Type 1 diabetes symptoms diagnosis treatment
Reading File
Finding Sources
Searching PubMed
"type 1 diabetes"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Searching PubMed
"type 1 diabetes" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced content to write a detailed answer. Let me compile everything.
Type 1 Diabetes Mellitus (T1DM)
Pathophysiology
Type 1 diabetes (previously called insulin-dependent diabetes) accounts for approximately 5-10% of all diabetes cases, with a peak onset at 11-12 years of age, though it can occur at any age. It is caused by autoimmune destruction of the insulin-producing beta (β) cells in the islets of Langerhans in the pancreas, resulting in absolute insulin deficiency.
The disease process involves multiple immune mechanisms:
- CD4+ Th1 cells reactive to islet antigens (including insulin)
- Cytotoxic T lymphocyte (CTL)-mediated lysis of islet cells
- Local production of cytokines (TNF and IL-1) damaging islet cells
- Autoantibodies against islet cells and insulin
The pathological lesion seen in the islets is called insulitis (cellular necrosis with lymphocytic infiltration of CD4+ and CD8+ T cells). Critically, 90% or more of islets must be destroyed before clinical manifestations appear, explaining the long preclinical phase.
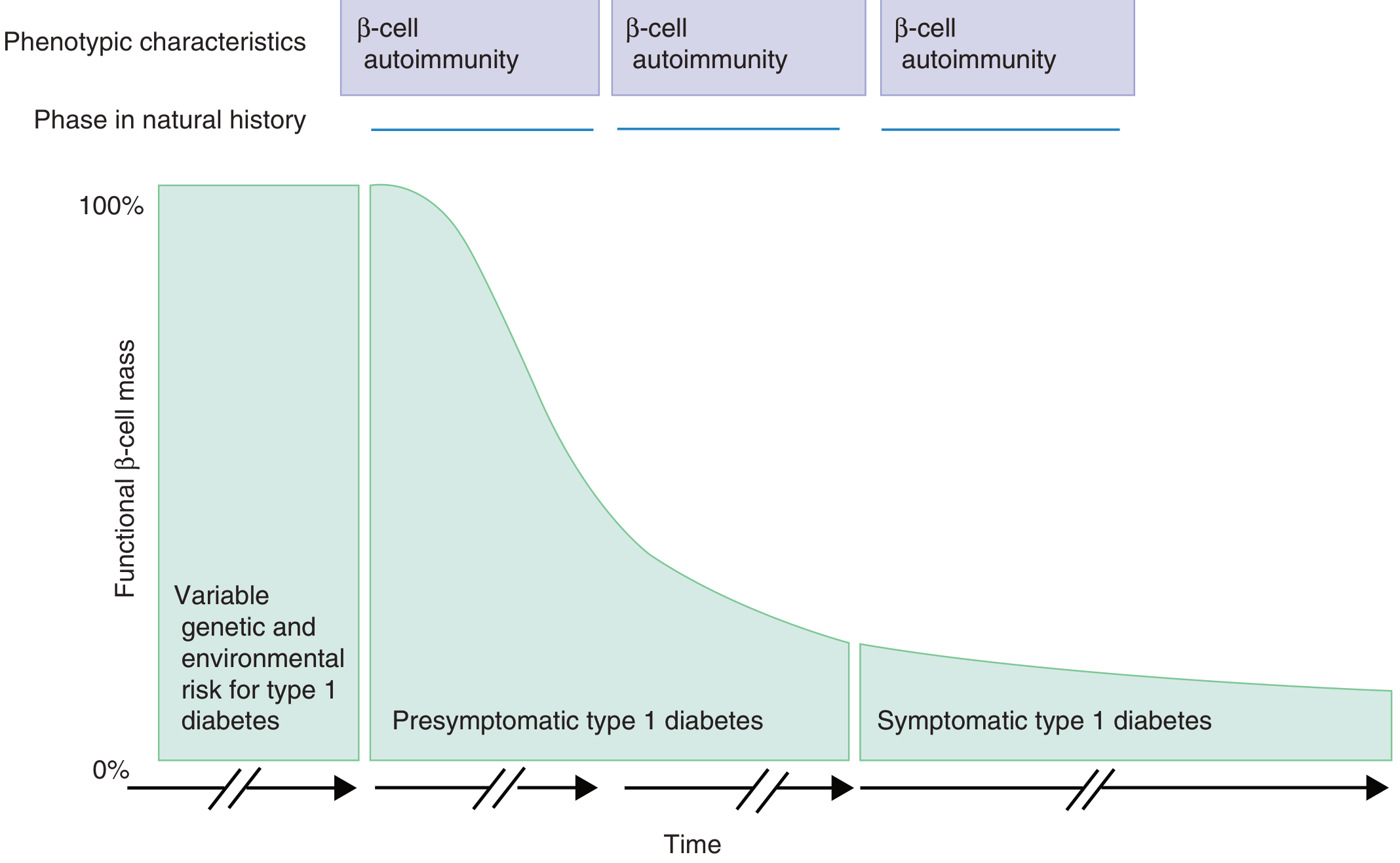
The diagram above shows how β-cell autoimmunity occurs long before symptoms appear. Clinical disease emerges only when functional β-cell mass falls near zero. (Goldman-Cecil Medicine)
Genetic factors: 90-95% of Caucasians with T1DM carry HLA-DR3 or DR4 (or both), vs. ~40% of healthy subjects. HLA-DQ alleles may be the actual disease-associated genes. Non-HLA genes - including insulin gene promoter polymorphisms and IL-2/CD25 polymorphisms - also contribute. Environmental triggers such as coxsackievirus B4 infection have been implicated.
Symptoms
The classic presentation is in a lean patient younger than 40 (often a child, adolescent, or young adult). Onset can be abrupt:
| Symptom | Mechanism |
|---|---|
| Polyuria | Osmotic diuresis from hyperglycemia |
| Polydipsia | Response to fluid losses |
| Polyphagia | Cells unable to use glucose; starvation signal |
| Weight loss | Catabolism of fat and protein (no insulin anabolism) |
| Fatigue | Impaired cellular glucose uptake |
| Blurred vision | Osmotic changes in the lens |
In some cases the disease first presents as diabetic ketoacidosis (DKA) - this is more common in children under age 5 and in low/middle-income countries, where 13-80% of first T1DM presentations worldwide are DKA. At the time of clinical diagnosis, about 10-20% of the original β-cell mass may still be functional.
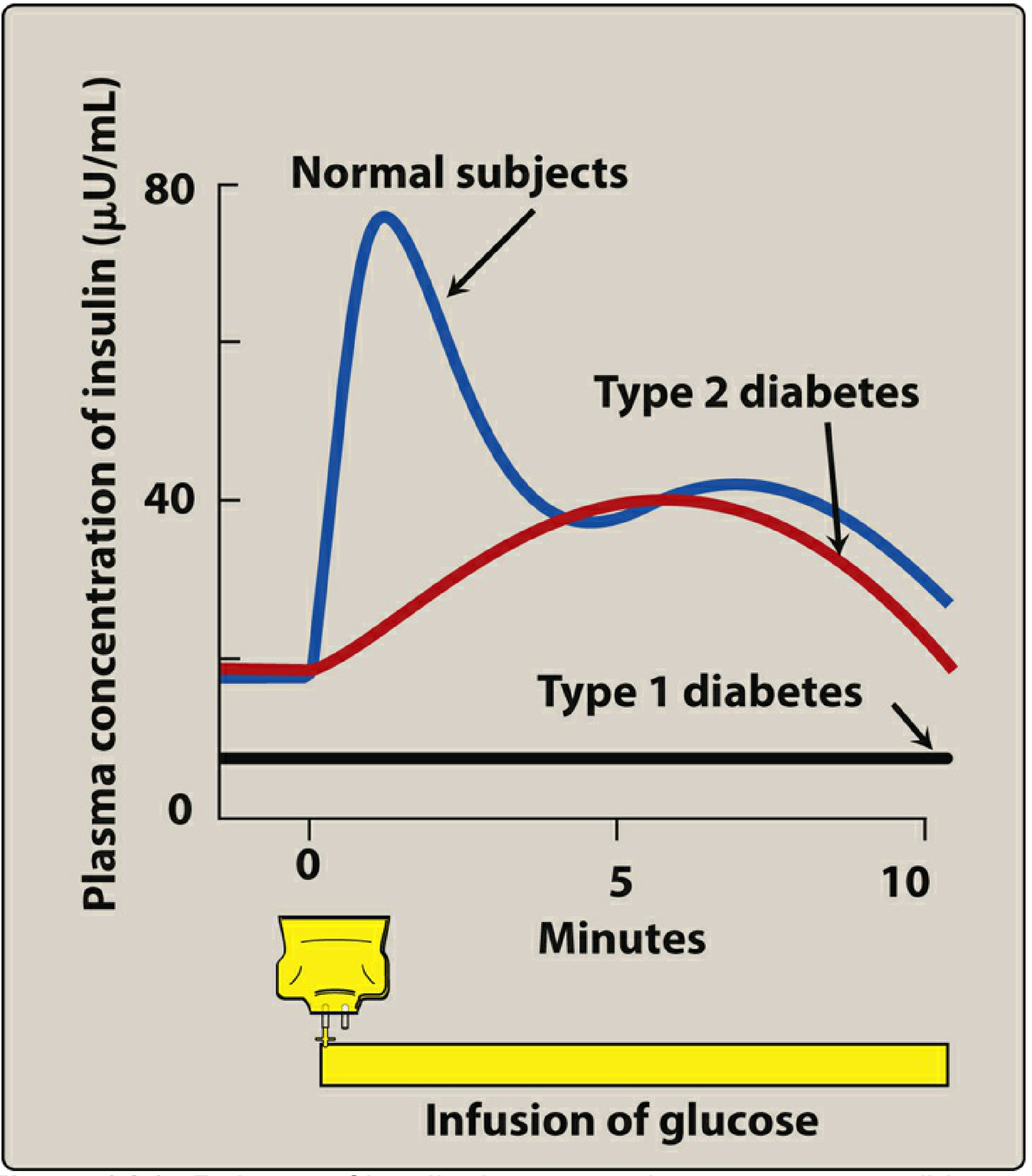
Type 1 diabetes produces essentially zero insulin response to a glucose load (flat black line). In normal subjects (blue), there is a sharp first-phase release within minutes. (Lippincott Illustrated Reviews: Pharmacology)
Chronic Complications
Long-standing hyperglycemia leads to:
- Macrovascular: Atherosclerosis, coronary artery disease, peripheral artery disease
- Microvascular: Diabetic retinopathy, nephropathy, peripheral neuropathy
- Other: Foot ulcers, recurrent infections, skin lesions, autonomic neuropathy
Diagnosis
The ADA diagnostic criteria for diabetes (any type) are:
| Criterion | Threshold |
|---|---|
| Random plasma glucose + symptoms | ≥200 mg/dL |
| Fasting plasma glucose (8-hour fast) | ≥126 mg/dL (confirmed on repeat) |
| 2-hour post-75g OGTT | ≥200 mg/dL |
| HbA1c | ≥6.5% |
If symptoms are absent, any single abnormal glucose result must be confirmed by repeat testing. - Miller's Anesthesia, 10e
Distinguishing T1DM from T2DM
Several markers help:
- Pancreatic autoantibodies - present in T1DM; markers include:
- Anti-GAD65 (glutamic acid decarboxylase) - highest sensitivity (91%) as single screening marker
- Anti-insulin (IAA) - more common in young children
- Anti-IA-2 (tyrosine phosphatase)
- Anti-ZnT8 (zinc transporter 8)
- Detection of ≥2 autoantibodies significantly increases prediction of T1DM development
- C-peptide - very low or undetectable in T1DM (reflects absent endogenous insulin)
- Clinical profile: Lean, young, prone to ketosis, absolute insulin requirement
"The presence or absence of anti-GAD65 or other antibodies is sometimes helpful to distinguish between type 1 and type 2 diabetes and to guide appropriate treatment if the diagnosis is in doubt." - Goldman-Cecil Medicine
"Honeymoon Phase"
After starting insulin, many patients experience weeks to months of easily controlled hyperglycemia due to partial remaining β-cell function. This fades as autoimmune destruction continues.
LADA (Latent Autoimmune Diabetes in Adults)
In some adults, T1DM follows a more indolent course and may initially be misdiagnosed as T2DM until progressive insulin deficiency reveals the T1DM phenotype.
Treatment
Core Principle
All patients with T1DM require exogenous insulin - without it, they will develop DKA. The goal is to maintain glucose in the physiologic range and prevent short- and long-term complications.
Glycemic Targets (ADA):
- HbA1c < 7% (most non-pregnant adults)
- Fasting glucose: 80-130 mg/dL
- Post-prandial glucose: <180 mg/dL
- Time-in-range (CGM): >70% of time between 70-180 mg/dL
Insulin Regimens
Total daily dose: 0.3-1.0 unit/kg/day for adults, with ~half given as basal and the remainder split as pre-meal boluses.
Insulin Types
| Type | Examples | Onset | Duration | Use |
|---|---|---|---|---|
| Rapid-acting analogues | Lispro, Aspart, Glulisine | 10-20 min | 3-5 hr | Mealtime bolus |
| Regular (short-acting) | Regular human insulin | 30-60 min | 6-8 hr | Mealtime |
| Intermediate-acting | NPH | 1-2 hr | 12-18 hr | Background |
| Long-acting analogues | Glargine, Detemir, Degludec | 1-2 hr | 20-24+ hr | Basal |
Basal-bolus regimen (multiple daily injections, MDI) is the standard - long-acting insulin once or twice daily, plus rapid-acting insulin before each meal. Prandial doses are adjusted using an insulin-to-carbohydrate ratio plus a correction factor (e.g., 1 unit of rapid insulin per 15g carbohydrate, with 1 unit correcting ~50 mg/dL of excess glucose).
Insulin Pump (Continuous Subcutaneous Insulin Infusion, CSII)
Insulin pumps deliver rapid-acting insulin via a subcutaneous catheter at a programmed variable basal rate, with on-demand boluses. Benefits vs. MDI:
- Reduces HbA1c by 0.3-0.5%
- Reduces severe hypoglycemia
- More flexible lifestyle
- Programmable basal rate variability (especially useful for the dawn phenomenon)
Sensor-augmented pumps (with CGM integration) reduce HbA1c by -0.4 to -0.6% and reduce hypoglycemia compared to MDI.
Closed-loop / Automated Insulin Delivery (AID) systems combine real-time CGM with an insulin control algorithm that automatically adjusts insulin delivery - the "artificial pancreas."
Monitoring
- HbA1c every 3 months - reflects average glucose over prior 3 months
- Self-monitoring blood glucose (SMBG) - fingerstick before meals and at bedtime
- Continuous glucose monitors (CGMs) - interstitial glucose every 5 minutes, glucose trend arrows, alarms for hypo/hyperglycemia
- Urine/capillary ketones - check when glucose is unexpectedly elevated; moderate/large ketones (≥2+ or >1.5 mmol/L) signal impending DKA
Additional Management
- DKA management: IV fluids, insulin infusion, electrolyte replacement (especially potassium)
- Hypoglycemia treatment: 15-20g fast-acting carbohydrate (glucose tablets, juice) for mild episodes; glucagon injection or IV dextrose for severe episodes
- Screening for complications: Annual ophthalmology exam, urine albumin/creatinine ratio, lipid panel, blood pressure monitoring, foot exam
- Immunotherapy (emerging): Teplizumab (anti-CD3 antibody) was approved in 2022 to delay onset of clinical T1DM in at-risk individuals with 2+ autoantibodies - this represents a new disease-modifying approach. A 2025 Lancet review outlines further emerging therapies including beta-cell replacement and antigen-specific immunotherapy.
- Multidisciplinary care: Endocrinologist, diabetes educator, dietitian, and - for pediatric patients - pediatric diabetes team
Sources: Rosen's Emergency Medicine, 9e | Goldman-Cecil Medicine, International Edition | Lippincott Illustrated Reviews: Pharmacology | Miller's Anesthesia, 10e | Henry's Clinical Diagnosis and Management by Laboratory Methods | Cellular and Molecular Immunology
This is a shared conversation. Sign in to Orris to start your own chat.