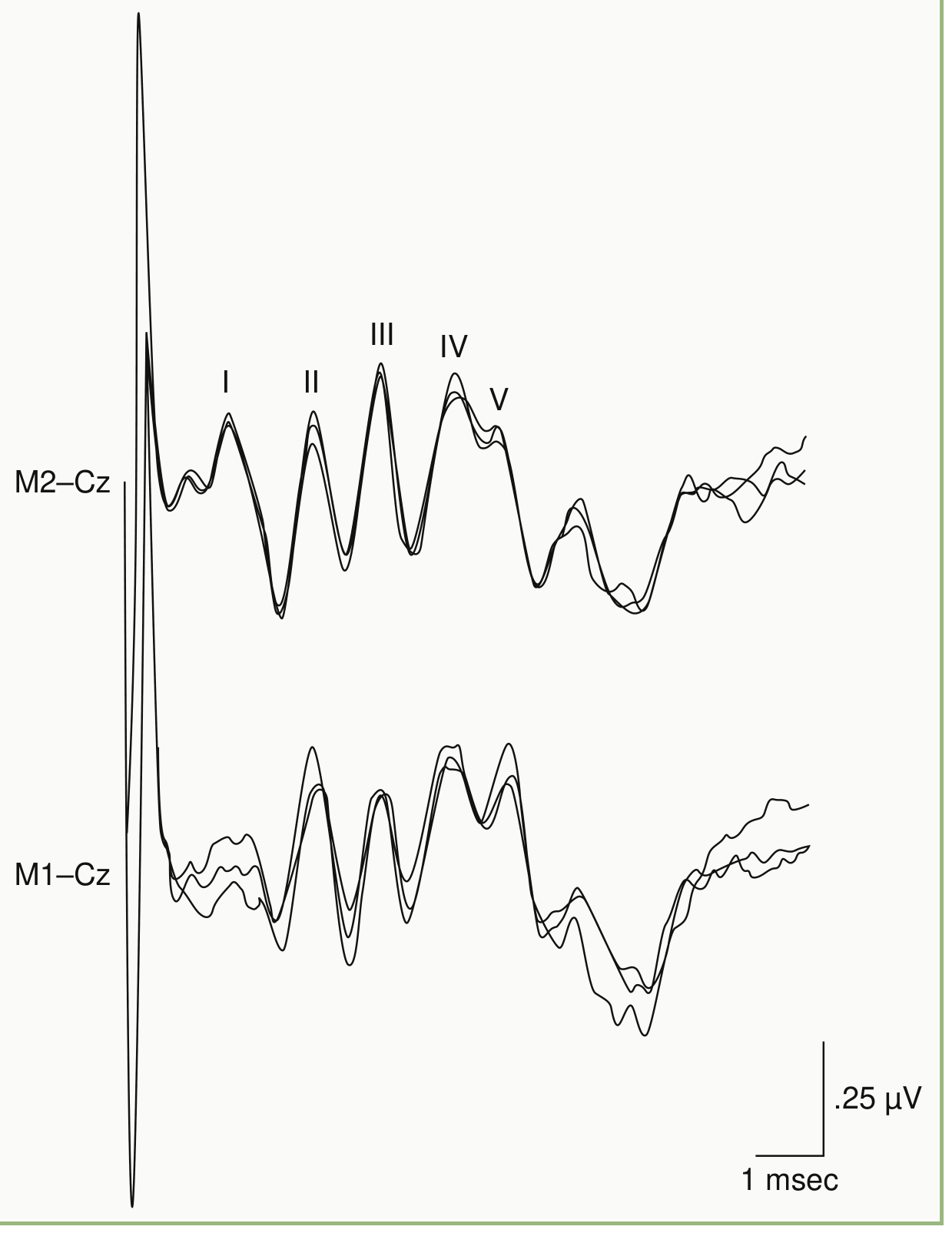
Normal BAEP recording. Wave components I-V are labeled with roman numerals. Clinical interpretation focuses primarily on latency of waves I, III, and V. - Bradley and Daroff's Neurology in Clinical Practice
Key Differences in Detail
1. Objectivity vs Subjectivity
ABR records the brain's own electrical response - no one has to judge whether a response occurred. Behavioural audiometry (especially BOA) depends on an observer deciding whether a baby's eye widened or limb moved, introducing significant inter-tester variability. - Scott-Brown's Otorhinolaryngology, Vol 2
2. Effect of Consciousness and Sedation
One of ABR's most clinically important features: "BAEPs persist essentially unchanged into deep coma or in the presence of general anaesthesia" in the absence of anatomical lesions. This makes ABR usable in unconscious or sedated patients. Behavioural tests require a conscious, alert patient.
- Bradley and Daroff's Neurology in Clinical Practice
3. Scope of the Auditory System Assessed
This is the critical limitation of ABR: "While electrophysiological testing has the advantage of being objective in terms of the child's response, behavioural and speech discrimination testing remain the only functional measures for assessing the complete auditory system."
- Scott-Brown's Otorhinolaryngology, Vol 2
ABR only tests the pathway up to the brainstem - it cannot assess cortical processing, speech understanding, or the full functional hearing experience. Behavioural audiometry, especially speech discrimination tests, evaluates the entire system.
4. When Each is Used
| Clinical Scenario | Preferred Test |
|---|---|
| Newborn hearing screening | ABR / OAE (objective, no cooperation needed) |
| Infant under 6 months | ABR (electrophysiological) |
| Infant 5-36 months (developmental age) | VRA (behavioural, conditioned) |
| Child unable to cooperate (learning disability) | ABR (as fallback) |
| Confirming thresholds pre-cochlear implant | ABR |
| Suspected non-organic hearing loss | ABR (cannot be faked) |
| Screening for acoustic neuroma | ABR (>90% sensitivity) |
| Assessing speech understanding | Behavioural only |
5. Sensitivity for Pathology
ABR is a highly sensitive screening test for acoustic neuroma, detecting abnormalities in greater than 90% of patients. Findings include prolongation of the I-III interpeak interval, distortion or loss of later wave components, or complete absence of waveform. Behavioural tests cannot localize a retrocochlear lesion. - Bradley and Daroff's Neurology in Clinical Practice
Summary
ABR is the objective, electrophysiological gold standard when patient cooperation is impossible or when retrocochlear pathology is suspected. Behavioural audiometry is subjective but remains the only way to assess the complete functional auditory system, including higher cortical processing and speech discrimination. The two are complementary, not mutually exclusive - complete audiological evaluation in children often requires both.
This is a shared conversation. Sign in to Orris to start your own chat.