Fallots tetrology
Reading File
Finding Sources
Searching PubMed
"tetralogy of Fallot"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive answer. Here is the full coverage of Tetralogy of Fallot:
Tetralogy of Fallot (TOF)
Tetralogy of Fallot is the most common cyanotic congenital heart disease, accounting for ~5% of all congenital cardiac malformations. It is the classic "blue baby" defect beyond infancy.
The Four Cardinal Features
All four defects arise from a single embryologic root cause: anterosuperior displacement of the infundibular (outlet) septum, causing unequal division of the truncus arteriosus.
| Feature | Detail |
|---|---|
| 1. Ventricular Septal Defect (VSD) | Large, unrestrictive, perimembranous defect near the outlet septum |
| 2. Right Ventricular Outflow Tract (RVOT) Obstruction | Usually subpulmonic (infundibular) stenosis; can also involve pulmonary valve stenosis or complete pulmonary atresia |
| 3. Overriding Aorta | Aortic valve straddles the VSD, receiving blood from both ventricles |
| 4. Right Ventricular Hypertrophy (RVH) | Secondary to the pressure load imposed by the RVOT obstruction |
Embryology
-
The subpulmonic conus fails to expand normally
-
This produces anterocephalad deviation of the outlet septum with hypertrophy of the septoparietal trabeculations
-
The result is simultaneous subpulmonary stenosis, malalignment VSD, and an aorta that overrides the defect
-
The RVH is entirely secondary - it is not a primary developmental defect
-
The Developing Human (Moore), p. 4435-4447
Gross Morphology
-
Heart is enlarged and "boot-shaped" (coeur en sabot) due to RVH with a concave main pulmonary artery segment
-
Proximal aorta is dilated; pulmonary trunk is hypoplastic
-
Left-sided chambers are normal in size
-
RV wall can be as thick or thicker than the LV
-
In severe cases (pulmonary atresia): a persistent PDA or bronchial collateral vessels are the only routes for pulmonary blood flow
-
Robbins & Kumar Basic Pathology, p. 288-292
Hemodynamics
The degree of clinical severity is directly determined by the severity of RVOT obstruction:
- Mild RVOT obstruction ("Pink Tet"): Left-sided pressure still dominates → left-to-right shunt → no cyanosis. Pink tets gradually become cyanotic by 1-3 years of age.
- Severe RVOT obstruction: Right-to-left shunting of deoxygenated blood → cyanosis from early infancy. Infants with severe obstruction may need PGE1 to maintain pulmonary flow via the PDA.
Clinical Features
Symptoms:
- Cyanosis (may deepen with crying, feeding, or exertion)
- Dyspnea on exertion
- Squatting posture in older children (increases SVR, reduces right-to-left shunt)
- Compensatory polycythemia
- Digital clubbing
Examination:
- Varying cyanosis
- Systolic ejection murmur along the left sternal border (from RVOT obstruction - not from the VSD, which is typically silent)
- Single second heart sound (soft P2 due to low pulmonary pressure)
- RV heave
Investigations:
| Test | Findings |
|---|---|
| Chest X-ray | Boot-shaped heart, decreased pulmonary vascular markings, right-sided aortic arch in ~25% |
| ECG | Right axis deviation, RVH; in repaired adults: complete RBBB |
| Echocardiography | Confirms anatomy, assesses RVOT gradient, VSD, PA size |
| CMR | Best for RV volumes, pulmonary regurgitation severity, branch PA anatomy |
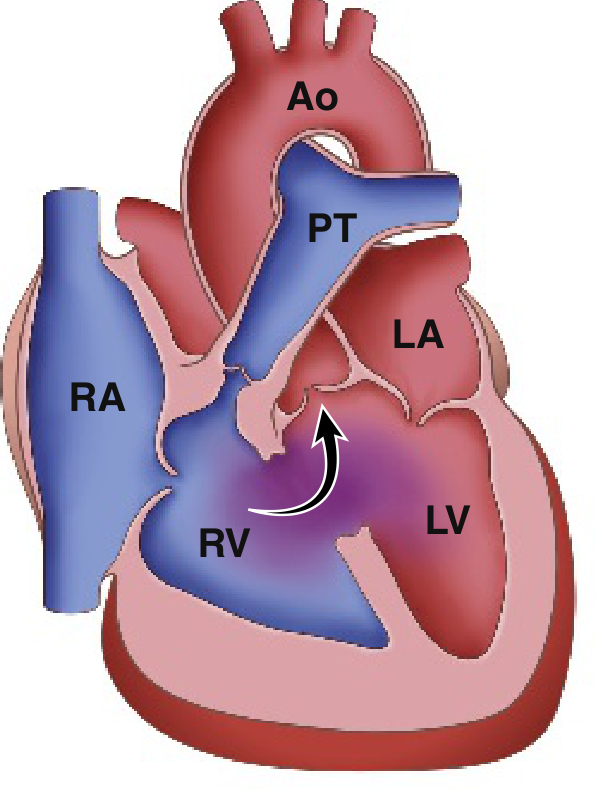
Tet Spells (Hypercyanotic / Hypoxic Spells)
Peak incidence: 2-4 months of age. Triggered by any event that drops SVR (crying, defecation, fever, hypovolemia, tachycardia).
Vicious cycle:
↓ SVR → ↑ R→L shunt via VSD
→ ↓ PaO₂, ↑ PCO₂, ↓ pH (acidosis)
→ Hyperpnea → ↑ venous return to RV
→ More blood shunted R→L → ↑ hypoxia
→ Further ↓ SVR → worsening spell
Management of a Tet Spell (Rosen's Box 165.8)
- Knee-to-chest position - compresses femoral arteries, raises SVR, reduces R-to-L shunt
- Supplemental oxygen (limited benefit alone)
- Morphine 0.1-0.2 mg/kg IV/IM (reduces hyperpnea, decreases sympathetic tone)
- Fentanyl 1 µg/kg IV/IM (alternative to morphine); or 1.5-2 µg/kg intranasally
- Midazolam 0.2-0.3 mg/kg intranasally
- Sodium bicarbonate 1 mEq/kg IV if acidosis present
- Ketamine 1-2 mg/kg IV or 3-5 mg/kg IM (raises SVR)
- Propranolol 0.1-0.2 mg/kg (reduces infundibular spasm)
- Phenylephrine 0.01-0.02 mg/kg IV (pure alpha agonist, raises SVR)
Associated Anomalies
- Right-sided aortic arch (~25%)
- Coronary artery anomalies - most commonly LAD originating from RCA, crossing the RVOT (surgical importance: may require RV-to-PA conduit instead of direct RVOT patch)
- ASD ("Pentalogy of Fallot" when ASD is present)
- AVSD (in Down syndrome)
Anatomic Variants
| Variant | Features |
|---|---|
| TOF with pulmonary atresia + MAPCAs | ~15% of TOF; no direct RV-PA connection; pulmonary flow via PDA and major aortopulmonary collateral arteries; repair requires unifocalization |
| TOF with absent pulmonary valve | Markedly stenotic annulus, absent/rudimentary leaflets; massively dilated/aneurysmal PAs causing airway compression |
| "Pink Tet" | Minimal RVOT obstruction, initially acyanotic |
Surgical Management
Palliative shunts (when primary repair is not feasible):
- Blalock-Taussig-Thomas (BTT) shunt - subclavian artery to PA; increases pulmonary blood flow
Definitive repair (preferred - primary repair in early infancy is now standard):
- VSD closure with a patch
- RVOT reconstruction (infundibulectomy + patch, or transannular patch if annulus is small)
- Branch PA augmentation if hypoplastic
A 2024 systematic review and meta-analysis (PMID 39444206) comparing primary vs. staged repair in symptomatic neonates found primary repair to be a viable approach, supporting the current trend toward early complete correction.
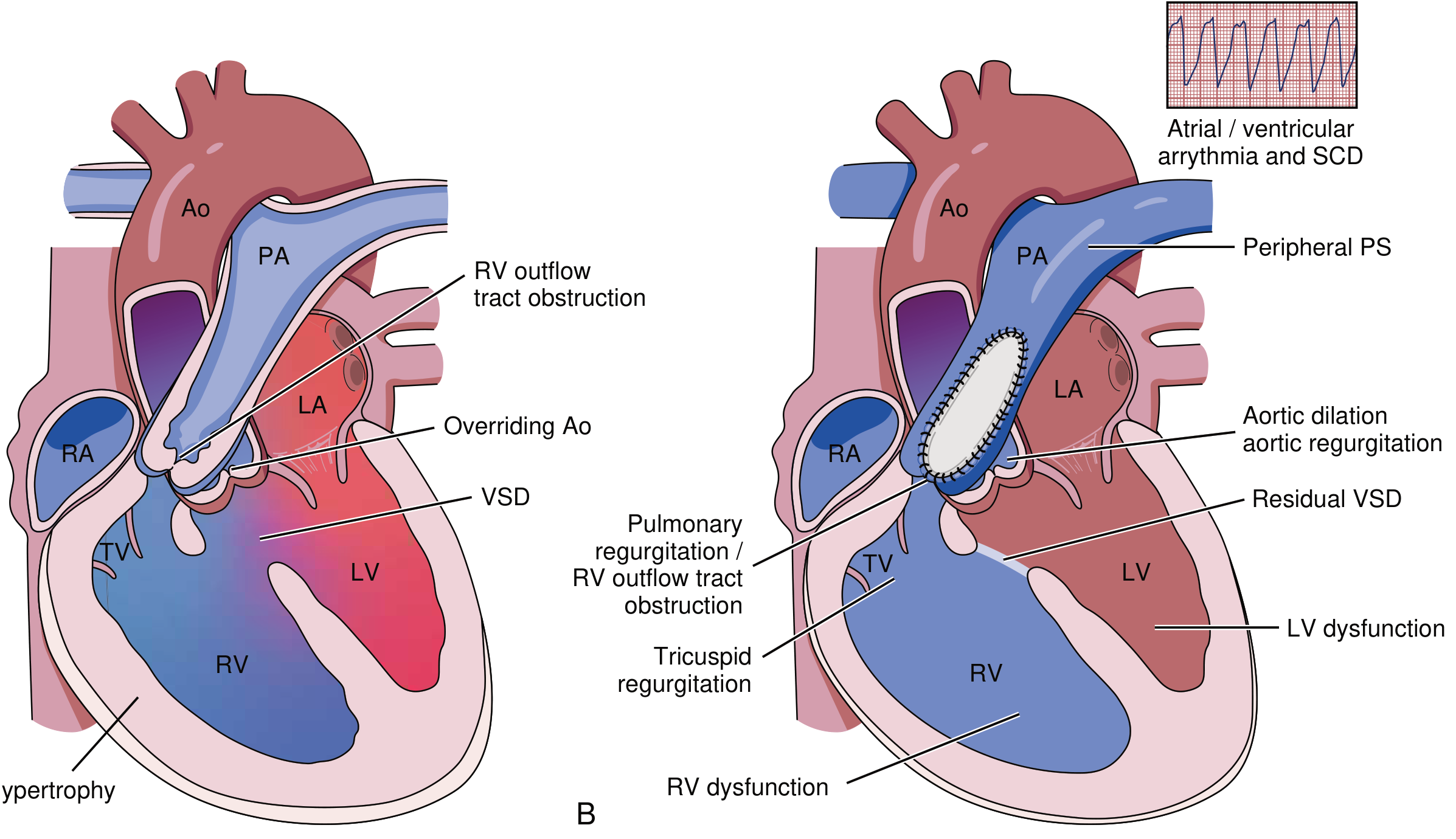
Long-term Complications After Repair
Repaired TOF patients are one of the largest adult congenital heart disease (ACHD) populations. Lifelong follow-up is mandatory.
| Complication | Notes |
|---|---|
| Pulmonary regurgitation (PR) | Most common long-term problem after transannular patch repair; leads to progressive RV dilatation |
| RVOT obstruction (residual/recurrent) | From residual stenosis or conduit dysfunction |
| RV dysfunction / failure | From chronic PR and volume overload |
| Residual VSD | Requires re-intervention if significant |
| Aortic root dilatation + aortic regurgitation | From intrinsic aortopathy |
| Arrhythmias | VT (from RVOT scar), AF/flutter; risk of sudden cardiac death (SCD) |
| Complete RBBB | Near-universal after ventriculotomy-based repair |
Pulmonary valve replacement (PVR) is the key re-intervention - timing is guided by RV volumes on CMR (RV end-diastolic volume index >160 mL/m² is a common threshold), symptoms, and exercise tolerance.
- Braunwald's Heart Disease, p. 2774-2808
Key Points Summary
- TOF = VSD + RVOT obstruction + overriding aorta + RVH - all from one embryologic defect (infundibular septum malalignment)
- Most common cyanotic CHD beyond infancy (~5% of all CHD)
- Clinical severity tracks with degree of RVOT obstruction
- Tet spells: manage with knee-chest position + morphine + bicarbonate ± phenylephrine
- Definitive treatment is surgical correction - primary repair in infancy is preferred
- Long-term: pulmonary regurgitation is the dominant post-repair problem, monitored with CMR; PVR when RV is significantly dilated
- Right aortic arch in 25%; coronary anomalies must be excluded before surgery
According to 1st year mbbs
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Here is Tetralogy of Fallot explained at the 1st year MBBS level - covering Anatomy, Embryology, and basic Physiology (the three subjects in 1st year).
Tetralogy of Fallot - 1st Year MBBS
What is it?
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart disease. It accounts for ~5% of all congenital heart defects. "Tetralogy" means a group of four defects, all present together.
The Four Defects (Must Memorize)
Mnemonic: PROVE - Pulmonary stenosis, RVH, Overriding aorta, VSD
| # | Defect | Simple Meaning |
|---|---|---|
| 1 | Pulmonary stenosis (RVOT obstruction) | The opening from the right ventricle to the lungs is narrowed |
| 2 | Ventricular Septal Defect (VSD) | A hole between the right and left ventricles |
| 3 | Overriding Aorta | The aorta sits on top of both ventricles (straddles the VSD) instead of only the left |
| 4 | Right Ventricular Hypertrophy (RVH) | The right ventricle wall thickens because it has to pump against high resistance |
Embryology (Most Important for 1st Year)
This is the key topic for 1st year. TOF arises from one single embryological error that causes all four defects.
Normal Development (Quick Recap)
- The primitive heart tube has a single outflow channel called the truncus arteriosus
- The truncus arteriosus is divided into the aorta and pulmonary trunk by a spiraling septum called the aorticopulmonary septum
- At the same time, the interventricular septum grows upward to close the gap between the two ventricles
- The infundibular (outlet) septum separates the outflows of the two ventricles
What Goes Wrong in TOF
Anterosuperior displacement of the infundibular septum during development
When the infundibular septum shifts forward and upward instead of staying in the midline:
Infundibular septum displaced anterosuperiorly
↓
┌─────────────────────────────────┐
│ Unequal division of truncus │
│ arteriosus │
└──────────┬──────────────────────┘
│
┌──────────▼──────────────────────┐
│ Pulmonary trunk → too SMALL │ → Pulmonary stenosis (#1)
│ Aorta → too BIG (dilated) │
└──────────┬──────────────────────┘
│
┌──────────▼──────────────────────┐
│ Interventricular septum │
│ cannot close properly │ → VSD (#2)
└──────────┬──────────────────────┘
│
┌──────────▼──────────────────────┐
│ Large aorta shifts to sit │
│ over the VSD │ → Overriding aorta (#3)
└──────────┬──────────────────────┘
│
┌──────────▼──────────────────────┐
│ RV pumps against obstruction │
│ → wall thickens │ → RVH (#4)
└─────────────────────────────────┘
- Note: RVH is secondary - it is not a primary developmental defect. It develops after birth as the RV works against the RVOT obstruction.
- Extreme form: Pulmonary atresia with VSD - the pulmonary trunk is completely blocked; all blood exits through the aorta. Lungs get blood only via a Patent Ductus Arteriosus (PDA) or bronchial collaterals.
The Developing Human - Moore (Clinically Oriented Embryology), p. 4435-4447
Robbins & Kumar Basic Pathology, p. 283
Anatomy of the Defects
1. The Heart's Shape
- The heart looks "boot-shaped" (coeur en sabot) on X-ray
- This is because the RV is massively enlarged and the pulmonary trunk segment is concave (small)
2. VSD Location
- Usually large and perimembranous (near the membranous part of the interventricular septum)
- Located just below the overriding aortic valve
3. Pulmonary Stenosis
- Most commonly infundibular (subpulmonic) - the narrowing is in the muscular outflow channel below the pulmonary valve
- Can also involve the pulmonary valve itself
- In extreme cases: pulmonary atresia (complete blockage)
4. Overriding Aorta
- The aortic root is displaced to the right and sits directly above the VSD
- It receives blood from BOTH the left and right ventricles
5. Right Ventricular Hypertrophy
- The RV wall becomes as thick or thicker than the LV
- This is a compensatory change, not a primary structural defect
Physiology - Why Cyanosis Occurs
Normal Blood Flow (for comparison):
Deoxygenated blood → RV → Pulmonary artery → Lungs → Oxygenated
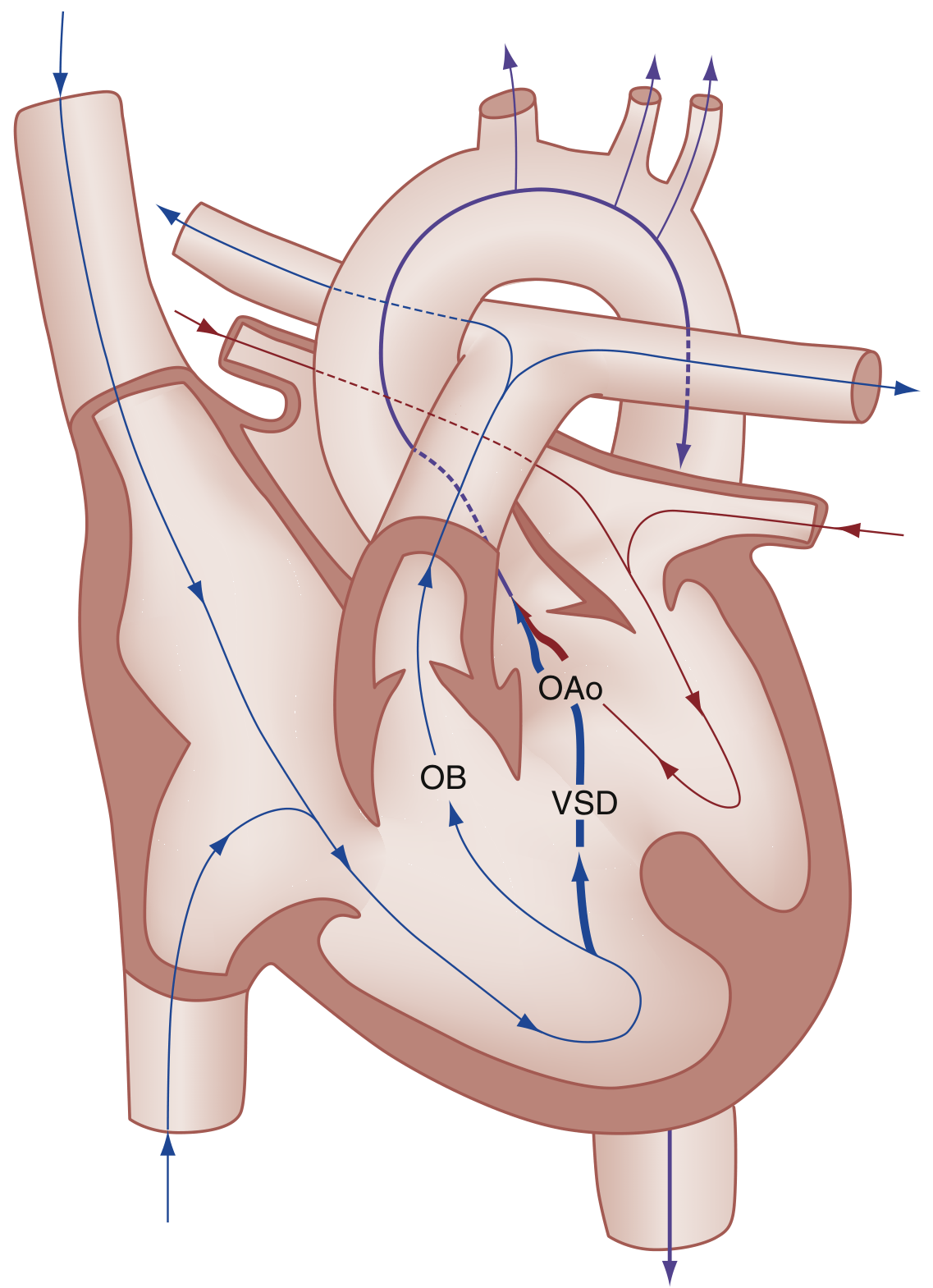
In TOF:
Deoxygenated blood in RV
↓
Pulmonary artery is NARROW (stenosis)
↓
Blood cannot easily go to lungs
↓
Takes the easier path → Through the VSD into LV
↓
Mixes with oxygenated blood from lungs
↓
Exits through the OVERRIDING AORTA
↓
Deoxygenated (mixed) blood goes to body
↓
CYANOSIS (blue baby)
This is called a Right-to-Left shunt - the direction blood shunts is reversed compared to a simple VSD.
The Severity Depends on How Narrow the Pulmonary Stenosis Is:
| Degree of Pulmonary Stenosis | Blood Shunt Direction | Cyanosis |
|---|---|---|
| Mild | Left-to-right (normal direction) | No cyanosis - called "Pink Tet" |
| Severe | Right-to-left | Cyanosis present |
- In "Pink Tets," cyanosis may not be present at birth but gradually develops by 1-3 years of age as the infundibular obstruction worsens
Simple Clinical Points (1st Year Level)
| Feature | What You Need to Know |
|---|---|
| Cyanosis | Most obvious sign - blue lips, tongue, fingers |
| Clubbing | Chronic low oxygen → finger/toe nail changes (develops over months-years) |
| Squatting | Child squats after exertion - squatting compresses leg arteries, raises blood pressure in systemic circulation, reduces the right-to-left shunt temporarily |
| Chest X-ray | Boot-shaped heart, decreased lung blood vessel markings |
| "Tet spell" | Sudden worsening of cyanosis (hypoxic spell), most common 2-4 months of age |
Summary Box for Exam
| Point | Answer |
|---|---|
| Most common cyanotic CHD? | Tetralogy of Fallot |
| % of all CHD? | ~5% |
| Number of defects? | 4 (tetralogy) |
| Embryological cause? | Anterosuperior displacement of the infundibular septum → unequal division of truncus arteriosus |
| Which defect is NOT primary? | RVH (it is secondary/compensatory) |
| Type of shunt? | Right-to-left shunt |
| Heart shape on X-ray? | Boot-shaped (coeur en sabot) |
| Most common RVOT obstruction type? | Infundibular (subpulmonic) stenosis |
| Extreme form? | Pulmonary atresia with VSD |
| Treatment? | Surgical correction |
Sources: The Developing Human - Moore (Embryology) | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.