Hello to all Anatomy imp questions : Dural sinus venous Facial nerve Layers of the scalp Triangles -4 Cavernous sinus Deep servical fascia Bells palsy Black eye Dangerous layer of scalp
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
layers of scalp SCALP mnemonic dangerous layer anatomy
Reading File
Reading File
Searching the Web
Bell's palsy facial nerve LMN UMN difference forehead sparing anatomy
All 9 topics covered in depth from authoritative medical textbooks. Here's a quick roadmap to what's above:
- Layers of the Scalp - S-C-A-L-P mnemonic with clinical significance of each layer
- Dangerous Layer - 4th layer (loose areolar), valveless emissary veins, route of infection to meninges
- Dural Venous Sinuses - All named sinuses, their courses and drainage patterns, all ultimately draining to the internal jugular vein
- Cavernous Sinus - Contents (ICA + CN VI inside; CN III, IV, V1, V2 in wall), connections, and clinical syndromes
- Facial Nerve - Full course through temporal bone (5 segments), all branches and their functions, terminal branches mnemonic
- Bell's Palsy - LMN palsy, HSV-1 etiology, forehead involvement (vs. UMN stroke), treatment within 72 hours
- Triangles of the Neck - Anterior (4 subdivisions) + Posterior (2 subdivisions), boundaries and key contents
- Deep Cervical Fascia - 3 layers + carotid sheath, the "danger space" (alar-prevertebral), spread of infection
- Black Eye - Clinical approach, must-not-miss diagnoses (panda eyes = basal skull fracture)
Scalp detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
All the data and diagrams are ready. Here is the complete detailed scalp anatomy guide:
🧠 The Scalp - Detailed Anatomy
Extent / Boundaries of the Scalp
The scalp covers the calvaria (dome of skull) and extends:
- Anteriorly: Superciliary arches (supraorbital margins)
- Posteriorly: External occipital protuberance + superior nuchal lines
- Laterally: Zygomatic arches + external acoustic meatus
Layers of the Scalp - S.C.A.L.P.
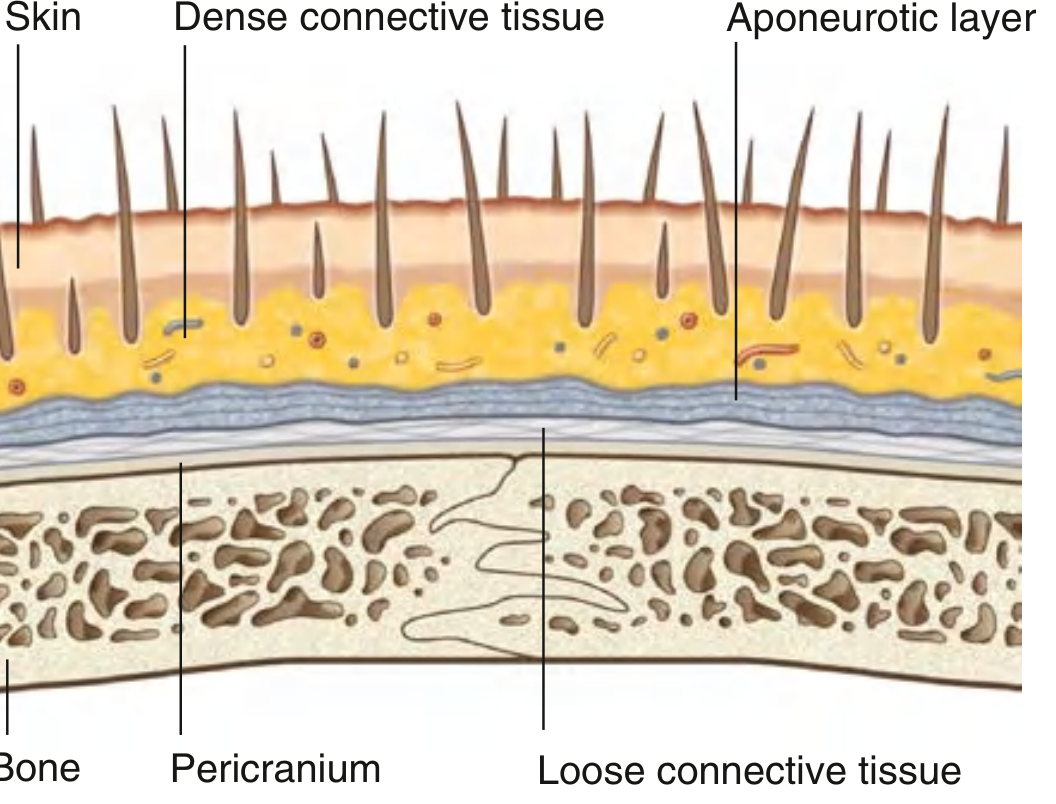
Layer 1 - S = Skin
- Thickest skin in the body: 3 mm (vertex) to 8 mm (occiput)
- Contains hair follicles, sebaceous glands, sweat glands
- Functions as barrier against external environment and pathogens
- Endocrine function: synthesis of Vitamin D
Layer 2 - C = Connective Tissue (Dense)
- Also called superficial fascia or subcutaneous tissue
- Most vascular layer - contains arteries, veins and nerves of the scalp
- The dense fibrous septa tether the vessels in this layer - so when cut, vessels CANNOT retract
- This is the main reason scalp lacerations bleed profusely - arteries remain held open by surrounding fibrous tissue
- Also, in the erect position, venous pressure is extremely low, so most bleeding is arterial
Exam Point: Bleeding from scalp wounds is predominantly arterial - vessels don't retract because they are tethered by the fibrous connective tissue.
Layer 3 - A = Aponeurotic Layer (Galea Aponeurotica / Epicranial Aponeurosis)
- The galea aponeurotica is a flat, tough, fibrous tendon connecting two muscles:
- Anteriorly: Frontalis muscle (frontal belly of occipitofrontalis)
- Posteriorly: Occipitalis muscle (occipital belly of occipitofrontalis)
- Laterally, the galea blends with the SMAS (Superficial Musculo-Aponeurotic System) of the face and temporoparietal fascia
The Occipitofrontalis Muscle:
- Frontal belly - attached to skin of eyebrows; moves upward across forehead; wrinkles forehead and raises eyebrows
- Occipital belly - arises from lateral superior nuchal line and mastoid process
- Motor supply:
- Frontal belly → Temporal branch of CN VII (facial nerve)
- Occipital belly → Posterior auricular branch of CN VII
Exam Point: The first 3 layers (S + C + A) are tightly bound together and move as a single unit - called the "Scalp Proper." This is the tissue torn away in "scalping" injuries.
Layer 4 - L = Loose Areolar Connective Tissue (LACT)
⚠️ THE DANGEROUS LAYER / DANGER ZONE OF SCALP
Why "dangerous?"
-
Contains emissary veins - these are valveless veins connecting:
- Scalp veins → Diploic veins → Intracranial dural venous sinuses
- No valves = retrograde flow possible → infection spreads from scalp to meninges
- Can cause: meningitis, subdural empyema, cavernous sinus thrombosis
-
Loose consistency - pus and blood can accumulate freely and spread widely across the whole skull in this plane
-
Allows movement - the scalp proper (layers 1-3) slides freely over the pericranium through this layer
-
Surgical plane - used for elevation of scalp flaps in craniofacial/neurosurgery (relatively avascular plane)
Layer 5 - P = Pericranium (Periosteum)
- Periosteum of the outer surface of the calvaria
- Firmly adherent to bones but can be stripped from the bone surface
- Firmly attached at suture lines - this is why subperiosteal collections (e.g., cephalohematoma) do NOT cross suture lines
- Provides a small amount of blood supply to the outer skull
Comparison of Scalp Space Pathologies
| Condition | Layer / Space | Crosses Suture Lines? | Notes |
|---|---|---|---|
| Caput Succedaneum | Layer 2 (connective tissue) | YES | Edema/hematoma in SQ tissue; neonatal head molding during delivery |
| Subgaleal Hematoma | Layer 4 (loose areolar tissue) | YES | Large, dangerous; can extend widely over whole calvaria; life-threatening blood loss in neonates |
| Cephalohematoma | Subperiosteal (deep to Layer 5) | NO | Contained by periosteum at suture lines; takes weeks to resolve |
Mnemonic (Neonatal scalp collections from superficial to deep): Capt Succedaneum (C for connective tissue) → Subgaleal (S for subaponeurotic) → Cephalohematoma (C for subperiosteal - Cranium)
Arterial Supply of the Scalp
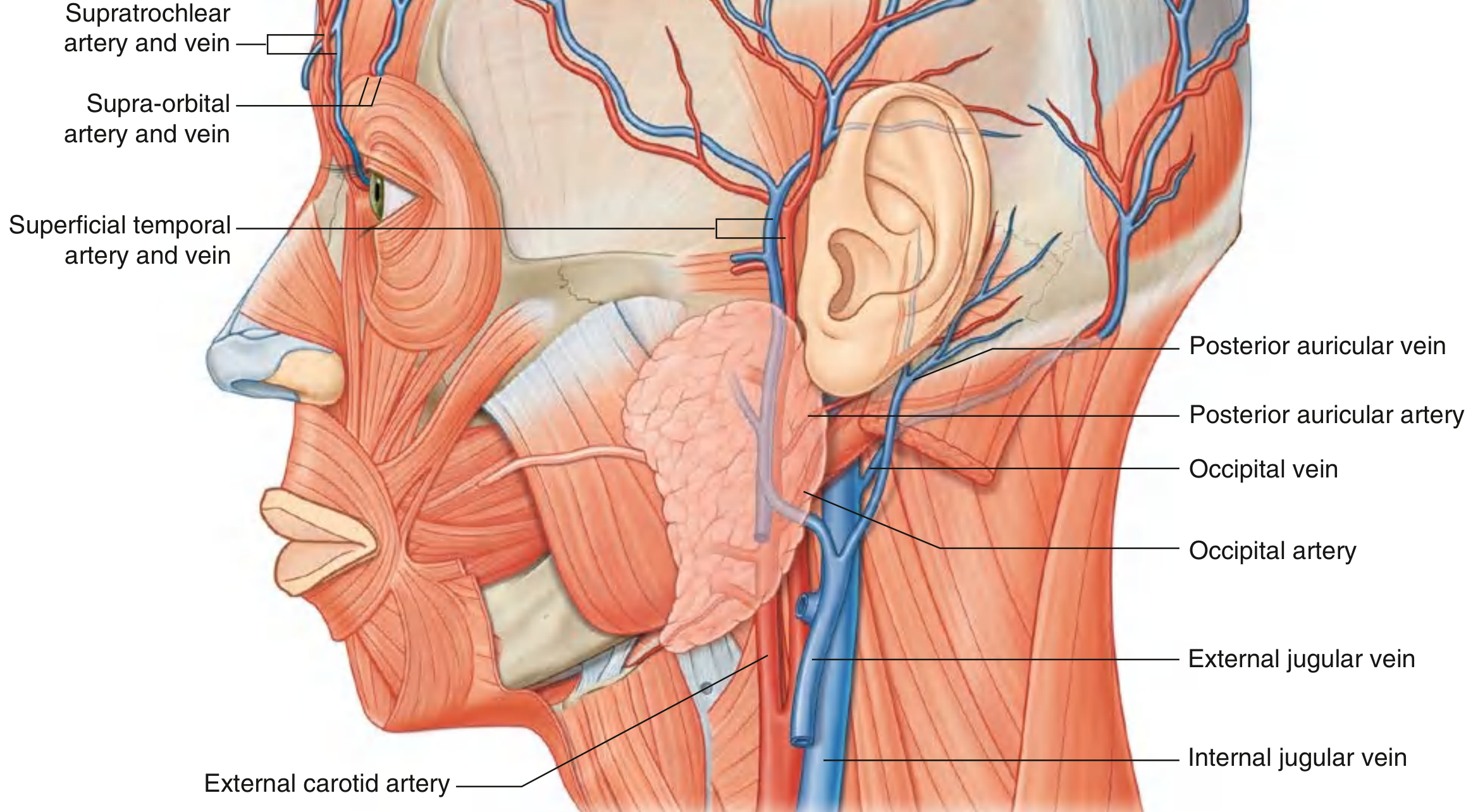
Two main sources: External Carotid Artery (ECA) + Internal Carotid Artery (ICA via ophthalmic artery)
| Artery | Origin | Region Supplied |
|---|---|---|
| Supratrochlear artery | Ophthalmic a. (ICA) | Anterior forehead near midline |
| Supra-orbital artery | Ophthalmic a. (ICA) | Anterior scalp to vertex |
| Superficial temporal artery | Terminal branch of ECA | Entire lateral scalp (largest supply); palpable anterior to ear/tragus |
| Posterior auricular artery | ECA (posterior) | Scalp posterior to the ear |
| Occipital artery | ECA (posterior) | Posterior scalp (large area) |
Exam Tip: The scalp arteries anastomose freely with each other and across the midline - this is why scalp flaps survive even when based on one arterial pedicle, and why scalp bleeding is hard to control.
Anatomical Rule: All scalp vessels run in Layer 2 (dense connective tissue) and approach from the periphery upward toward the vertex.
Venous Drainage of the Scalp
Follows the same pattern as arteries (companion veins):
- Supratrochlear + Supra-orbital veins → angular vein → facial vein
- Superficial temporal vein → retromandibular vein
- Posterior auricular vein → tributary of retromandibular vein
- Occipital vein → suboccipital venous plexus
Additionally, all scalp veins communicate with intracranial dural sinuses via emissary veins through Layer 4 (the dangerous layer).
Nerve Supply (Sensory Innervation)

Dividing line: A line from the posterior ear → vertex → opposite posterior ear
- Anterior to this line → Trigeminal Nerve (CN V) branches
- Posterior to this line → Cervical Nerve branches (C2, C3)
Anterior (Trigeminal - CN V):
| Nerve | Branch of | Area Supplied |
|---|---|---|
| Supratrochlear | CN V1 (ophthalmic) | Medial forehead near midline |
| Supra-orbital | CN V1 (ophthalmic) | Forehead to vertex |
| Zygomaticotemporal | CN V2 (maxillary) | Small anterior temple area |
| Auriculotemporal | CN V3 (mandibular) | Temporal scalp + anterior to ear to near vertex |
Posterior (Cervical Nerves C2, C3):
| Nerve | Origin | Area Supplied |
|---|---|---|
| Greater Occipital nerve | Posterior ramus of C2 | Large posterior scalp up to vertex - MOST IMPORTANT |
| Lesser Occipital nerve | Anterior ramus of C2 (cervical plexus) | Posterior and superior to ear |
| Great Auricular nerve | Anterior rami of C2+C3 (cervical plexus) | Small area posterior to ear |
| Third Occipital nerve | Posterior ramus of C3 | Small lower posterior scalp area |
Motor Supply:
- Occipitofrontalis muscle → CN VII (facial nerve)
- Frontal belly → Temporal branches of CN VII
- Occipital belly → Posterior auricular branch of CN VII
Lymphatic Drainage of the Scalp
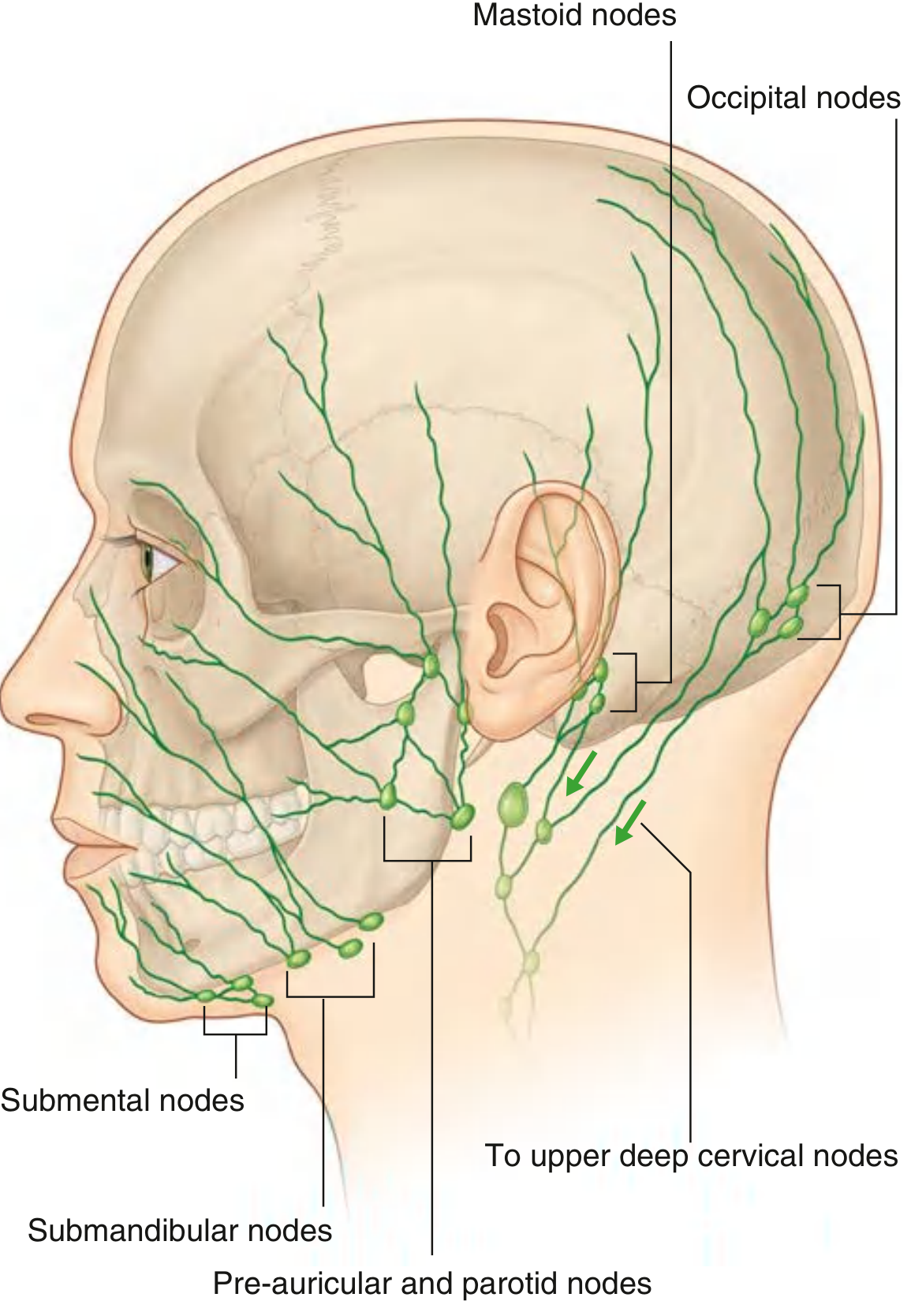
Lymphatics follow the arterial distribution pattern, draining to a "ring" of nodes around the base of the skull:
| Region of Scalp | Primary Nodes | Secondary Nodes |
|---|---|---|
| Posterior scalp (occiput) | Occipital nodes | Upper deep cervical nodes |
| Posterior to vertex | Mastoid nodes (retroauricular) | Upper deep cervical nodes |
| Anterior to vertex / temporal | Pre-auricular and parotid nodes | Upper deep cervical nodes |
| Forehead | Submandibular nodes (via facial artery) | Deep cervical nodes |
All eventually drain to the upper deep cervical lymph nodes.
Clinical Summary - Exam High Yield Points
| Point | Detail |
|---|---|
| Scalp mnemonic | S-C-A-L-P |
| Scalp proper | First 3 layers (S+C+A) move together |
| Profuse bleeding | Due to dense CT holding vessels open + arterial bleed |
| Dangerous layer | Layer 4 (Loose areolar) - valveless emissary veins |
| Emissary veins | Scalp → diploic veins → dural sinuses (no valves!) |
| Infection spread | Layer 4 → meningitis, cavernous sinus thrombosis |
| Cephalohematoma | Subperiosteal - does NOT cross suture lines |
| Subgaleal hematoma | Layer 4 - DOES cross suture lines - massive blood loss |
| Caput succedaneum | Layer 2 - crosses sutures - resolves fast |
| Sensory nerve | Anterior = CN V; Posterior = C2, C3 |
| Most important posterior nerve | Greater occipital nerve (C2 posterior ramus) |
| Motor to scalp muscles | CN VII (facial nerve) |
| Arterial supply | 5 arteries: 2 from ICA (ophthalmic), 3 from ECA |
| Veins | Drain to emissary veins → dural sinuses |
| Lymph drainage | Ring of nodes at skull base → deep cervical nodes |
Sources: Gray's Anatomy for Students, Scott-Brown's Otorhinolaryngology, Roberts & Hedges' Clinical Procedures in Emergency Medicine, Rosen's Emergency Medicine
Scalp
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.