Acid base balance full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the key images and content needed. Let me compile the comprehensive MD exam answer.
ACID-BASE BALANCE - Comprehensive MD Exam Answer (10 Marks)
1. NORMAL ACID-BASE HOMEOSTASIS
Systemic arterial pH is maintained between 7.35 and 7.45 by three integrated mechanisms:
- Extracellular and intracellular chemical buffers (immediate, seconds)
- Respiratory regulation of PaCO2 (minutes to hours)
- Renal regulation of plasma HCO3- (hours to days)
The relationship between these components is expressed by the Henderson-Hasselbalch equation:
pH = pK' + log [HCO3-] / (0.03 x PaCO2)
Where pK' = 6.1, and 0.03 is the solubility coefficient of CO2. At steady state, pH = 7.4 when [HCO3-] = 24 mEq/L and PaCO2 = 40 mmHg.
Normal daily acid production: ~50-70 mEq of fixed (non-volatile) acid from metabolism.
2. BUFFER SYSTEMS
A. Bicarbonate Buffer (most important extracellular buffer)
CO2 + H2O ⇌ H2CO3 ⇌ H+ + HCO3-
- pKa = 6.1 (far from physiological pH, yet most effective because CO2 is an open system - lungs continuously regulate CO2)
- Buffers ~50% of acid load
B. Proteins (Hemoglobin - most important intracellular buffer)
- Hb is the major intracellular buffer in blood
- Deoxyhemoglobin is a better buffer than oxyhemoglobin (Haldane effect)
C. Phosphate Buffer
- HPO4²- / H2PO4- system (pKa = 6.8)
- Important in urine acidification and intracellular buffering
D. Bone Buffer
- In chronic acidosis, bone carbonate and phosphate are mobilized - contributes to osteomalacia/osteoporosis
3. RESPIRATORY REGULATION
The respiratory system controls PaCO2 by adjusting alveolar ventilation:
- Acidosis → stimulates peripheral (carotid body) and central chemoreceptors → hyperventilation → decreased PaCO2 → pH rises
- Alkalosis → decreased chemoreceptor drive → hypoventilation → increased PaCO2 → pH falls
Respiratory compensation is rapid (minutes to hours) but incomplete - it returns pH toward, but not to, normal.
4. RENAL REGULATION
The kidney regulates pH by:
- Reabsorption of filtered HCO3- (proximal tubule: 80-85%; TAL and distal: remainder)
- Titratable acid excretion (mainly as H2PO4- in distal tubule)
- Ammonium (NH4+) excretion - most important for net acid excretion
- Proximal tubule generates NH4+ from glutamine
- NH4+ excreted in urine carries H+ out of the body
Renal compensation is slow (days) but complete (fully restores pH in isolated respiratory disorders).
5. CLASSIFICATION OF ACID-BASE DISORDERS
| Disorder | pH | Primary Change | Compensation |
|---|---|---|---|
| Metabolic acidosis | ↓ | HCO3- ↓ | PaCO2 ↓ (hyperventilation) |
| Metabolic alkalosis | ↑ | HCO3- ↑ | PaCO2 ↑ (hypoventilation) |
| Respiratory acidosis | ↓ | PaCO2 ↑ | HCO3- ↑ (renal) |
| Respiratory alkalosis | ↑ | PaCO2 ↓ | HCO3- ↓ (renal) |
6. COMPENSATION FORMULAS (Critical for MD Exams)
| Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | PaCO2 = 1.5 x [HCO3-] + 8 ± 2 (Winter's formula) |
| Metabolic alkalosis | PaCO2 increases by 0.7 mmHg per 1 mEq/L rise in HCO3- |
| Acute resp. acidosis | HCO3- increases by 1 mEq/L per 10 mmHg rise in PaCO2 |
| Chronic resp. acidosis | HCO3- increases by 3.5 mEq/L per 10 mmHg rise in PaCO2 |
| Acute resp. alkalosis | HCO3- falls by 2 mEq/L per 10 mmHg fall in PaCO2 |
| Chronic resp. alkalosis | HCO3- falls by 5 mEq/L per 10 mmHg fall in PaCO2 (only disorder where pH fully normalizes) |
- Harrison's Principles of Internal Medicine 22E, p. 411
7. ACID-BASE NOMOGRAM
The Davenport/acid-base nomogram plots pH vs. HCO3- with PCO2 isobars, showing 95% confidence bands for each simple disorder:
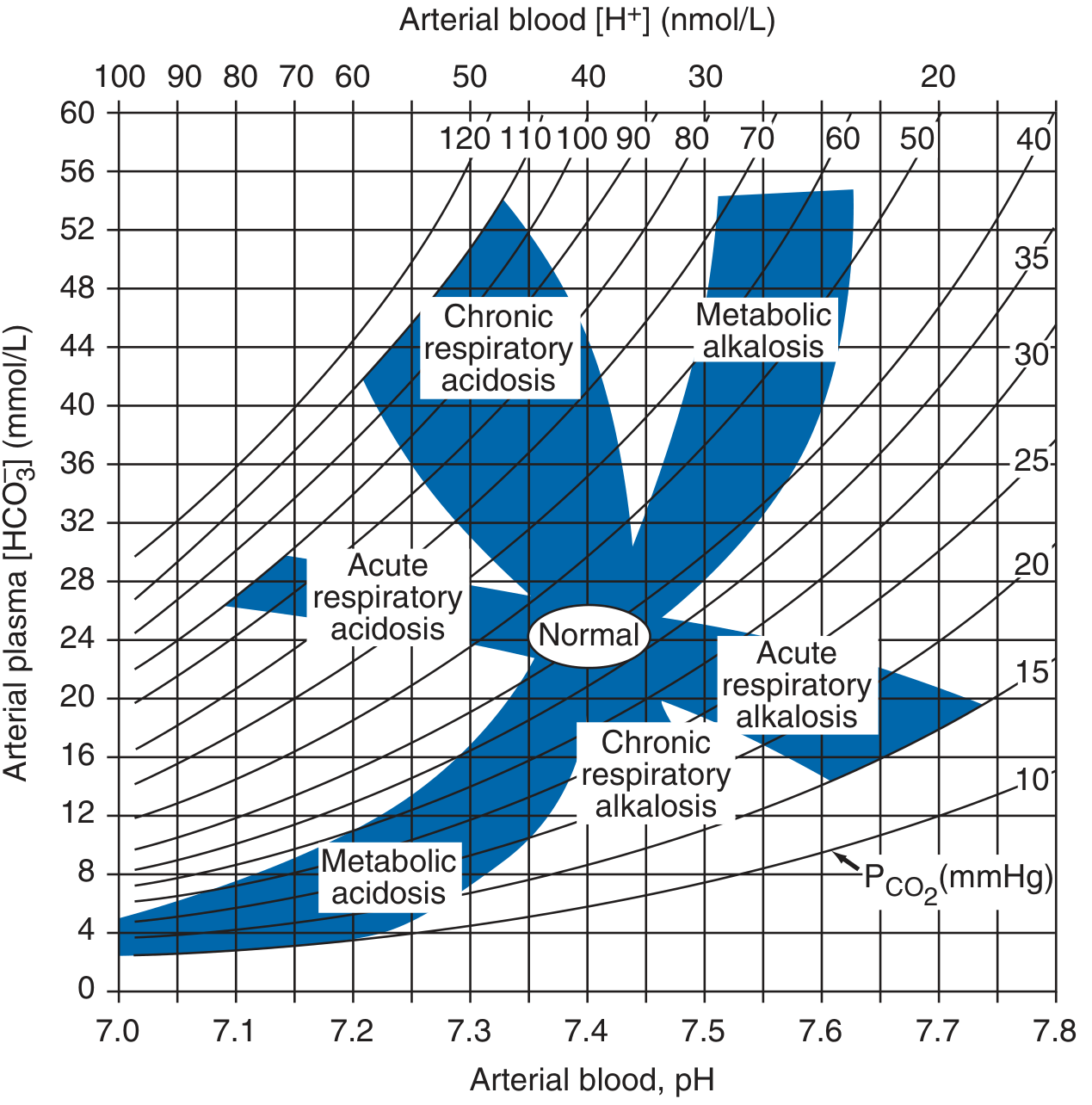
Acid-base nomogram (Harrison's Principles of Internal Medicine 22E) - shaded zones represent 95% confidence limits for simple disorders
8. METABOLIC ACIDOSIS
Definition
Primary fall in plasma HCO3- (< 22 mEq/L), with compensatory fall in PaCO2.
Causes - classified by Anion Gap
Anion Gap (AG) = Na+ - (Cl- + HCO3-)
- Normal AG = 6-12 mEq/L (average ~10 mEq/L)
- Corrected AG: add 2.5 mEq/L per 1 g/dL fall in serum albumin below 4.5 g/dL
High Anion Gap (HAGMA) - mnemonic MUDPILES:
- M - Methanol
- U - Uraemia (renal failure)
- D - DKA (diabetic ketoacidosis)
- P - Propylene glycol / Paraldehyde
- I - Isoniazid / Iron
- L - Lactic acidosis (type A: tissue hypoxia; type B: metformin, liver failure)
- E - Ethylene glycol
- S - Salicylates
Normal Anion Gap (hyperchloraemic) acidosis - mnemonic HARD-UP:
- Diarrhoea (most common - loss of HCO3-)
- Renal tubular acidosis (types 1, 2, 4)
- Ureterosigmoidostomy
- Addison's disease
- Post-hypocapnia
- Carbonic anhydrase inhibitors (acetazolamide)
Delta Ratio (for HAGMA) = (AG - 12) / (24 - HCO3-)
- <0.4: pure normal AG acidosis
- 0.4-0.8: mixed HAGMA + normal AG acidosis
- 1-2: pure HAGMA
-
2: HAGMA + concurrent metabolic alkalosis
Clinical Features
- Kussmaul breathing (deep, rapid - compensatory hyperventilation in severe metabolic acidosis)
- Decreased cardiac contractility, hypotension
- Decreased insulin sensitivity, hyperkalaemia
- Confusion, lethargy, coma
Treatment
- Treat underlying cause
- NaHCO3 rarely needed; use if pH < 7.1 or severe acidaemia with haemodynamic compromise
9. METABOLIC ALKALOSIS
Definition
Primary rise in plasma HCO3- (>26 mEq/L), with compensatory hypoventilation (PaCO2 rises).
Causes
Chloride-responsive (urine Cl- <10 mEq/L):
- Vomiting/nasogastric suction (loss of HCl)
- Diuretics (thiazides, loop)
- Post-hypercapnia
- Villous adenoma
Chloride-resistant (urine Cl- >20 mEq/L):
- Hyperaldosteronism (primary/secondary)
- Cushing's syndrome
- Bartter's/Gitelman's syndrome
- Severe hypokalaemia
Maintenance factors
- Volume depletion → increased aldosterone → renal HCO3- retention
- Hypokalaemia → increased renal H+ secretion
Treatment
- Chloride-responsive: IV saline (0.9%) + KCl; correct the underlying cause
- Chloride-resistant: treat underlying mineralocorticoid excess
10. RESPIRATORY ACIDOSIS
Definition
Primary rise in PaCO2 (>45 mmHg) with compensatory rise in HCO3-.
Causes (hypoventilation)
| CNS depression | Opiates, sedatives, anaesthesia, brainstem lesion |
|---|---|
| Neuromuscular | Myasthenia gravis, GBS, poliomyelitis, MND |
| Airway obstruction | COPD, severe asthma, foreign body |
| Chest wall | Kyphoscoliosis, obesity hypoventilation |
| Parenchymal | End-stage pulmonary fibrosis |
Acute vs Chronic
- Acute: HCO3- rises by 1 mEq/L per 10 mmHg rise in PaCO2; pH falls markedly
- Chronic: HCO3- rises by 3.5 mEq/L per 10 mmHg rise in PaCO2; pH nearly normal
Treatment
- Treat the cause
- Mechanical ventilation if severe
- Oxygen cautiously in COPD (avoid eliminating hypoxic drive)
11. RESPIRATORY ALKALOSIS
Definition
Primary fall in PaCO2 (<35 mmHg) with compensatory fall in HCO3-.
Causes (hyperventilation)
- Anxiety, psychogenic
- Hypoxaemia (pneumonia, PE, high altitude, severe anaemia)
- Sepsis (early) - most common cause of resp. alkalosis in ICU
- CNS stimulation (salicylates, fever, head injury)
- Pregnancy (progesterone effect)
- Liver failure (hepatic encephalopathy)
- Iatrogenic (mechanical ventilation)
Compensation
- Acute: HCO3- falls 2 mEq/L per 10 mmHg fall in PaCO2
- Chronic: HCO3- falls 5 mEq/L per 10 mmHg fall - only disorder where full pH compensation can occur
Clinical Features
- Paraesthesias (perioral, fingertips), carpopedal spasm
- Lightheadedness, syncope
- Decreased ionised calcium (alkalosis increases protein binding of Ca2+)
12. MIXED ACID-BASE DISORDERS
Defined as independently coexisting disorders (not just compensation). Common in critically ill patients.
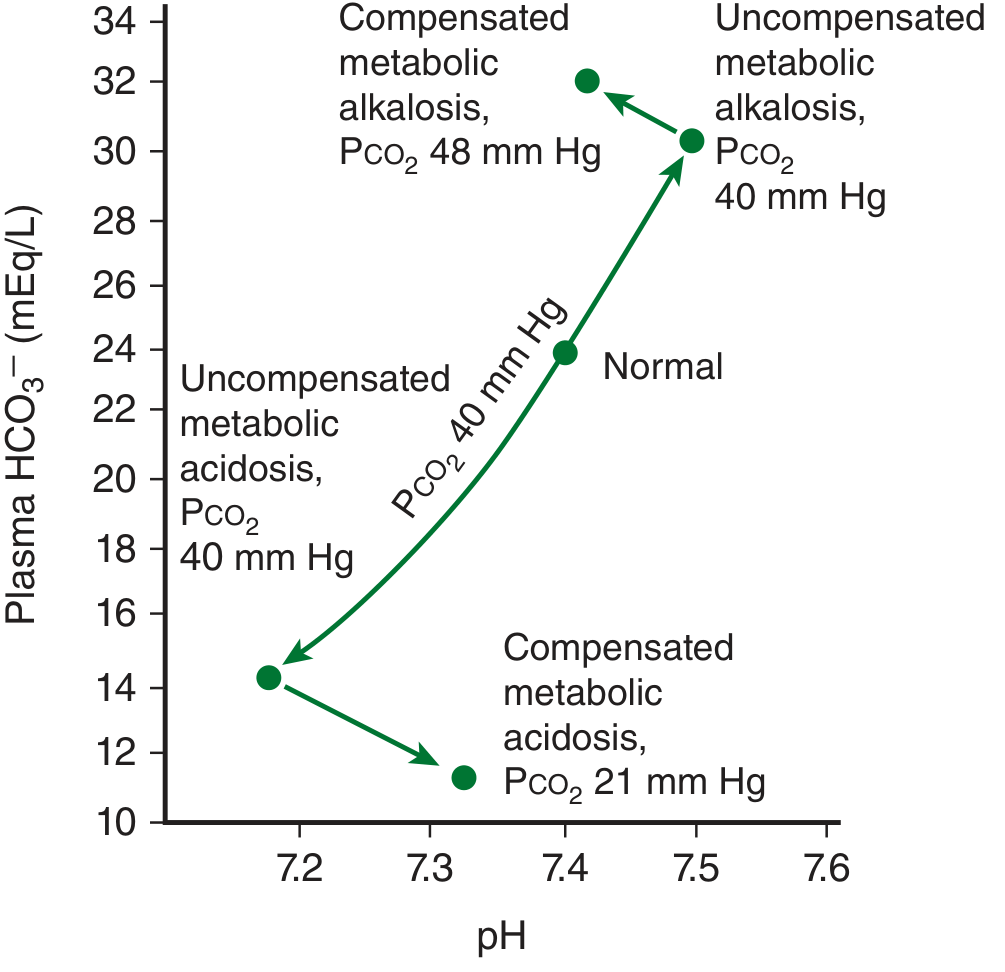
Acid-base paths during metabolic acidosis and alkalosis (Ganong's Review of Medical Physiology, 26th Ed.)
| Mixed Disorder | pH change | Example |
|---|---|---|
| Met. acidosis + Resp. acidosis | Severe ↓↓ | Cardiac arrest, severe COPD + DKA |
| Met. acidosis + Resp. alkalosis | May be near normal | Sepsis + shock, salicylate poisoning |
| Met. alkalosis + Resp. acidosis | May be near normal | COPD + diuretics/vomiting |
| Met. acidosis + Met. alkalosis | pH variable | DKA + vomiting |
Key: If PaCO2 deviates from the predicted compensation (using Winter's formula or compensation table), a mixed disorder is present.
13. SYSTEMATIC APPROACH TO ABG INTERPRETATION (Step-by-Step)
- Check pH - acidaemia (<7.35) or alkalaemia (>7.45)?
- Check PaCO2 - elevated, normal, or low?
- Check HCO3- - elevated, normal, or low?
- Identify the primary disorder - which change (CO2 or HCO3-) explains the pH direction?
- Calculate expected compensation - using formulas above
- Compare actual vs. expected compensation - deviation = mixed disorder
- Calculate Anion Gap - if metabolic acidosis present
- Calculate Delta Ratio - if HAGMA present
- Correlate with clinical context
14. KEY NORMAL VALUES (Reference)
| Parameter | Normal Range |
|---|---|
| Arterial pH | 7.35-7.45 |
| PaCO2 | 35-45 mmHg |
| HCO3- | 22-26 mEq/L |
| PaO2 | 80-100 mmHg |
| Base excess | -2 to +2 mEq/L |
| Anion Gap | 6-12 mEq/L |
15. SPECIAL TOPICS FOR MD EXAMS
Renal Tubular Acidosis (RTA) - Normal AG acidosis
| Type | Defect | Urine pH | K+ | Cause |
|---|---|---|---|---|
| Type 1 (Distal) | Failure to acidify urine | >5.5 | Low | SLE, Sjogren's, amphotericin |
| Type 2 (Proximal) | Failure to reabsorb HCO3- | <5.5 | Low | Multiple myeloma, Wilson's |
| Type 4 | Aldosterone deficiency/resistance | <5.5 | High | DM nephropathy, Addison's |
Lactic Acidosis
- Type A: Tissue hypoperfusion - shock, cardiac arrest, severe anaemia, CO poisoning
- Type B: No obvious hypoperfusion - metformin toxicity, liver failure, thiamine deficiency, malignancy
Salicylate Poisoning - Classic Mixed Disorder
- Early: Respiratory alkalosis (direct CNS stimulation)
- Late: Metabolic acidosis (HAGMA) + Respiratory alkalosis simultaneously
- Classic exam scenario
Sources: Harrison's Principles of Internal Medicine 22E (2025), Ganong's Review of Medical Physiology 26th Ed., Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.