What is cause pof hypotension
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of the causes of hypotension, organized by the four classical categories used in clinical medicine:
Causes of Hypotension
Hypotension is low blood pressure, typically defined as systolic BP < 90 mmHg. In patients with shock, distributive causes account for ~65% of cases, hypovolemic and cardiogenic each about 15%, and obstructive < 5%.
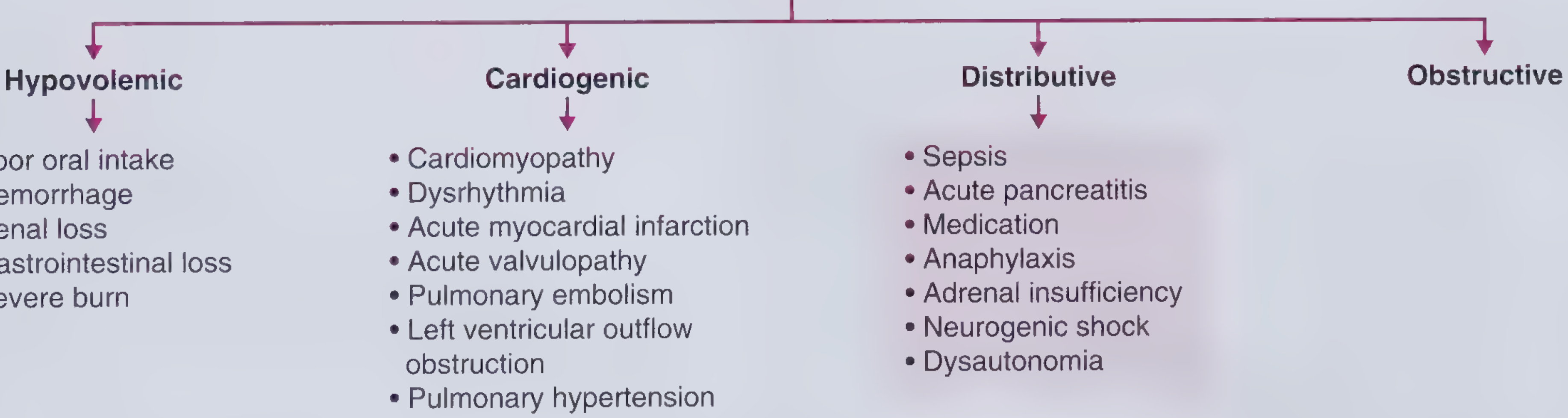
1. Hypovolemic Hypotension
Mechanism: Decreased intravascular volume → reduced preload → decreased cardiac output.
Hemodynamics: Low JVP, Low CO, High SVR (cool extremities)
| Cause | Example |
|---|---|
| Poor oral intake | Elderly, anorexia, delirium, intestinal obstruction |
| Hemorrhage | Trauma (retroperitoneal, pelvic, thigh bleeds are occult) |
| Renal losses | Diuretics, primary adrenal insufficiency (renal salt wasting) |
| GI losses | Diarrhea, vomiting |
| Severe burns | Massive transcutaneous fluid loss |
2. Cardiogenic Hypotension
Mechanism: Heart fails to pump adequately → reduced cardiac output.
Hemodynamics: High JVP, Low CO, High SVR
- Cardiomyopathy (dilated, hypertrophic, restrictive)
- Dysrhythmias (atrial fibrillation with rapid rate, heart block)
- Acute myocardial infarction (especially inferior MI causing right heart failure)
- Acute valvulopathy (acute aortic regurgitation, mitral regurgitation)
- Pulmonary embolism (massive PE with acute right heart strain)
- Left ventricular outflow tract obstruction (aortic stenosis, hypertrophic cardiomyopathy)
- Pulmonary hypertension (right heart failure)
3. Distributive Hypotension
Mechanism: Pathological systemic vasodilation → decreased SVR despite normal or high CO.
Hemodynamics: Normal/Low JVP, High CO, Low SVR (warm extremities)
- Sepsis - the most common cause (~65% of all shock cases)
- Anaphylaxis - accompanied by bronchospasm and urticaria
- Acute pancreatitis - massive inflammatory vasodilation
- Medications - antihypertensives, nitrates, opioids, anesthetics, antidepressants (TCAs)
- Adrenal insufficiency (Addison's disease) - hyperpigmentation + hyponatremia + hyperkalemia
- Neurogenic shock - spinal cord injury with sudden loss of sympathetic tone
- Dysautonomia - e.g., Parkinson's disease causing orthostatic hypotension
4. Obstructive Hypotension
Mechanism: Physical obstruction to cardiac filling or output.
Hemodynamics: High JVP, Low CO, High SVR
- Cardiac tamponade - enlarged cardiac silhouette, muffled heart sounds, pulsus paradoxus > 10 mmHg
- Tension pneumothorax - tracheal deviation, absent breath sounds, requires emergency needle decompression
- Constrictive pericarditis - Kussmaul's sign + pericardial knock
Additional Specific Causes to Know
| Category | Examples |
|---|---|
| Orthostatic hypotension | Dehydration, prolonged bed rest, autonomic neuropathy (diabetes, Parkinson's) |
| Medication-induced | Beta-blockers, calcium channel blockers, ACE inhibitors, alpha-blockers, diuretics |
| Endocrine | Hypothyroidism, adrenal crisis, pheochromocytoma crisis |
| Toxicological | Overdose with antihypertensives, opioids, barbiturates, tricyclics |
| Pregnancy-related | Aortocaval compression (supine hypotension syndrome), hemorrhage |
Key clinical tip: Always approach hypotension by quickly identifying the mechanism - the treatment differs completely: fluids for hypovolemic, inotropes/vasopressors for cardiogenic, vasopressors + antibiotics for sepsis, and emergency decompression for obstructive causes.
- Frameworks for Internal Medicine, pp. 295-301
- Miller's Anesthesia, 10e (Other Causes of Hypotension section)
This is a shared conversation. Sign in to Orris to start your own chat.