Intestinal TB
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching PubMed
"intestinal tuberculosis" AND diagnosis
Finding Sources
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Intestinal Tuberculosis
Overview
Intestinal TB is a form of extrapulmonary tuberculosis (EPTB) caused by Mycobacterium tuberculosis (or occasionally M. bovis). It accounts for 1-3% of all TB cases worldwide. Among EPTB presentations, it is less common than lymph node, genitourinary, bone/joint, or meningeal disease - but its frequency is rising with HIV co-infection and global migration.
Aetiology and Routes of Infection
Three routes of intestinal involvement:
- Swallowing of infected sputum - from active pulmonary or laryngeal TB (historically the most common)
- Ingestion of contaminated unpasteurized milk - caused by M. bovis (important in non-endemic countries)
- Haematogenous/miliary spread - direct extension from adjacent infected organs
Importantly, active pulmonary TB is no longer required for intestinal TB to develop - chest X-rays are normal at time of diagnosis in many cases. - Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 2207
Key risk factors: HIV infection (up to 50% of TB in HIV-positive patients is EPTB), malignancies (especially lymphoma), glucocorticoid use, and anti-TNF agent therapy.
Sites of Involvement
Any region from mouth to anus can be affected, but the terminal ileum and caecum are involved in 75% of cases. This is due to the abundance of lymphoid tissue (Peyer's patches) in that region and the physiological slowing of intestinal contents.
Critically, both sides of the ileocaecal valve are typically affected, leading to valve incompetence - a feature that helps distinguish intestinal TB from Crohn's disease, which tends to respect the valve. - Sleisenger and Fordtran's, p. 2207
Pathology
Gross Morphology (3 Types)
| Type | Frequency | Features |
|---|---|---|
| Ulcerative | ~60% | Multiple superficial, transverse ulcers with undermined edges; serosa studded with tubercles; heals with fibrosis → strictures |
| Hypertrophic | ~10% | Scarring, fibrosis, heaped-up mass; can mimic carcinoma or Crohn's disease |
| Ulcero-hypertrophic | ~30% | Combination of ulceration + healing/scarring |
- The ulcerative type indicates organism virulence > host resistance. Transverse ulcers heal to form multiple strictures causing obstruction.
- The hypertrophic type occurs when host resistance is greater; there is marked inflammatory thickening of the terminal ileum, narrowing the lumen. Fibrosis pulls the caecum upward into a subhepatic position, widening the ileocaecal angle beyond 90°.
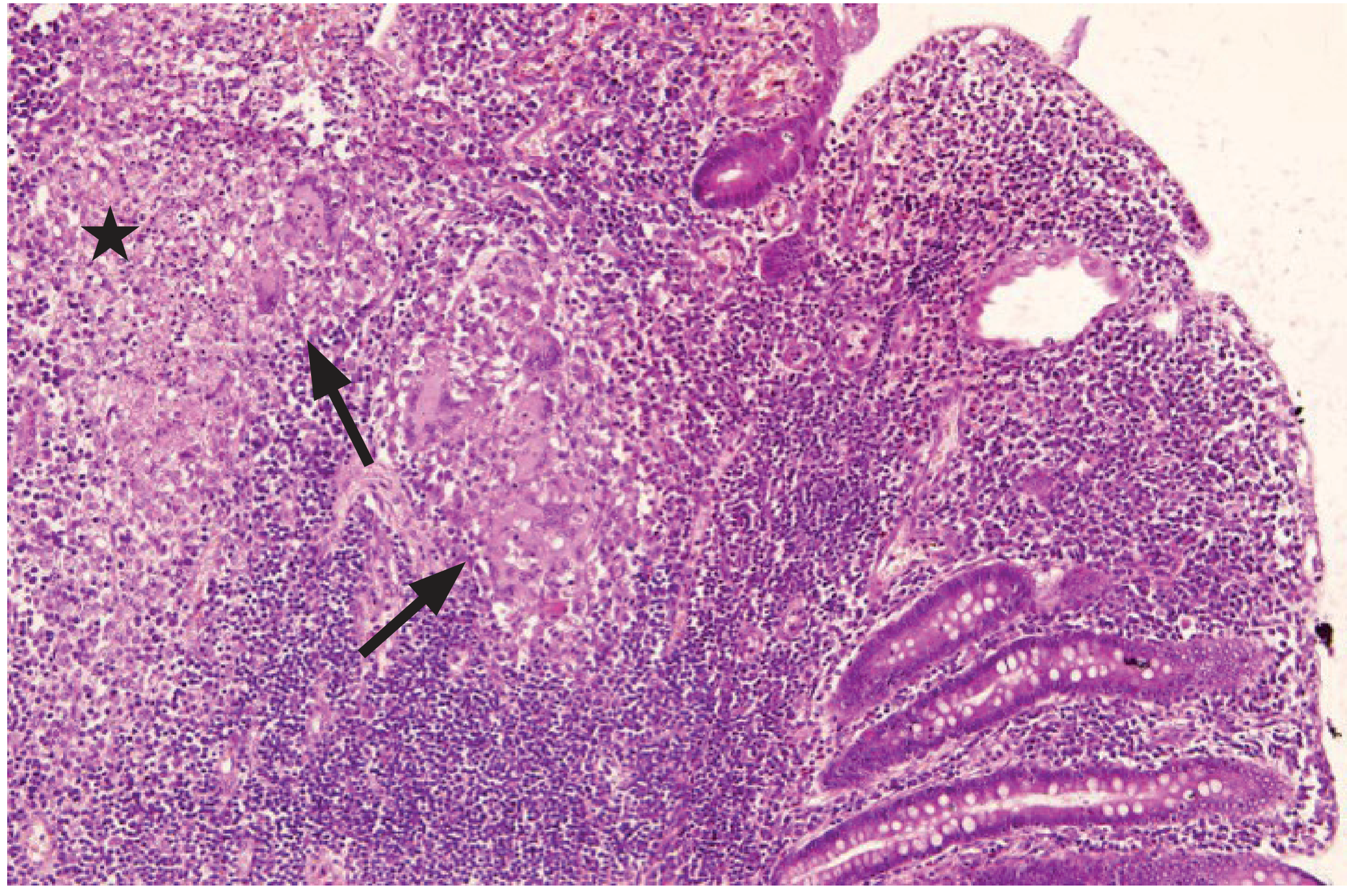
Histology
The hallmark is the caseating granuloma - epithelioid cell granulomas with central caseation and Langhans giant cells, seen in 50-80% of biopsy specimens.
Clinical Features
Elective / Chronic Presentation
- Weight loss, malaise, evening pyrexia with night sweats
- Alternating constipation and diarrhoea
- Chronic, vague, non-specific abdominal pain (80-90% of patients) - may mimic appendicitis
- Palpable right iliac fossa mass (in 25-50% of cases) from the hyperplastic type
- Abdominal distension with a "doughy" feel from loculated ascites
- Multiple fistula-in-ano with watery, undermined edges
Emergency Presentation
- Features of distal small bowel obstruction (from ileal strictures): pain, distension, constipation, bilious/faeculent vomiting
- Rarely, peritonitis from perforation of a tuberculous ulcer
Complications
Intestinal obstruction, haemorrhage, perforation, fistula formation (including entero-enteric, entero-vesical), malabsorption (from SIBO proximal to strictures), and perianal disease. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Investigations
| Investigation | Findings |
|---|---|
| Blood tests | Raised ESR/CRP, mild anaemia, normal or low WBC |
| Sputum culture | Positive if concurrent pulmonary TB |
| Tuberculin skin test / IGRA | Supportive but not diagnostic; false-negative in HIV/elderly |
| Chest X-ray | May show pulmonary infiltrates; often normal |
| Abdominal USS | Loculated ascites, lymphadenopathy |
| CT abdomen | Bowel wall thickening, ileocaecal valve thickening, central necrotic/hypodense mesenteric lymph nodes (>1 cm = strongly suggestive), contracted caecum |
| Barium meal/follow-through | Multiple ileal strictures, subhepatic caecum |
| Colonoscopy + biopsy | Most useful procedure - histopathology, AFB staining, PCR, culture + sensitivity |
| PCR (tissue or stool) | Sensitivity ~65%; higher than AFB stain (~20%) |
| Xpert MTB/RIF | Emerging - 2024 meta-analysis confirmed useful accuracy for ITB diagnosis (PMID: 37531292) |
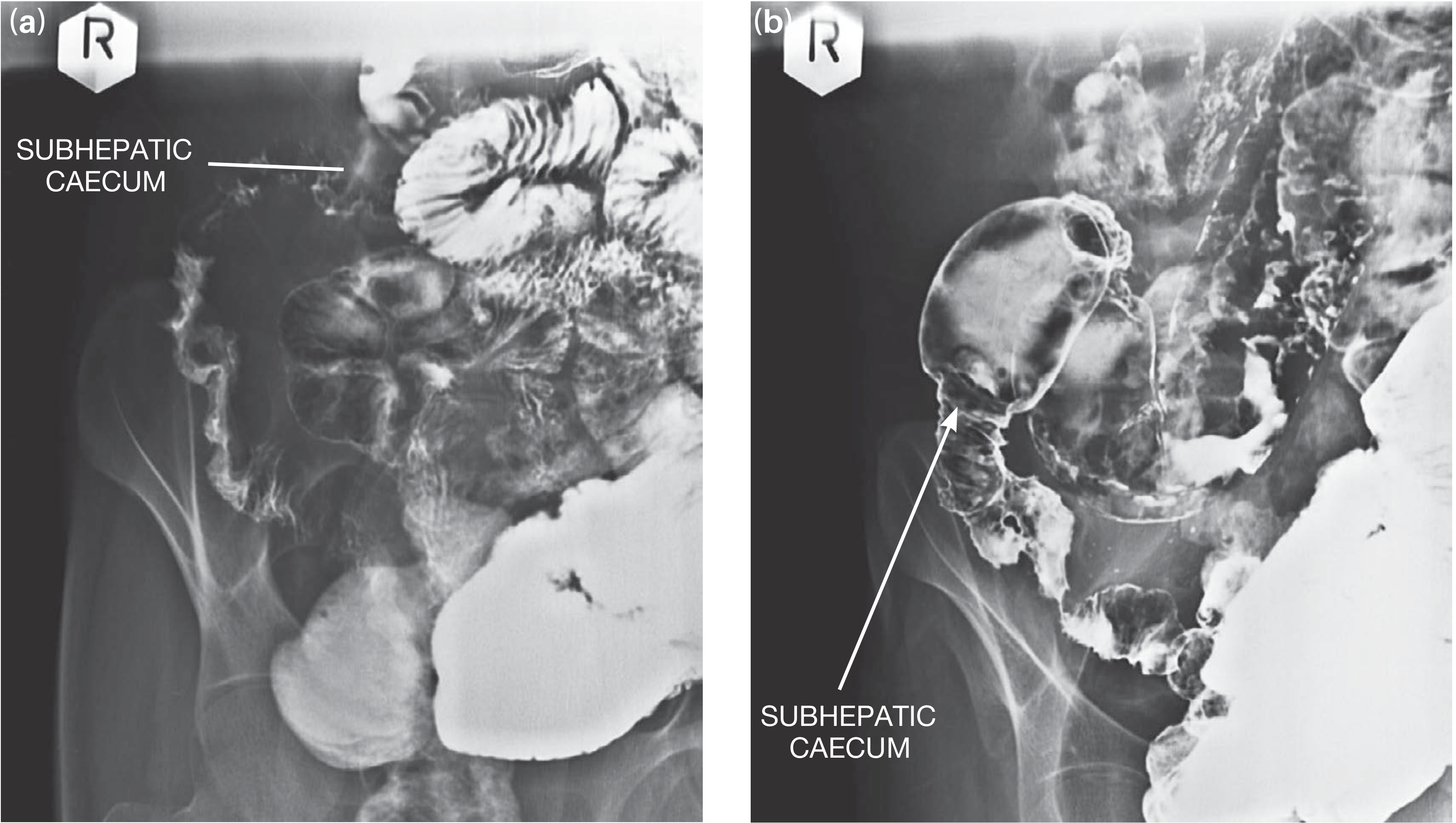
Radiology: Key Signs
- Stierlin sign: Conification (cone-shaped) of the caecum on barium enema, with contraction on both sides of the ileocaecal valve - characteristic of intestinal TB
- Subhepatic caecum: Fibrosis causes shortening and upward pull of the caecum into a subhepatic position, with the ileocaecal angle > 90°
- Calcified mesenteric lymph nodes: Suggest healed or chronic disease
- CT: Central necrosis in lymph nodes (caseous) strongly favours TB over Crohn's
Differentiating Intestinal TB from Crohn's Disease
This is one of the most clinically important distinctions, as anti-TNF therapy used in Crohn's can reactivate TB with devastating consequences.
| Feature | Intestinal TB | Crohn's Disease |
|---|---|---|
| Ileocaecal valve | Incompetent (both sides involved) | Usually spared/respected |
| Ulcer orientation | Transverse, circumferential | Linear, along bowel axis |
| Lymph nodes | Large (>1 cm), hypodense/necrotic | Smaller, non-necrotic |
| Granulomas | Large, confluent, caseating | Small, non-caseating |
| Perianal disease | Less common | Very common |
| Stierlin sign | Present | Absent |
| AFB/PCR | May be positive | Negative |
| Response to steroids | Worsens (can precipitate perforation) | Improves |
A 2024 systematic review on AI-based discrimination of these two conditions (PMID: 38058246) highlights the ongoing diagnostic challenge.
Treatment
Medical (First-line)
Standard multi-drug anti-tubercular therapy (ATT) in two phases:
- Intensive phase (2 months): Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) - i.e., 2HRZE
- Maintenance phase (4 months): Isoniazid + Rifampicin - i.e., 4HR
- Total duration: 6 months (may be extended to 9-12 months for complex disease)
Patients should be co-managed by a physician and surgeon throughout. After medical treatment, re-imaging the small bowel (barium/MRI) is done to assess for residual strictures.
Surgical (Indicated for)
- Intestinal obstruction not relieved by medical therapy
- Perforation and peritonitis
- Fistula formation (unresponsive to medical therapy)
- Haemorrhage
- Diagnostic uncertainty (where malignancy/IBD cannot be excluded)
Surgical Options
- Elective: Limited ileocolic resection with anastomosis; strictureplasty for single ileal strictures; right hemicolectomy for extensive ileocolic disease. Resections are kept as conservative as possible (same principles as Crohn's)
- Emergency: Minimum life-saving procedure - diseased segment resection with proximal ileostomy + distal mucus fistula (anastomosis avoided due to high leak risk in active infection + poor nutritional state). One-stage resection-anastomosis is rarely performed if general condition permits. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Key Takeaway Points
- Most common site: terminal ileum + caecum (75%)
- Hallmark histology: caseating granulomas (50-80% of biopsies)
- Classic X-ray finding: Stierlin sign + subhepatic caecum
- Most important DDx: Crohn's disease - critical to exclude TB before starting biologics
- Colonoscopy with biopsy (HPE + AFB + PCR + culture) is the most useful diagnostic procedure
- Treatment: 6 months ATT (2HRZE/4HR) is the backbone; surgery reserved for complications
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Bailey and Love's Short Practice of Surgery, 28th Ed. | Murray & Nadel's Textbook of Respiratory Medicine | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.