Easily earn me chest x rays for respiratory disese in medicine ,examples with images,causes , differentiate points bw them
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
chest X-ray respiratory diseases patterns examples images differentiation medicine
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading Web Page
https://radiologyassistant.nl/chest/chest-x-ray/lung-disease
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the images and textbook content I need. Let me compose the comprehensive guide:
🫁 Chest X-Ray Patterns in Respiratory Disease - The Complete Guide
Sources: Murray & Nadel's Respiratory Medicine, Goldman-Cecil Medicine, Harrison's Principles (22nd Ed.), Rosen's Emergency Medicine, Grainger & Allison's Diagnostic Radiology
Quick Memory Framework: The 5 Core CXR Patterns
| Pattern | Appearance | Think of |
|---|---|---|
| Consolidation | White/opaque area - airspace filled | Pneumonia, pulmonary oedema |
| Hyperinflation | Black/over-dark lungs, flat diaphragm | COPD/Emphysema |
| Pleural effusion | White lower zone, blunted angle | Heart failure, infection, cancer |
| Pneumothorax | Black rim + no lung markings | Trauma, spontaneous |
| Reticulation/Nodules | Fine mesh/lace or dots | TB, ILD, sarcoidosis |
1. LOBAR PNEUMONIA (Consolidation)
CXR Appearance:
- Homogeneous white opacity conforming to a lobe
- Air bronchograms (dark branching airways inside the white area - pathognomonic of airspace filling)
- Lobar or segmental distribution
- No volume loss (the lobe is FULL, not collapsed)
Causes:
- Streptococcus pneumoniae (most common, right upper lobe classic)
- Klebsiella pneumoniae (right upper lobe, "bulging fissure" sign)
- Community-acquired pneumonia (CAP)
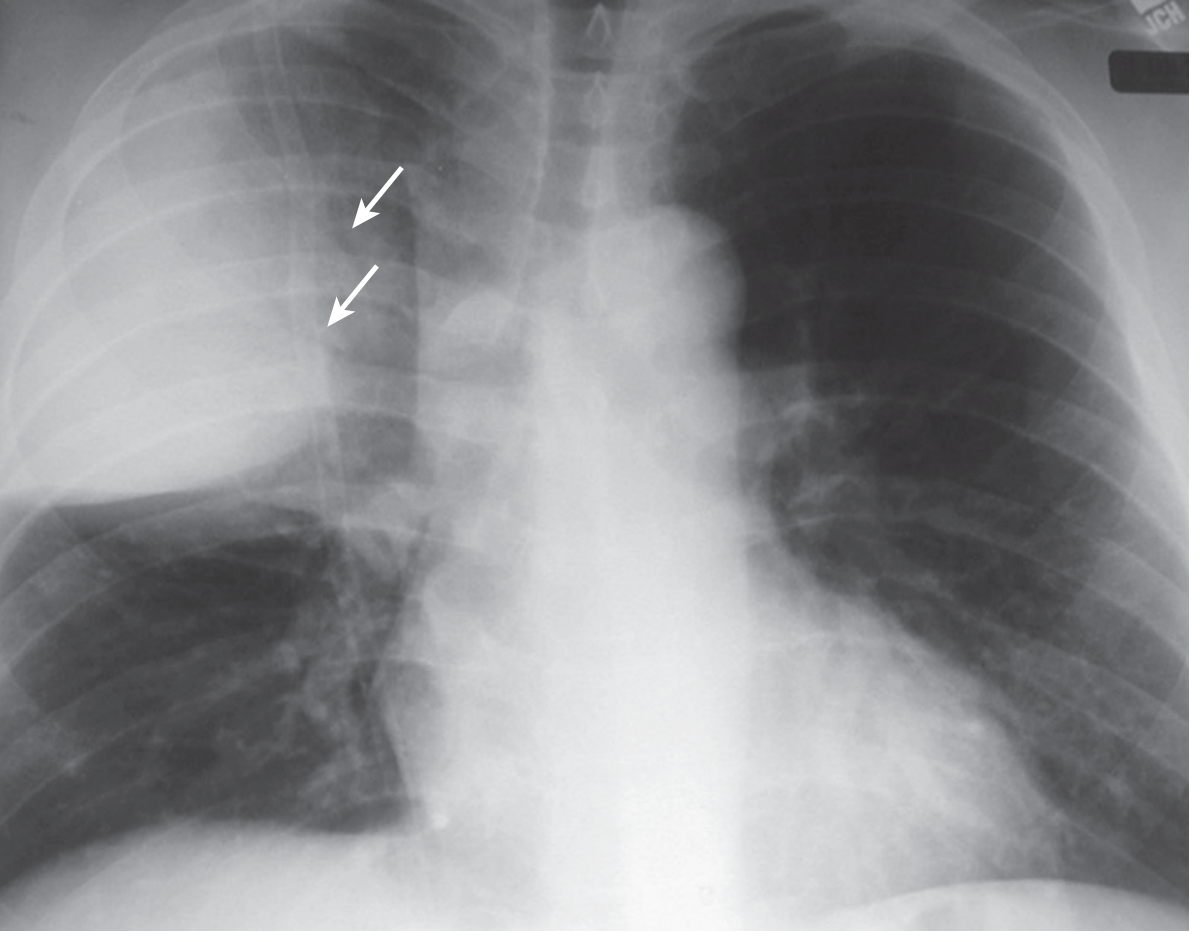
Key points: The arrow shows air bronchograms - dark air-filled airways visible through the white consolidated lobe. No volume loss = consolidation (not collapse).
2. BRONCHOPNEUMONIA (Patchy Consolidation)
CXR Appearance:
- Patchy, multifocal, ill-defined opacities - scattered like "cotton balls"
- Bilateral or unilateral
- No single lobe boundary
- May have small centrilobular nodules
Causes:
- Staphylococcus aureus (MRSA - can cavitate)
- Mycoplasma pneumoniae (bilateral, basal)
- Haemophilus influenzae
- Aspiration pneumonia (RLL predominant, dependent regions)
- Measles, adenovirus (viral - peribronchial pattern)
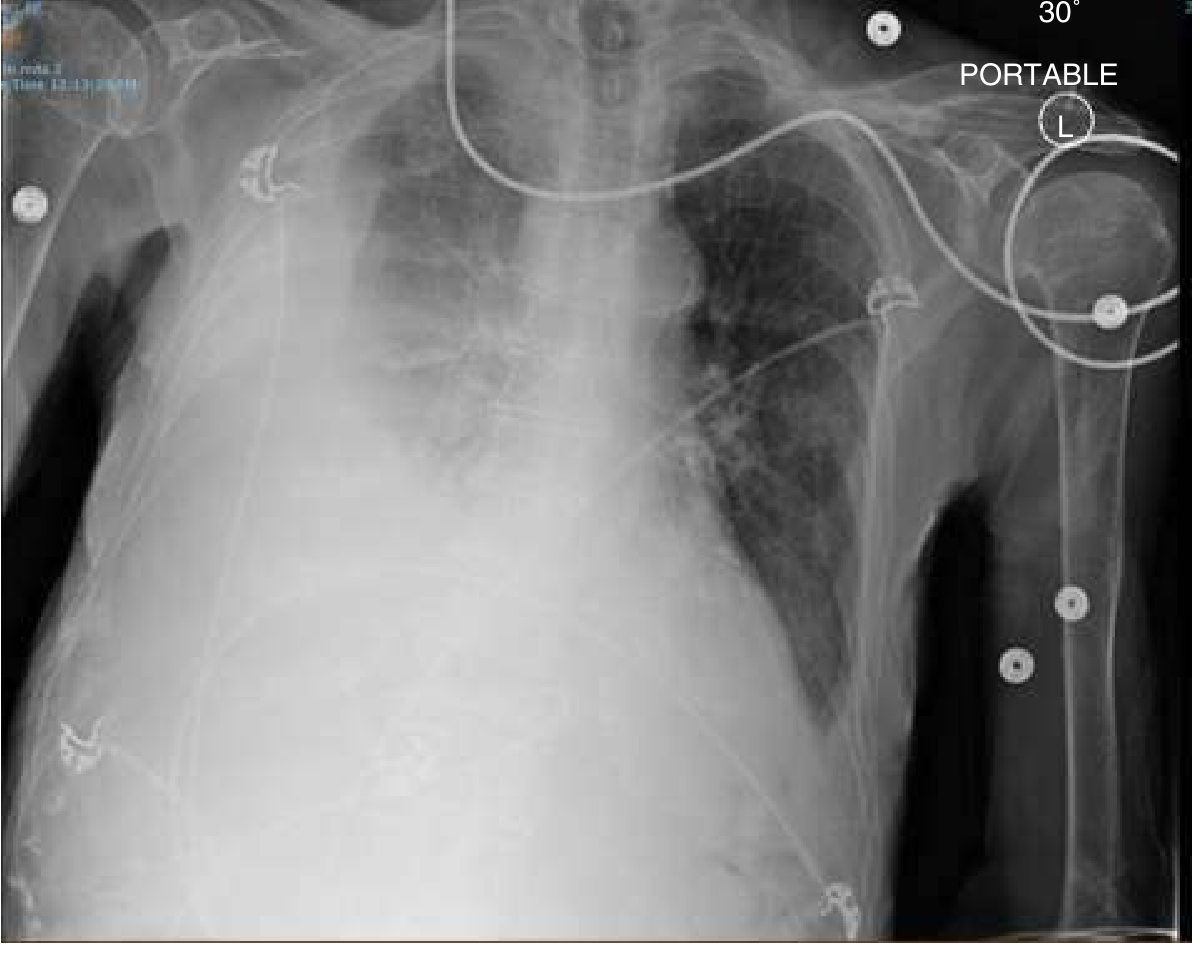
3. PULMONARY OEDEMA (Perihilar Bat-Wing / Alveolar Flooding)
CXR Appearance:
- Bilateral perihilar ("bat-wing") infiltrates
- Kerley B lines - 1-2 cm horizontal lines at lateral lung bases (dilated lymphatics/fluid in interlobular septa)
- Upper lobe vascular diversion (cephalization of flow)
- Cardiomegaly (heart > 50% of thoracic diameter)
- Blunted costophrenic angles (effusions)
- Hazy/ground-glass shadowing bilateral, perihilar > peripheral
Causes:
- Left ventricular failure / heart failure (cardiogenic)
- ARDS / sepsis (non-cardiogenic - no cardiomegaly, no effusions)
- Renal failure, volume overload
- Mitral stenosis

4. PLEURAL EFFUSION
CXR Appearance:
- Blunting of the costophrenic angle (>200 mL visible on PA)
- Homogeneous basal opacity with a concave upper margin (meniscus sign)
- Fluid layers laterally higher than medially
- Massive effusion: complete opacification of a hemithorax
- On supine films: diffuse haziness of the hemithorax
Causes:
- Transudate: Heart failure (bilateral, R > L), hypoalbuminaemia, renal failure
- Exudate: Pneumonia (parapneumonic), TB, malignancy, pulmonary embolism
How to spot: Start at the costophrenic angles - they should be sharp and acute. Any blunting = suspect effusion.
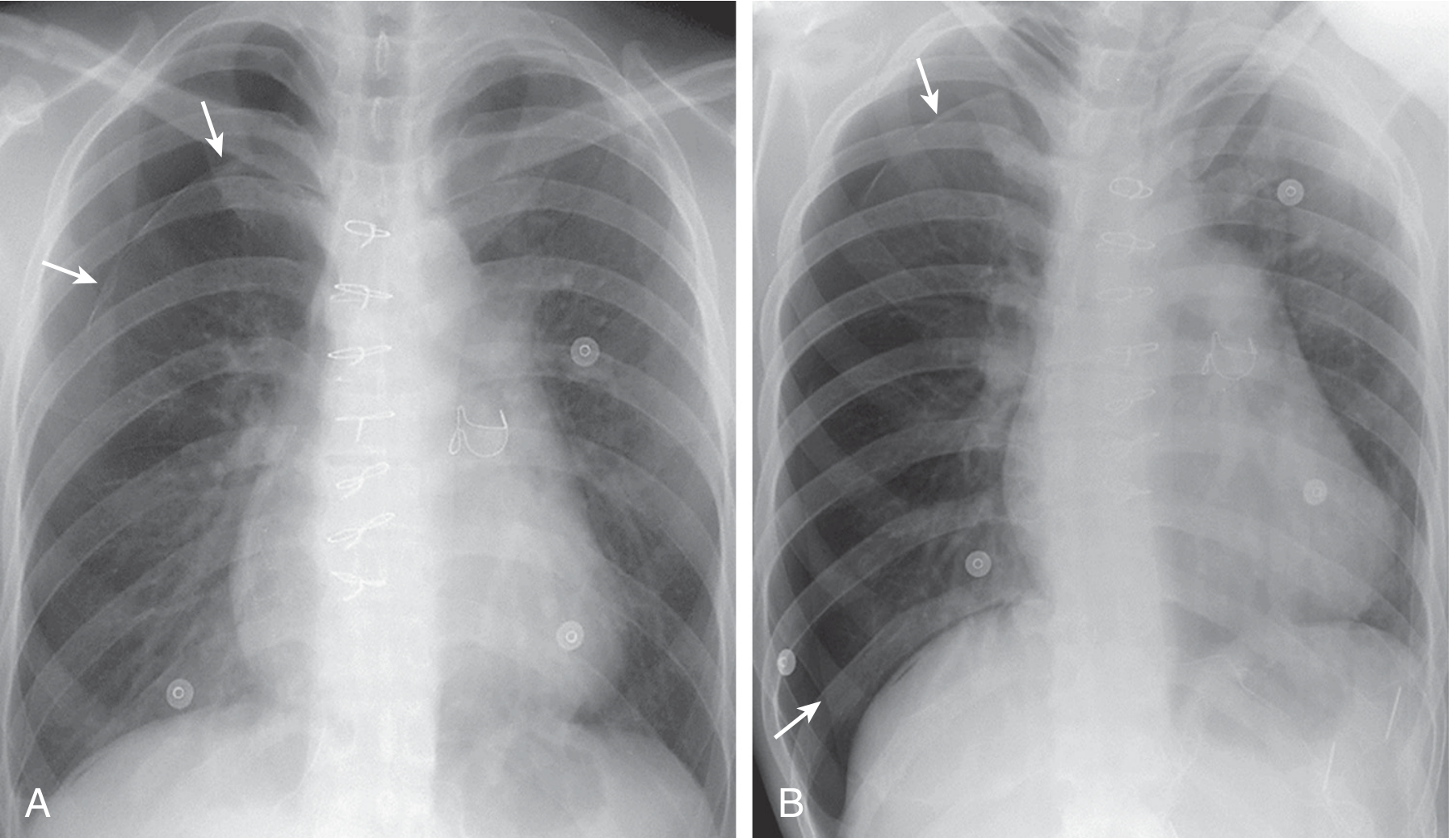
5. PNEUMOTHORAX
CXR Appearance:
- Visible pleural line - a thin white line parallel to the chest wall
- Complete absence of lung markings peripheral to that line (black space)
- Lung "falls away" from the chest wall
- Tension PTX: mediastinal shift AWAY from affected side + depressed hemidiaphragm - medical emergency!
Causes:
- Primary spontaneous: Tall, thin young males (ruptured apical bleb)
- Secondary spontaneous: COPD (emphysematous bullae), asthma, TB, cystic fibrosis
- Traumatic: Rib fractures, iatrogenic (central line, thoracentesis)
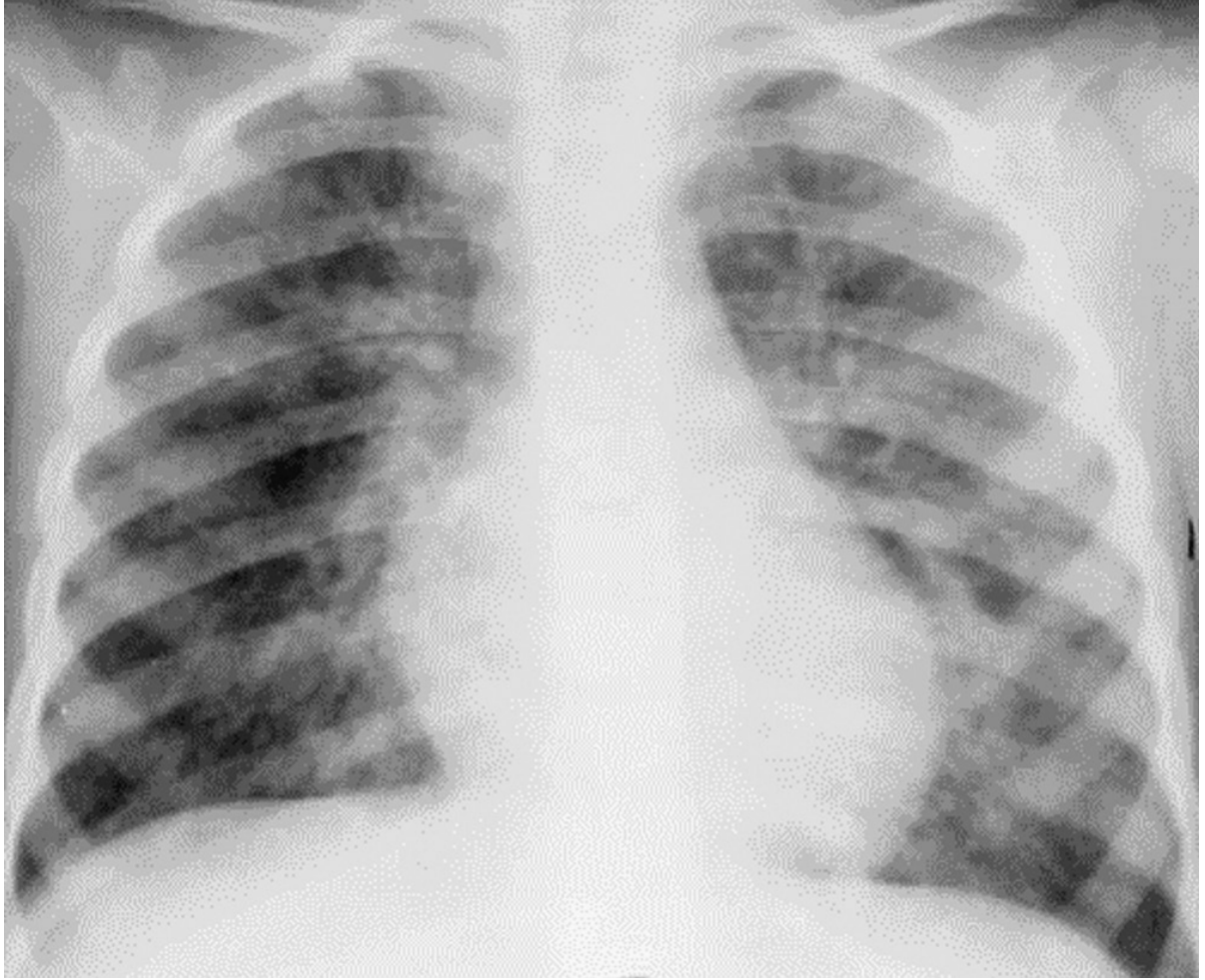
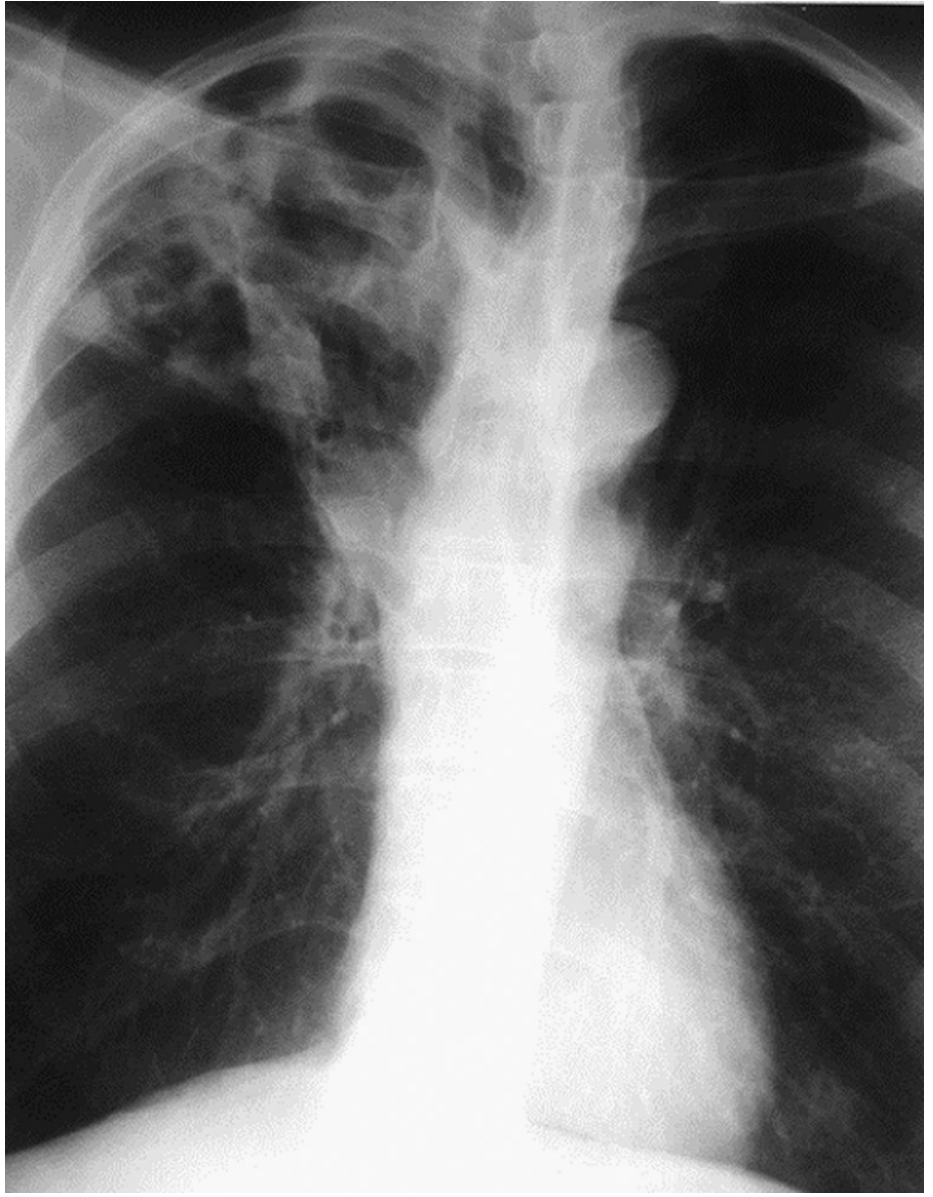
6. TUBERCULOSIS (TB)
CXR Appearance:
| Type | Location | Pattern |
|---|---|---|
| Primary TB | Middle/lower zone + ipsilateral hilar adenopathy | Consolidation + enlarged hilum |
| Reactivation TB | Apical/posterior segment upper lobes (R > L) | Cavitation, fibrosis, calcification |
| Miliary TB | Diffuse both lungs | 1-3mm nodules "millet seeds" throughout |
| HIV-associated TB | Lower zones, diffuse | Atypical - no cavity, adenopathy |
Causes: Mycobacterium tuberculosis - reactivation of latent infection
7. COPD / EMPHYSEMA
CXR Appearance:
- Hyperinflation - lungs look too dark, >6 anterior ribs visible above diaphragm on PA
- Flattened hemidiaphragms (most reliable sign)
- Increased AP diameter ("barrel chest")
- Increased retrosternal airspace on lateral view
- Prominent pulmonary arteries (cor pulmonale if right heart fails)
- Bullae (black avascular areas with thin walls) in emphysema
Causes: Smoking (>90%), alpha-1 antitrypsin deficiency, occupational dust
Memory trick: Flattened diaphragm + dark lungs + SMALL heart = COPD
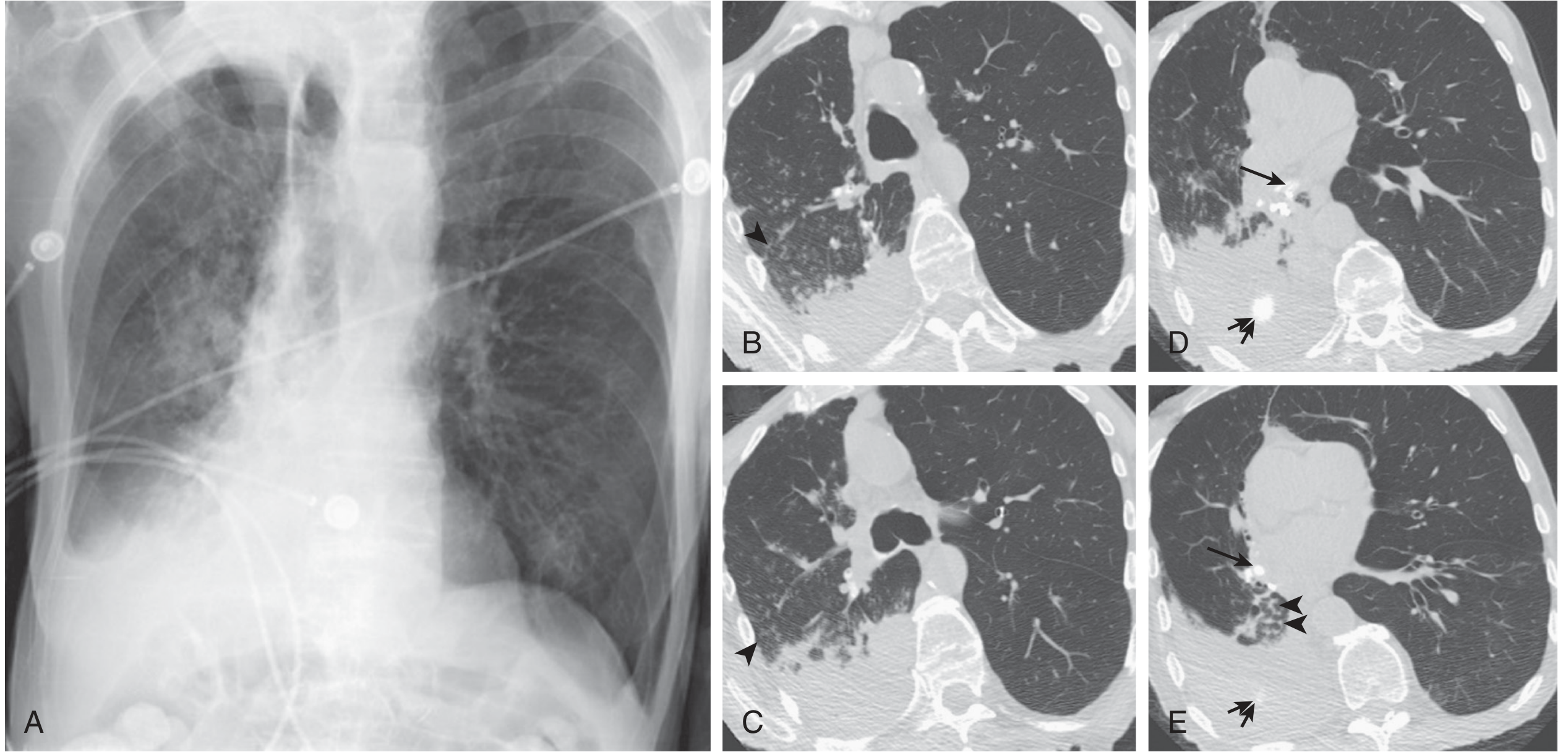
8. COVID-19 PNEUMONIA (Organizing Pneumonia Pattern)
CXR Appearance:
- Bilateral, peripheral, lower-zone predominant consolidation
- "Ground glass" opacities
- Rounded/confluent consolidations
- Spares central/perihilar regions (unlike pulmonary oedema)
- Often accompanied by small pleural effusions
MASTER DIFFERENTIATION TABLE
| Feature | Pneumonia (Lobar) | Pulm. Oedema | Pleural Effusion | Pneumothorax | TB (Reactivation) | COPD |
|---|---|---|---|---|---|---|
| Location | Lobar/segmental | Bilateral perihilar | Basal | Apex (rim) | Upper lobe | Diffuse |
| Opacity | Dense white, lobar | Perihilar haze | Lower zone white | Black (avascular) | Patchy + cavities | Hyper-dark |
| Air bronchograms | YES (hallmark) | May be present | No | No | Variable | No |
| Meniscus sign | No | No | YES | No | No | No |
| Kerley B lines | No | YES | Sometimes | No | No | No |
| Cardiomegaly | No | YES (cardiac cause) | No | No | No | Late (cor pulm) |
| Cavitation | Possible (MRSA) | No | No | No | YES (classic) | Bullae |
| Trachea/mediastinum | Midline | Midline | Shifted AWAY | Shifted AWAY (tension) | Shifted TOWARD (fibrosis) | Midline |
| Diaphragm | Normal | Normal-elevated | Obscured | Depressed (tension) | Elevated (fibrosis) | Flat |
| Volume | Preserved | Increased | Decreased (compressed) | Increased | Decreased | Increased |
| Key memory hook | Air bronchograms | Bat wings + Kerley B | Costophrenic blunting | Pleural line + black | Upper lobe cavity | Flat diaphragm |
QUICK MNEMONICS
For PLEURAL EFFUSION vs CONSOLIDATION:
- Effusion: Concave upper border (meniscus), no air bronchograms, shift AWAY
- Consolidation: Air bronchograms, no shift (unless collapse), lobar shape
For PULMONARY OEDEMA (ABCDE):
Alveolar oedema (bat-wing), B-lines (Kerley), Cardiomegaly, Diversion of vessels (upper lobe), Effusions (bilateral)
For TB upper zone lesions:
"FACTS" = Fibrocavitary, Apical, Calcification, Top (upper) lobe, Scarring
Pneumothorax vs Bullae:
- Pneumothorax: rim of air wraps the ENTIRE edge of lung
- Bullae: confined, localized, thin-walled bubble, lung markings present beyond it
CXR INTERPRETATION APPROACH (ABCDE System)
- A - Airways: trachea midline? carina angle (<70°)?
- B - Bones/soft tissue: rib fractures, mastectomy?
- C - Cardiac: size, shape (>50% of thorax = cardiomegaly)
- D - Diaphragm: flat (COPD), high (effusion, phrenic paralysis), costophrenic angles sharp?
- E - Everything else: lung fields zone by zone, hilum, mediastinum
Sources: Murray & Nadel's Respiratory Medicine | Goldman-Cecil Medicine | Harrison's Principles of Internal Medicine 22nd Ed. | Rosen's Emergency Medicine | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.