Metformin ●Biguanide ●Insulin sensitizing effect. Exact mechanism unclear ●Safety record spans several decades ●First medication to be used in T2DM and prediabetes ●Should be continued for as long as possible – alone or in combination with other medications for treatment intensification ●Side effects: GI intolerance ●Contraindications for use: kidney disease or liver disease.
Reading File
Finding Sources
Finding Sources
Searching PubMed
metformin type 2 diabetes mechanism
Reading File
Reading File
Loading Image
Here is a detailed, textbook-grounded expansion of the Metformin notes you provided:
Metformin - Expanded Review
Drug Class: Biguanide
Metformin is the only biguanide in clinical use. It is the most widely prescribed antidiabetic medication worldwide. - Lippincott Illustrated Reviews: Pharmacology
Mechanism of Action (Insulin-Sensitizing)
The note states the exact mechanism is "unclear" - this is accurate and worth understanding:
Primary mechanism: Reduction of hepatic gluconeogenesis (liver glucose output). This is why metformin primarily lowers fasting blood glucose, since excess overnight hepatic glucose production is the main driver of elevated fasting glucose in T2DM.
Additional mechanisms:
- Slows intestinal absorption of sugars
- Improves peripheral glucose uptake and utilization (insulin sensitization in muscle and fat)
- Does NOT stimulate insulin secretion - this is pharmacologically important
Molecular target (the "unclear" part): Metformin activates AMPK (AMP-activated protein kinase) in the liver, which suppresses gluconeogenesis. However, studies suggest AMPK-independent pathways also exist (inhibition of mitochondrial complex I, changes in AMP:ATP ratio), which is why the full mechanism remains an area of ongoing research.
Metformin's mechanism also has anti-aging implications via AMPK/mTOR signaling, which is the subject of current research. - Brenner & Rector's The Kidney
Position in T2DM & Prediabetes
- First-line for T2DM: initiated at diagnosis, with or without lifestyle modification
- Prediabetes: delays or prevents progression to T2DM
- Combination therapy: continues as the backbone when additional agents (SGLT2i, GLP-1 RA, sulfonylureas, etc.) are added
- HbA1c reduction: approximately 1.0-1.5% (11-16 mmol/mol) - Goldman-Cecil Medicine
- Also useful in PCOS (polycystic ovary syndrome) - addresses insulin resistance, restores ovulation
Cardiovascular Benefit
A key advantage not always highlighted in basic notes:
- Metformin decreases cardiovascular events and death in obese patients with T2DM (originally demonstrated in the UKPDS trial)
- Does not cause weight gain - may cause modest weight loss due to appetite reduction
- Does not cause hypoglycemia when used as monotherapy (no insulin secretion is stimulated)
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Route | Oral |
| Protein binding | Not bound to serum proteins |
| Metabolism | Not metabolized (excreted unchanged) |
| Elimination | Renal filtration - excreted unchanged in urine |
| Max dose | 2,550 mg/day |
Side Effects (Expanded)
The GI side effects are the most common reason for discontinuation:
- Diarrhea, nausea, vomiting, bloating, metallic taste
- Occur in ~20-30% of patients, especially early in therapy
- Mitigation strategy: Start low (500 mg once or twice daily with meals), titrate slowly
- Extended-release (XR) formulation reduces GI effects significantly
Less common but important:
| Side Effect | Details |
|---|---|
| Lactic acidosis | Rare but potentially fatal; risk increases with renal impairment, hepatic failure, excessive alcohol use, tissue hypoxia |
| Vitamin B12 deficiency | Long-term use reduces ileal absorption of the intrinsic factor-B12 complex; monitor B12 levels periodically, especially if anemia or peripheral neuropathy present |
| Weight loss | Generally considered beneficial; mild appetite suppression |
Contraindications (Expanded from your notes)
Your notes mention "kidney disease or liver disease." The full picture:
Renal Contraindications
- Absolute: eGFR < 30 mL/min/1.73 m² - do not use (lactic acidosis risk)
- Caution/dose limit: eGFR 30-45 - use with caution, limit dose
- Temporary hold: Before IV iodinated contrast procedures (withhold 48 hours)
- Also withhold during: acute MI, sepsis, exacerbation of heart failure, any condition causing acute renal impairment
Other Contraindications/Cautions
| Condition | Reason |
|---|---|
| Severe hepatic disease | Impairs lactate clearance, raising lactic acidosis risk |
| Acute heart failure exacerbation | Reduced renal perfusion |
| Sepsis/critical illness | Tissue hypoxia promotes lactic acidosis |
| Excessive alcohol use | Potentiates lactic acidosis risk |
| Age > 80 years | Caution (renal function often impaired) |
Key Clinical Points to Remember
-
No hypoglycemia risk as monotherapy - because it does NOT stimulate insulin. Hypoglycemia can occur only when combined with insulin or sulfonylureas.
-
Lactic acidosis is the feared rare complication - the kidney contraindication exists to prevent this.
-
Vitamin B12 monitoring is often overlooked in long-term users.
-
Contrast hold rule: Metformin should be temporarily stopped before iodinated contrast procedures and restarted 48 hours after, confirming renal function is stable.
-
PCOS benefit: Often used off-label but well-supported by evidence.
Recent Evidence (2025)
Recent systematic reviews confirm metformin's role extends well beyond glycemic control, including potential anti-cancer, anti-aging, and cardioprotective effects (PMID 41357061, PMID 40555912). These findings reinforce why metformin is kept as background therapy for as long as possible, even as newer agents are added.
Sources: Lippincott Illustrated Reviews: Pharmacology; Goldman-Cecil Medicine, 2-Vol Set; Brenner and Rector's The Kidney
Oral antidaibetes of t2dm
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content for all drug classes. Here is the full, organized review:
Oral Antidiabetic Agents for Type 2 Diabetes Mellitus
Sources: Lippincott Illustrated Reviews: Pharmacology; Goldman-Cecil Medicine; Katzung's Basic & Clinical Pharmacology
Overview: Quick Comparison Table
| Drug Class | Mechanism | Hypoglycemia Risk | Weight Effect |
|---|---|---|---|
| Biguanides (Metformin) | ↓ Hepatic gluconeogenesis | No | ↓ (neutral/loss) |
| Sulfonylureas | ↑ Insulin secretion (β cell) | Yes | ↑ gain |
| Meglitinides | ↑ Insulin secretion (postprandial) | Yes | ↑ gain |
| Thiazolidinediones (TZDs) | Insulin sensitizer (PPARγ) | No | ↑ gain |
| DPP-4 Inhibitors (Gliptins) | ↑ GLP-1 activity → ↑ insulin, ↓ glucagon | Low | Neutral |
| SGLT2 Inhibitors (Gliflozins) | ↑ Urinary glucose excretion | Low | ↓ loss |
| α-Glucosidase Inhibitors | ↓ Carbohydrate digestion (postprandial) | No (monotherapy) | Neutral |
1. Biguanides - Metformin
Drug: Metformin (the only biguanide in use)
Mechanism:
- Primary: reduces hepatic gluconeogenesis (targets fasting glucose)
- Also: ↓ intestinal glucose absorption, ↑ peripheral insulin sensitivity
- Does NOT stimulate insulin secretion
HbA1c reduction: 1.0-1.5%
Adverse effects:
- GI - diarrhea, nausea, vomiting (most common; start low, titrate slowly, take with meals)
- Lactic acidosis (rare but serious)
- Vitamin B12 deficiency (long-term use - monitor levels)
Contraindications: eGFR < 30 mL/min; hepatic failure; acute MI, sepsis, contrast procedures (hold temporarily)
Special advantage: Preferred first-line; weight neutral or mild weight loss; no hypoglycemia risk as monotherapy; cardiovascular mortality benefit in obese T2DM patients
2. Sulfonylureas (Insulin Secretagogues)
Drugs (2nd generation): Glyburide, Glipizide, Glimepiride
Mechanism:
- Block ATP-sensitive K⁺ channels on pancreatic β cells
- This causes membrane depolarization → Ca²⁺ influx → insulin exocytosis
- Effect is glucose-independent (insulin released even without a meal)
HbA1c reduction: ~1.0-1.5%
Adverse effects:
- Hypoglycemia (most important - major risk, especially glyburide)
- Weight gain
- Drug interactions (NSAIDs, warfarin, fluconazole potentiate hypoglycemia; rifampin reduces efficacy)
Important notes:
- Glyburide - highest hypoglycemia risk; avoid in elderly and renal impairment
- Glipizide / Glimepiride - safer in renal dysfunction and elderly patients
- Do NOT combine with meglitinides (overlapping mechanism → severe hypoglycemia)
3. Meglitinides (Short-Acting Secretagogues)
Drugs: Repaglinide, Nateglinide
Mechanism:
- Same target as sulfonylureas (β cell K⁺ channels) but faster onset, shorter duration
- Taken just before each meal - targets postprandial glucose spikes
- Called "postprandial glucose regulators"
Adverse effects:
- Hypoglycemia (but lower risk than sulfonylureas due to short duration)
- Weight gain
- Skip dose if skipping a meal
Metabolism: Via CYP2C8/CYP3A4 (repaglinide) and CYP2C9/CYP3A4 (nateglinide)
4. Thiazolidinediones (TZDs) - Insulin Sensitizers
Drugs: Pioglitazone, Rosiglitazone
Mechanism:
- Agonists of PPARγ (peroxisome proliferator-activated receptor-gamma) - a nuclear transcription factor
- Activates insulin-responsive genes → ↑ insulin sensitivity in adipose tissue, liver, and skeletal muscle
- Require insulin to be present for action; do NOT cause hypoglycemia as monotherapy
Adverse effects:
- Weight gain (subcutaneous fat ↑) + fluid retention → avoid in heart failure
- Osteopenia / fracture risk (especially women)
- Pioglitazone: possible ↑ bladder cancer risk
- Rosiglitazone: boxed warning for ↑ myocardial infarction risk (very limited use now)
- Hepatotoxicity (rare) - monitor LFTs
Pharmacokinetics: Both metabolized by CYP2C8; no renal dose adjustment needed
5. DPP-4 Inhibitors ("Gliptins") - Incretin Enhancers
Drugs: Sitagliptin, Saxagliptin, Linagliptin, Alogliptin
Mechanism:
- Inhibit DPP-4 enzyme, which normally degrades incretins (GLP-1, GIP)
- Result: prolonged GLP-1 activity → glucose-dependent ↑ insulin secretion + ↓ glucagon
- Because action is glucose-dependent, hypoglycemia risk is low
- Weight neutral (unlike GLP-1 agonists, DPP-4 inhibitors do NOT cause satiety/weight loss)
Adverse effects:
- Nasopharyngitis, headache (most common)
- Pancreatitis (rare but serious - monitor)
- Severe joint pain (arthralgia)
- Saxagliptin specifically - ↑ risk of heart failure hospitalizations (use with caution in HF patients)
- Hypersensitivity reactions
Renal dosing: Most require dose adjustment in renal impairment EXCEPT linagliptin (eliminated via bile)
Do NOT combine DPP-4 inhibitors with GLP-1 receptor agonists (overlapping mechanism, ↑ toxicity)
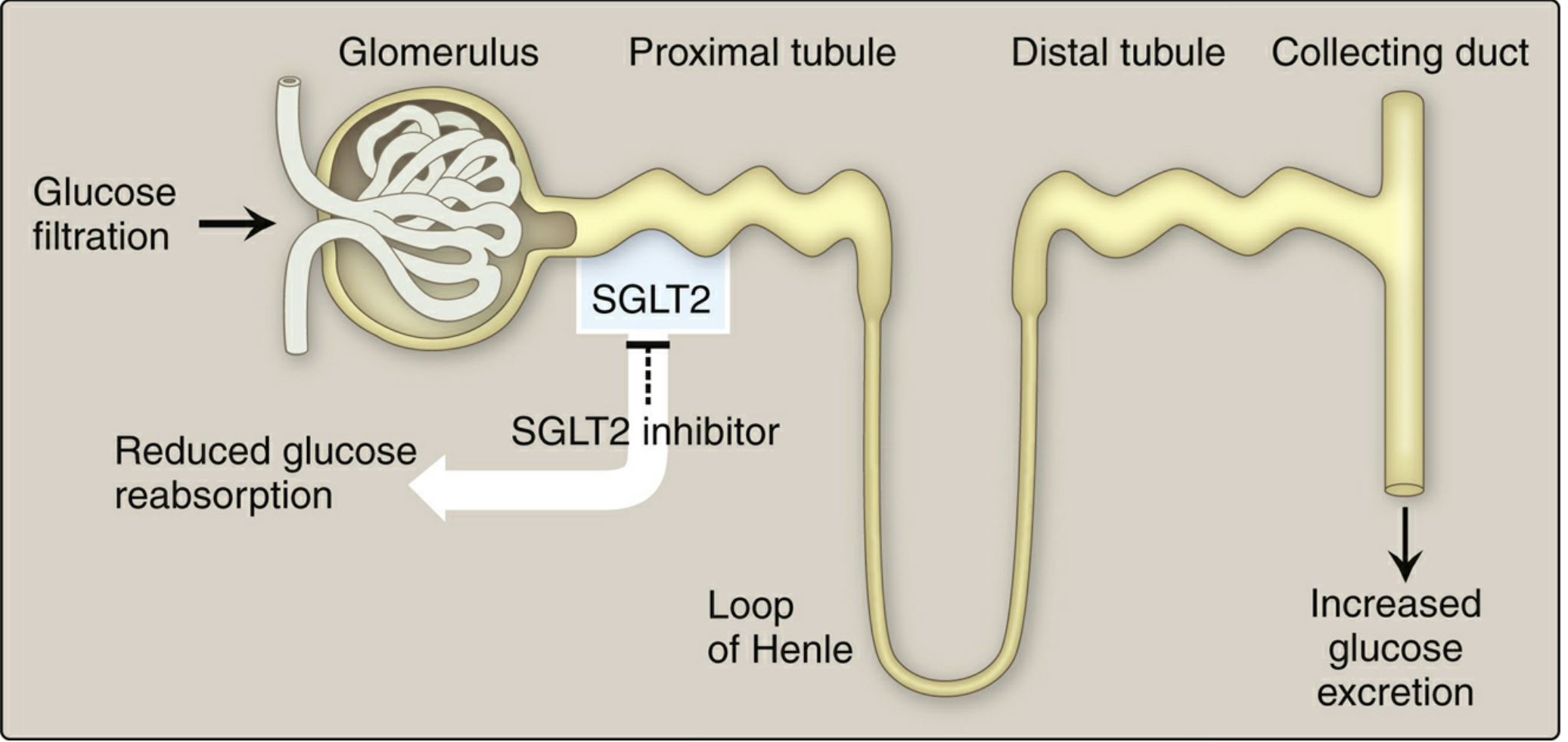
6. SGLT2 Inhibitors ("Gliflozins") - Renal Glucose Excretion
Drugs: Empagliflozin, Canagliflozin, Dapagliflozin, Ertugliflozin
Mechanism:
- Inhibit SGLT2 (sodium-glucose cotransporter 2) in the proximal tubule of the kidney
- Normally SGLT2 reabsorbs ~90% of filtered glucose - blocking it causes glucosuria
- Also causes natriuresis and osmotic diuresis → ↓ BP, ↓ preload
HbA1c reduction: ~0.5-1.0%
Additional approved indications (beyond T2DM):
- Cardiovascular death reduction: Canagliflozin, Empagliflozin (in patients with T2DM + CVD)
- Heart failure (HFrEF): Dapagliflozin, Empagliflozin
- CKD progression: Canagliflozin, Dapagliflozin
Adverse effects:
- Genital mycotic infections (vulvovaginal candidiasis, balanitis) - most common
- Urinary tract infections, urinary frequency
- Hypotension (especially elderly, those on diuretics)
- DKA (including euglycemic DKA - even with near-normal glucose levels)
- Bone fractures (canagliflozin specifically)
- Fournier's gangrene (necrotizing fasciitis of perineum - rare but serious)
Limitation: Efficacy reduced when eGFR < 45 mL/min (needs filtration to work)
7. α-Glucosidase Inhibitors
Drugs: Acarbose, Miglitol
Mechanism:
- Reversibly inhibit α-glucosidase enzymes in the intestinal brush border
- These enzymes break down complex carbs into absorbable simple sugars
- Result: delayed carbohydrate digestion → blunted postprandial glucose rise
- No effect on fasting glucose
- No insulin secretion stimulation → no hypoglycemia as monotherapy
Important pearl: If hypoglycemia occurs (when combined with insulin/secretagogues), treat with pure glucose (NOT sucrose/table sugar - sucrase is also inhibited by these drugs)
Adverse effects:
- Flatulence, diarrhea, abdominal cramping (very common - limits clinical use)
- Avoided in IBD, colonic ulceration, intestinal obstruction
8. Other Oral Agents (Minor Use)
| Drug | Class | Mechanism | Note |
|---|---|---|---|
| Bromocriptine | Dopamine agonist | Unknown glucose-lowering mechanism | Modest HbA1c effect; limited use |
| Colesevelam | Bile acid sequestrant | Unknown glucose-lowering mechanism | Also lowers LDL; modest HbA1c effect |
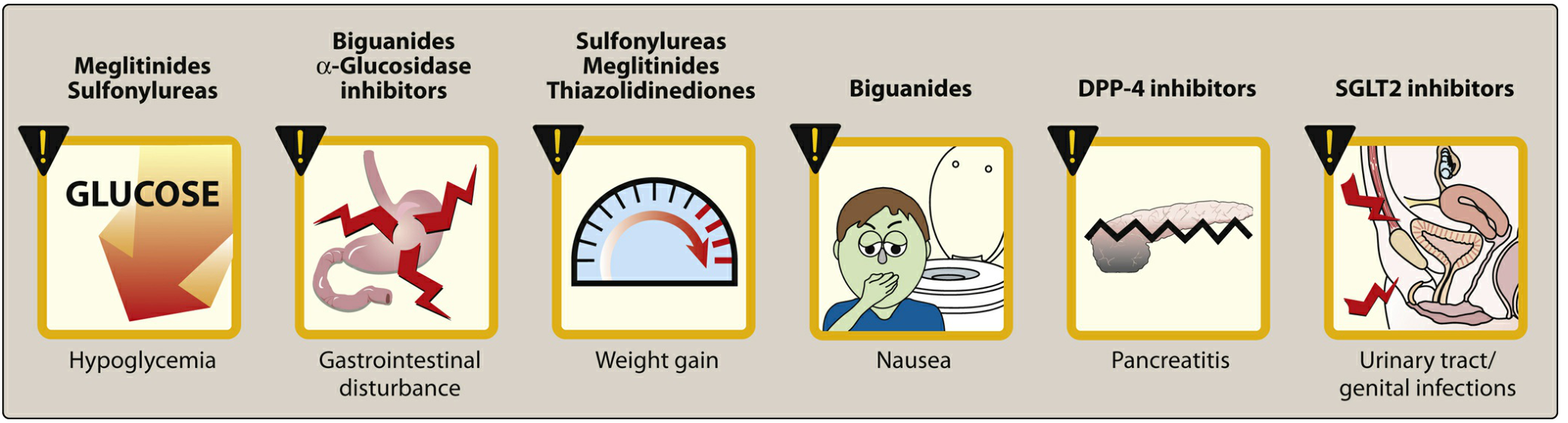
Adverse Effects at a Glance
Key Exam Points
- Hypoglycemia risk exists only with: Sulfonylureas, Meglitinides, and any drug combined with insulin/secretagogues
- No hypoglycemia as monotherapy: Metformin, TZDs, DPP-4i, SGLT2i, α-glucosidase inhibitors
- Weight gain drugs: Sulfonylureas, Meglitinides, TZDs
- Weight loss/neutral drugs: Metformin, SGLT2i (mild loss), DPP-4i (neutral)
- SGLT2i = cardio-renal protection - the modern "add-on" after metformin in patients with CVD, HF, or CKD
- Lactic acidosis - feared complication of metformin (rare); avoid in renal failure
- DKA - feared complication of SGLT2 inhibitors (can be euglycemic)
- Pancreatitis - associated with DPP-4 inhibitors and GLP-1 agonists
- Linagliptin - the only DPP-4 inhibitor NOT requiring renal dose adjustment (biliary excretion)
- Glyburide - safest to avoid in renal impairment among sulfonylureas
This is a shared conversation. Sign in to Orris to start your own chat.