Mechanism of acidification of urine renal physiology detailed explanation in simple way with flowcharts
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from authoritative sources. Let me compose the full, detailed answer with embedded diagrams.
Mechanism of Urine Acidification - Renal Physiology
The kidney is the final defender of acid-base balance. It maintains blood pH ~7.4 by excreting ~70 mEq of fixed (non-volatile) acid every day, progressively acidifying the filtrate from pH 7.4 down to as low as pH 4.4 in the collecting duct.
Overview Flowchart
Dietary metabolism
↓
Fixed acids produced (H2SO4, H3PO4, organic acids)
↓
Buffered by plasma HCO3⁻ → HCO3⁻ consumed
↓
Kidney must:
1. Reclaim all filtered HCO3⁻ (proximal tubule)
2. Excrete daily H⁺ load (buffered by phosphate + ammonia)
↓
Result: Urine pH drops from 7.4 → 4.4–6.0
The Three Core Mechanisms
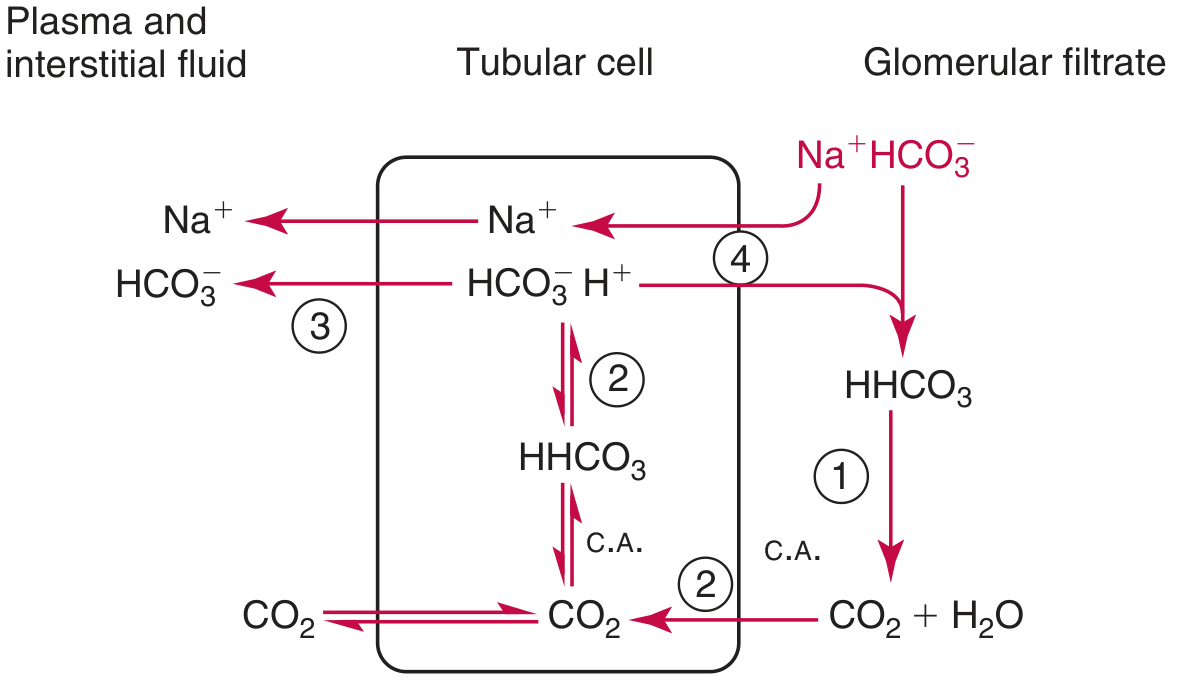
1. Bicarbonate Reclamation (Proximal Tubule)
This does not excrete acid but prevents bicarbonate loss. ~4,300 mEq of HCO3⁻ is filtered daily - virtually all must be reclaimed.
TUBULAR LUMEN PROXIMAL TUBULE CELL BLOOD
Na⁺ + HCO3⁻ ──────→ H⁺ secreted by NHE3 HCO3⁻ exits
↕ (Na⁺/H⁺ exchanger) via NBC-1
H⁺ + HCO3⁻ → H2CO3
↓ (Carbonic Anhydrase IV, brush border)
CO2 + H2O
↓ (diffuses into cell)
CO2 + OH⁻ → HCO3⁻ (Carbonic Anhydrase II)
↓
HCO3⁻ → exits to blood via NBC-1
H⁺ → secreted again by NHE3
Key point: H⁺ secreted here recombines with filtered HCO3⁻ to form CO2 + H2O - so the luminal pH barely falls. This is reclamation, not new acid excretion. - National Kidneys Foundation Primer on Kidney Diseases, 8e
Here is the diagram from Tietz Textbook showing bicarbonate reclamation:
2. H⁺ Secretion and Urinary Buffering (Distal Tubule + Collecting Duct)
This is where true acidification happens. The luminal pH progressively falls from ~6.5 in the distal tubule to 4.4 in the medullary collecting duct.
The α-Intercalated Cell (the star player)
COLLECTING DUCT LUMEN α-INTERCALATED CELL BLOOD
H2O ──→ H⁺ + OH⁻
OH⁻ + CO2 → HCO3⁻ (via CA II)
↓
H⁺ ←────────────────────── H⁺-ATPase (apical)
(acidifies urine)
HCO3⁻ ──→ exits via
Cl⁻/HCO3⁻ exchanger
(AE1, band 3) → HCO3⁻ to blood
For every H⁺ secreted into the urine, one HCO3⁻ is added back to the blood, replenishing what was used to buffer dietary acids. - NKF Primer on Kidney Diseases, 8e
Limit: Free H⁺ alone could only carry 0.04 mEq/L at pH 4.4 - you would need 1,750 L of urine to excrete 70 mEq daily! So two urinary buffers do the heavy lifting:
2a. Titratable Acid (Phosphate Buffer)
In tubular lumen:
HPO4²⁻ (dibasic, filtered) + H⁺ → H2PO4⁻ (monobasic, excreted)
(pKa = 6.8) (this is "titratable acid")
Net result:
- ~30 mEq H⁺/day excreted this way
- 1 HCO3⁻ generated and returned to blood for each H⁺ buffered
The pKa of 6.8 means ~90% of its buffering capacity works above urine pH 5.8 - making it very effective in the distal tubule. - Tietz Textbook of Laboratory Medicine, 7e
2b. Ammonium Buffer (NH4⁺) - the most important and regulatable
This is the system the kidney upregulates in acidosis (can go from 30-40 mEq/day up to 200 mEq/day).
Step 1 - Ammonia synthesis in proximal tubule cells:
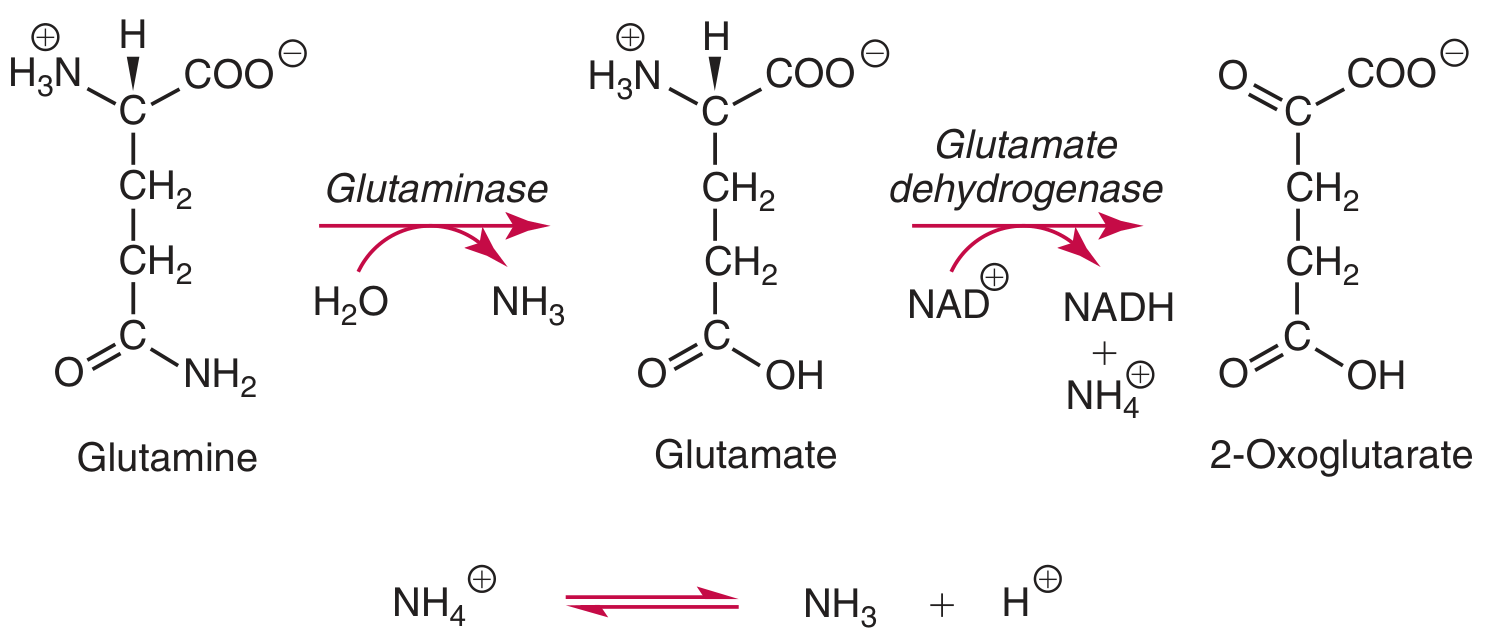
Glutamine (from muscle/liver)
↓ Glutaminase
Glutamate + NH4⁺
↓ Glutamate dehydrogenase
α-ketoglutarate + NH4⁺
↓
NH4⁺ ⇌ NH3 + H⁺
- Produces 2 NH4⁺ + 2 HCO3⁻ per glutamine
- The new HCO3⁻ goes to blood to replace what was lost in buffering
Step 2 - NH4⁺ transport through the loop:
Proximal tubule: NH4⁺ secreted into lumen
↓
Thick ascending limb (TAL):
NH4⁺ substitutes for K⁺ on NKCC2 cotransporter
→ NH4⁺ reabsorbed into medullary interstitium
→ NH4⁺ ⇌ NH3 + H⁺ (interstitium is less acid, favors NH3)
↓
Medullary interstitium: high [NH3]
Step 3 - NH3 "trapping" in the collecting duct (the key acidification step):
Medullary interstitium Inner Medullary Collecting Duct
[NH3] high ──────────────────────→ NH3 (enters via RhCG protein)
↓
NH3 + H⁺ → NH4⁺
(H⁺ comes from H⁺-ATPase of α-ICs)
↓
NH4⁺ TRAPPED (can't cross membrane)
↓
Excreted in urine as NH4Cl, etc.
At urine pH 5.0: ratio of NH3 : NH4⁺ = 1 : 10,000 → virtually all is NH4⁺ and cannot escape. - Tietz Textbook of Laboratory Medicine, 7e; NKF Primer, 8e
Complete Integrated Diagram (Tietz Textbook)
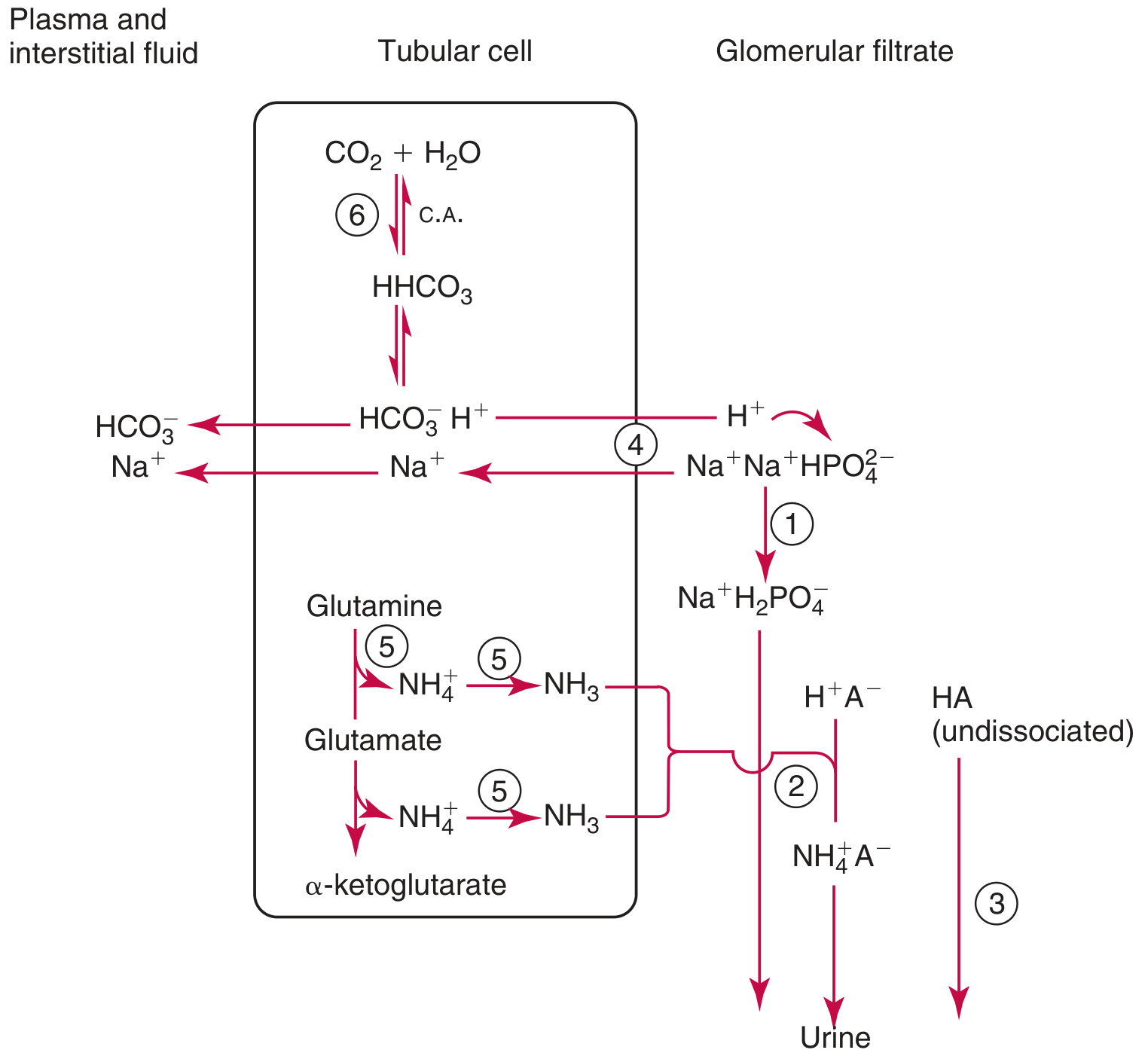
This diagram shows all 6 steps together in the tubular cell.
Summary Table: Three Routes of H⁺ Excretion
| Mechanism | Amount (normal) | Maximum (acidosis) | Where | Buffer |
|---|---|---|---|---|
| Free H⁺ | Tiny (<1 mEq/day) | Limited by pH 4.4 | Collecting duct | None |
| Titratable Acid (H2PO4⁻) | ~30 mEq/day | ~30-40 mEq/day | Proximal + distal | HPO4²⁻ |
| Ammonium (NH4⁺) | ~30-40 mEq/day | ~200 mEq/day | Proximal → TAL → CD | NH3 |
Key Regulatory Points
Acidosis triggers:
├── ↑ NHE3 activity (more H⁺ secreted proximally)
├── ↑ H⁺-ATPase on α-intercalated cells
├── ↑ Glutamine uptake → ↑ NH4⁺ synthesis
├── ↑ Phosphate filtered (if acidemia worsens)
└── ↑ Angiotensin II → ↑ proximal NHE3 (if low EABV)
Alkalosis triggers:
├── ↓ H⁺ secretion
├── ↑ β-intercalated cells → secrete HCO3⁻ into lumen
└── ↑ Urinary citrate excretion
Potassium-H⁺ Interaction (Clinically Important!)
Hyperkalemia → K⁺ competes with H⁺ in NHE3 → less H⁺ secreted
→ less acidification → body fluid MORE acid
→ Metabolic ACIDOSIS
Hypokalemia → More H⁺ secreted instead of K⁺
→ more acidification → body fluid MORE alkaline
→ Metabolic ALKALOSIS
- Tietz Textbook of Laboratory Medicine, 7e
Nephron Segment Summary
Glomerulus
↓ Filtrate pH = 7.4, contains 4300 mEq HCO3⁻/day
Proximal Tubule (PCT)
↓ NHE3 reclaims ~85% of filtered HCO3⁻
↓ Ammoniagenesis from glutamine begins
Loop of Henle (TAL)
↓ NH4⁺ reabsorbed via NKCC2, builds medullary [NH3]
Distal Convoluted Tubule
↓ Further H⁺ secretion, pH begins to fall significantly
Collecting Duct (α-intercalated cells)
↓ H⁺-ATPase + H⁺-K⁺-ATPase secrete H⁺
↓ Phosphate → H2PO4⁻ (titratable acid)
↓ NH3 enters → trapped as NH4⁺ (ion trapping)
↓ MINIMUM urine pH = 4.4
Final Urine: pH 4.4–6.0
Sources:
- NKF Primer on Kidney Diseases, 8e - Sections: Urinary Acidification, H⁺ Secretion, Titratable Acid, Ammonium Excretion
- Tietz Textbook of Laboratory Medicine, 7e - Section: Renal Mechanisms in the Regulation of Acid-Base Balance (Figs. 50.12, 50.13, 50.14)
- Tietz Laboratory Medicine - Na⁺/H⁺ Exchange, Ammonia production, HCO3⁻ reclamation
This is a shared conversation. Sign in to Orris to start your own chat.