Make detailed write up on normal physiological changes in menstrual cycle
Reading File
Finding Sources
Finding Sources
Searching PubMed
"menstrual cycle" AND "physiology" AND "hormonal changes"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the data needed for a comprehensive, authoritative write-up. Let me compose the full detailed document.
Normal Physiological Changes in the Menstrual Cycle
Overview
The menstrual cycle is a recurring series of physiological events in women of reproductive age, designed to prepare the body for potential pregnancy and, if fertilization does not occur, to reset the system for the next cycle. A "typical" cycle spans 28 days (though 21-35 days is normal), measured from the first day of menstrual bleeding to the first day of the next bleed. The cycle involves precise, interdependent coordination among four anatomical components: the hypothalamus, the anterior pituitary, the ovaries, and the uterus (endometrium).
The cycle is divided into two major parallel tracks:
| Track | Phase 1 | Phase 2 |
|---|---|---|
| Ovarian cycle | Follicular phase (days 1-14) | Luteal phase (days 15-28) |
| Uterine cycle | Proliferative phase (days 1-14) | Secretory phase (days 15-28) |
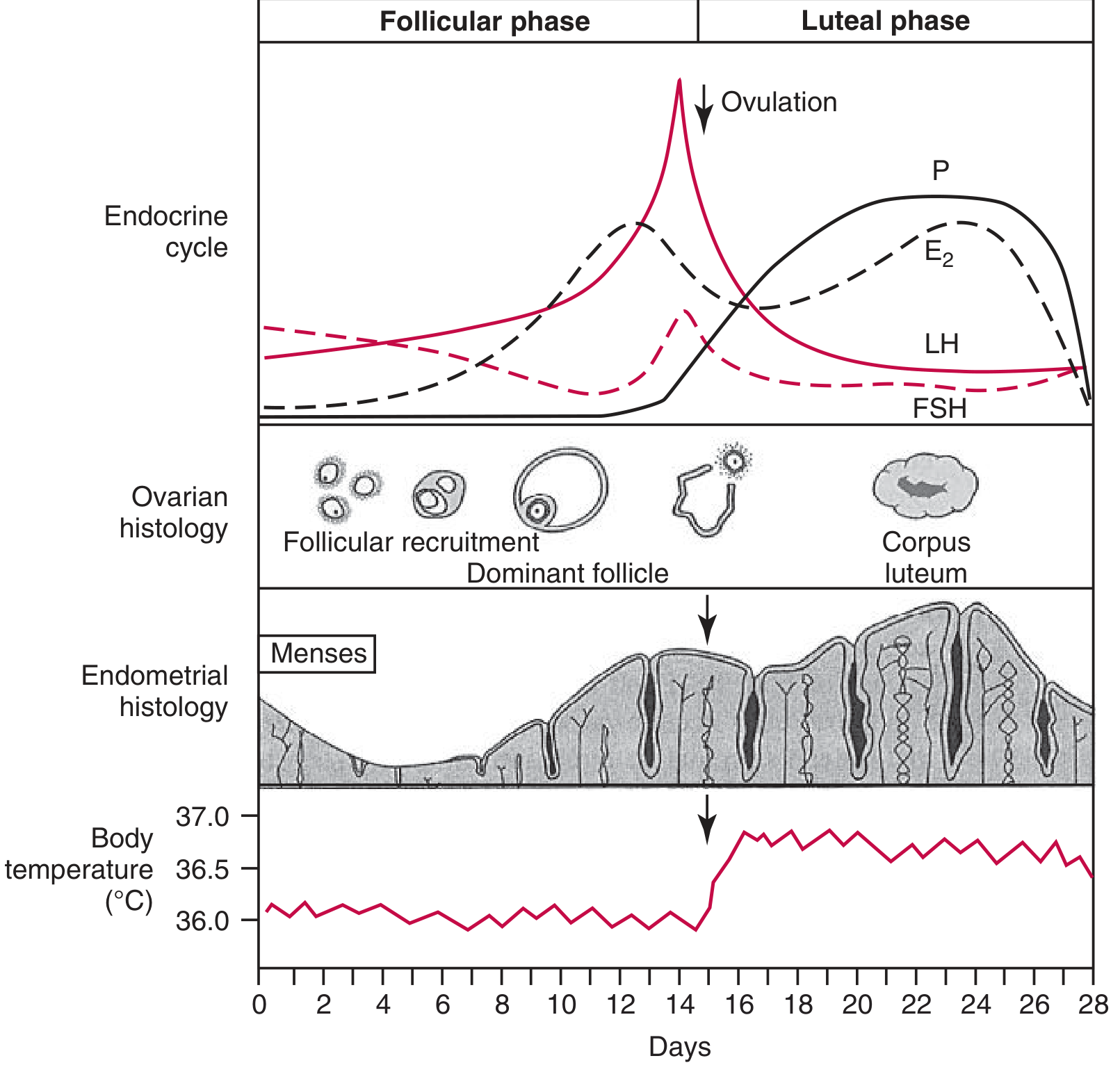
Figure: Hormonal, ovarian, endometrial, and basal body temperature changes throughout the normal menstrual cycle. (Tietz Textbook of Laboratory Medicine, 7th Edition)
1. Neuroendocrine Control: The Hypothalamic-Pituitary-Ovarian Axis
Hypothalamus and GnRH
The hypothalamus is the master regulator of the menstrual cycle. Located at the base of the brain above the optic chiasm, it contains specialized neurons (primarily in the arcuate nucleus) that synthesize and release gonadotropin-releasing hormone (GnRH) - a decapeptide - in pulsatile fashion into the hypothalamo-hypophyseal portal circulation.
The pulsatility of GnRH is critical: the frequency and amplitude of pulses determine the relative amounts of FSH and LH secreted by the pituitary:
- Slower, lower-amplitude pulses favor FSH secretion
- Faster, higher-amplitude pulses favor LH secretion
- Continuous, non-pulsatile GnRH actually suppresses gonadotropin release (the basis for GnRH agonist therapy)
The hypothalamus operates within three feedback loop levels:
- Long loop: circulating ovarian steroids (estrogen, progesterone) feed back on hypothalamic and pituitary receptors
- Short loop: pituitary gonadotropins feed back to hypothalamus
- Ultrashort loop: GnRH itself feeds back locally on GnRH neurons
Anterior Pituitary
The anterior pituitary responds to GnRH pulses by releasing two gonadotropins:
- Follicle-stimulating hormone (FSH): a glycoprotein that drives follicular recruitment, granulosa cell proliferation, and estrogen synthesis
- Luteinizing hormone (LH): essential for androgen production in theca cells, triggering ovulation, and supporting corpus luteum function
2. The Follicular Phase (Days 1-14)
Early Follicular Phase (Days 1-5): Follicle Recruitment
At the beginning of each cycle, estrogen and progesterone levels are at their lowest (following corpus luteum demise from the previous cycle). This fall in steroid levels releases the pituitary from negative feedback, allowing FSH to rise.
Rising FSH recruits a cohort of primordial follicles from the ovarian reserve. At birth, the ovaries contain approximately 2 million primordial follicles; by puberty this falls to under 300,000, and only approximately 500 follicles will ever reach maturity over a woman's reproductive life - the rest undergo atresia by apoptosis.
The recruited follicles are initially primordial follicles (one oocyte surrounded by a single layer of granulosa cells). Under FSH stimulation they progress to:
- Primary follicles - granulosa cells become cuboidal and proliferate
- Secondary (preantral) follicles - theca cells differentiate; estrogen synthesis begins
- Tertiary (antral) follicles - a fluid-filled antrum forms; the follicle grows substantially
The Two-Cell, Two-Gonadotropin Model
Estrogen biosynthesis in the follicle requires both cell types working in concert:
- Theca interna cells (LH-stimulated) produce androgens (androstenedione, testosterone) from cholesterol
- These androgens diffuse into granulosa cells, where FSH-stimulated aromatase converts them to estradiol (E2)
This is the "two-cell, two-gonadotropin" model of ovarian steroidogenesis.
Dominant Follicle Selection (Around Day 6-7)
By approximately day 6, one follicle in one ovary becomes the dominant follicle, while the others undergo atresia. The mechanism of selection is not fully understood but appears to relate to the dominant follicle's superior ability to produce intrafollicular estrogen, which amplifies its own FSH-receptor expression and creates a microenvironment increasingly supportive of further growth.
As the dominant follicle grows, it secretes increasing amounts of estradiol and inhibin B:
- Inhibin B acts on the pituitary to suppress FSH (selectively reducing FSH support from subordinate follicles, causing their atresia)
- Rising estradiol initially exerts negative feedback on both FSH and LH
Late Follicular Phase (Days 10-13): Pre-Ovulatory Rise
In the late follicular phase, the dominant (graafian) follicle reaches 18-25 mm in diameter. Estradiol peaks at 250-500 pg/mL (917-1835 pmol/L). At this critical threshold, estradiol switches its action from negative to positive feedback on the hypothalamic-pituitary axis - a phenomenon unique to this phase and dependent on:
- Sustained exposure to high estradiol for at least 36-48 hours
- A threshold concentration being maintained
This positive feedback triggers the LH surge - a sharp, massive release of LH from the anterior pituitary.
Additionally, FSH-induced LH receptors appear on granulosa cells during the late follicular phase, and progesterone secretion begins. This early progesterone is responsible for the FSH midcycle surge that occurs alongside the LH surge.
3. Ovulation (Around Day 14)
The LH surge is the proximate trigger for ovulation, occurring 24-36 hours after the surge onset. For 90% of women, the onset of the LH surge occurs 16-58 hours before ovulation, and the LH peak occurs 3-36 hours before ovulation.
The LH surge induces:
- Resumption of meiosis in the oocyte - the primary oocyte (arrested in prophase I since fetal development) completes the first meiotic division, extruding the first polar body to form the secondary oocyte, which immediately begins meiosis II (arrests at metaphase II; completed only if fertilization occurs)
- Follicular wall rupture - via prostaglandin synthesis, collagenase activation, and smooth muscle contraction in the follicular wall
- Oocyte extrusion into the peritoneal cavity, where it is captured by the fimbriated end of the fallopian tube
Minor bleeding from the ruptured follicle into the peritoneal cavity may cause mittelschmerz (fleeting mid-cycle lower abdominal pain). The empty follicle rapidly fills with blood, forming the corpus hemorrhagicum.
4. The Luteal Phase (Days 15-28)
Corpus Luteum Formation and Function
After ovulation, the granulosa and theca cells of the ruptured follicle rapidly undergo luteinization - a process driven by LH. The clotted blood in the corpus hemorrhagicum is replaced by yellowish, lipid-rich luteal cells, forming the corpus luteum. Vascular ingrowth (critically dependent on VEGF - vascular endothelial growth factor) supports the corpus luteum's metabolic needs.
The corpus luteum secretes two key hormones:
- Progesterone: the dominant hormone of the luteal phase, peaking around 8 days post-ovulation (days 21-22 of a 28-day cycle). Serum levels rise 10- to 20-fold from baseline. A midluteal progesterone >3 ng/mL is presumptive evidence of ovulation
- Estradiol: a secondary peak (~125 pg/mL) occurs in the midluteal phase from corpus luteum secretion
- Inhibin A: also secreted by the corpus luteum; suppresses FSH
Together, progesterone, estradiol, and inhibin A exert negative feedback on the hypothalamic-pituitary axis, suppressing LH and FSH and preventing new follicular development during this phase.
Corpus Luteum Demise (Days 24-28)
In the absence of pregnancy (and therefore no hCG from trophoblast to maintain it), the corpus luteum begins to degenerate around day 24 of the cycle. The mechanism of luteolysis is not entirely clear in humans but involves withdrawal of LH support and local prostaglandins.
As the corpus luteum fails:
- Progesterone, estradiol, and inhibin A all fall
- The negative feedback on the pituitary is removed
- FSH begins to rise in the late luteal phase, recruiting the next cohort of follicles
- The endometrium loses hormonal support, leading to menstruation
- The corpus luteum is eventually replaced by an avascular scar, the corpus albicans
If pregnancy occurs, the embryo's trophoblast secretes hCG (human chorionic gonadotropin) from implantation (around day 21-23), which has high structural homology to LH and binds LH receptors on the corpus luteum, "rescuing" it and maintaining progesterone production until the placenta takes over at approximately 8-10 weeks.
5. The Uterine (Endometrial) Cycle
The endometrium undergoes parallel histological changes driven by ovarian hormones. The superficial two-thirds of the endometrium (the stratum functionalis) proliferates and is shed each cycle; the deep layer (the stratum basalis) persists and is the source of regeneration.
Menstruation (Days 1-4)
When the corpus luteum degenerates and estrogen/progesterone fall:
- The stroma becomes edematous, then undergoes necrosis
- Spiral arteries (which supply the stratum functionalis) undergo vasospasm, likely mediated by prostaglandins (particularly PGF2α), causing ischemic necrosis
- The superficial endometrium (stratum compactum and stratum spongiosum) is shed along with blood
- Normal menstrual flow: 2-6 days, average blood loss 20-60 mL (up to 80 mL is normal)
- Prostaglandin-mediated uterine contractions produce menstrual cramps (dysmenorrhea); this is why prostaglandin synthetase inhibitors (NSAIDs) relieve cramping
Proliferative Phase (Days 5-14)
Under the influence of rising estradiol from the developing follicle, the endometrium regenerates and thickens from approximately 1-2 mm to up to 10 mm. Key histological changes:
- Glands: straight, narrow, and lined by columnar epithelium with increasing mitotic activity; glands elongate as the endometrium thickens
- Stroma: dense and cellular; mitotic figures visible
- Spiral arteries: grow and elongate parallel to the gland growth
- Surface epithelium: columnar cells reform the uterine cavity lining
By convention, this phase corresponds exactly to the follicular (ovarian) phase.
Secretory Phase (Days 15-28)
After ovulation, progesterone from the corpus luteum transforms the proliferative endometrium into a secretory endometrium ideally suited for embryo implantation:
- Glands: become coiled and tortuous; columnar cells develop subnuclear glycogen vacuoles (earliest histological sign, day 16-17) that then move to supranuclear position and discharge secretions into the gland lumen
- Stroma: becomes edematous; predecidual reaction begins around spiral arteries late in the luteal phase (days 23-24)
- Spiral arteries: elongate markedly and become tightly coiled
- Pinopodes: surface epithelial projections appear around days 20-22, coinciding with the "implantation window"
If implantation occurs, the stroma transforms fully into decidua (decidualization). If no pregnancy occurs, the endometrium involutes with the corpus luteum, setting the stage for the next menstruation.
The classic histological dating of the endometrium (Noyes, Hertig, and Rook, 1950) correlates endometrial morphology precisely with cycle day and progesterone exposure.
6. Cervical Changes
The cervix also undergoes cyclic changes that facilitate or impede sperm transport:
Follicular phase (estrogen dominant):
- Cervical vascularity, congestion, and edema increase
- Cervical mucus quantity increases 10- to 30-fold (from ~20-60 mg/day to 600+ mg/day near ovulation)
- Mucus becomes copious, watery, and elastic (spinnbarkeit - can be drawn into threads >6 cm)
- When spread on a glass slide, it produces a "ferning" (arborization) pattern - crystallization of sodium chloride creates a palm-leaf pattern. This corresponds to the fertile window, forming channels through which sperm can be propelled
Luteal phase (progesterone dominant):
- Mucus volume decreases dramatically
- Mucus becomes thick, viscous, and non-elastic - a "hostile" mucus that impedes sperm penetration
- The ferning pattern disappears (no crystallization)
- This change is physiologically appropriate: post-ovulation, the window for fertilization has closed
7. Vaginal Changes
The vaginal epithelium is exquisitely sensitive to estrogen and provides a clinical indicator of hormonal status:
- Low estrogen (early follicular, menstruation): thin, pale epithelium with predominantly parabasal cells; low maturation index
- Rising estrogen: progressive cornification of the superficial epithelial layer; increased percentage of cornified (superficial) cells; vaginal pH decreases (more acidic)
- Progesterone (luteal phase): decreases the percentage of cornified cells; increases precornified intermediate cells with increased cellular debris and clumping of desquamated cells
Vaginal cytology (maturation index) can be used as a bioassay for estrogen status.
8. Basal Body Temperature (BBT)
Progesterone has a mild thermogenic effect mediated via the hypothalamic thermoregulatory center:
- During the follicular phase, resting BBT is approximately 36.0-36.5°C
- After ovulation, progesterone from the corpus luteum causes a rise of approximately 0.2-0.5°C
- BBT remains elevated throughout the luteal phase (~36.5-37.0°C) and falls at the onset of menstruation
This biphasic pattern (seen in the diagram above) forms the basis of the basal body temperature method of cycle tracking. Since the rise occurs after ovulation, it confirms ovulation retrospectively rather than predicting it prospectively.
9. Androgen Changes
Androgen production also fluctuates across the cycle. A midcycle peak in androgens (androstenedione and testosterone) occurs around ovulation, arising from the theca cells of the dominant follicle under LH stimulation. Some women notice a slight increase in libido at this time, which has evolutionary relevance. Estrone, primarily from peripheral aromatization of androstenedione, is also increased throughout the cycle.
10. Inhibins and Other Regulatory Peptides
Two isoforms of inhibin play distinct roles:
- Inhibin B: secreted by granulosa cells of small antral follicles in the early-to-mid follicular phase; selectively suppresses FSH from the pituitary, contributing to dominant follicle selection
- Inhibin A: secreted by the dominant follicle pre-ovulation and by the corpus luteum in the luteal phase; contributes to suppression of FSH during the luteal phase
Activin (a related TGF-β family peptide) has the opposite effect - it stimulates FSH secretion and amplifies FSH action within follicles. The ratio of inhibin to activin modulates the fine-tuning of gonadotropin output.
Follistatin is an activin-binding protein that dampens activin signaling, adding another layer of regulation.
11. Hormone Reference Ranges Across the Cycle
| Hormone | Follicular phase | LH surge / Ovulation | Luteal phase |
|---|---|---|---|
| FSH | 3-10 IU/L (rises early, then falls) | Midcycle peak: 7-20 IU/L | 2-8 IU/L |
| LH | 2-15 IU/L | Surge peak: 25-100+ IU/L | 2-15 IU/L |
| Estradiol (E2) | 20-350 pg/mL (rising) | 250-500 pg/mL peak | ~125 pg/mL (second rise) |
| Progesterone | <1 ng/mL | <2 ng/mL | 5-20 ng/mL (peak ~day 21) |
12. Summary: The Integrated Cycle
The diagram below shows the integrated pituitary, ovarian, and endometrial cycles:
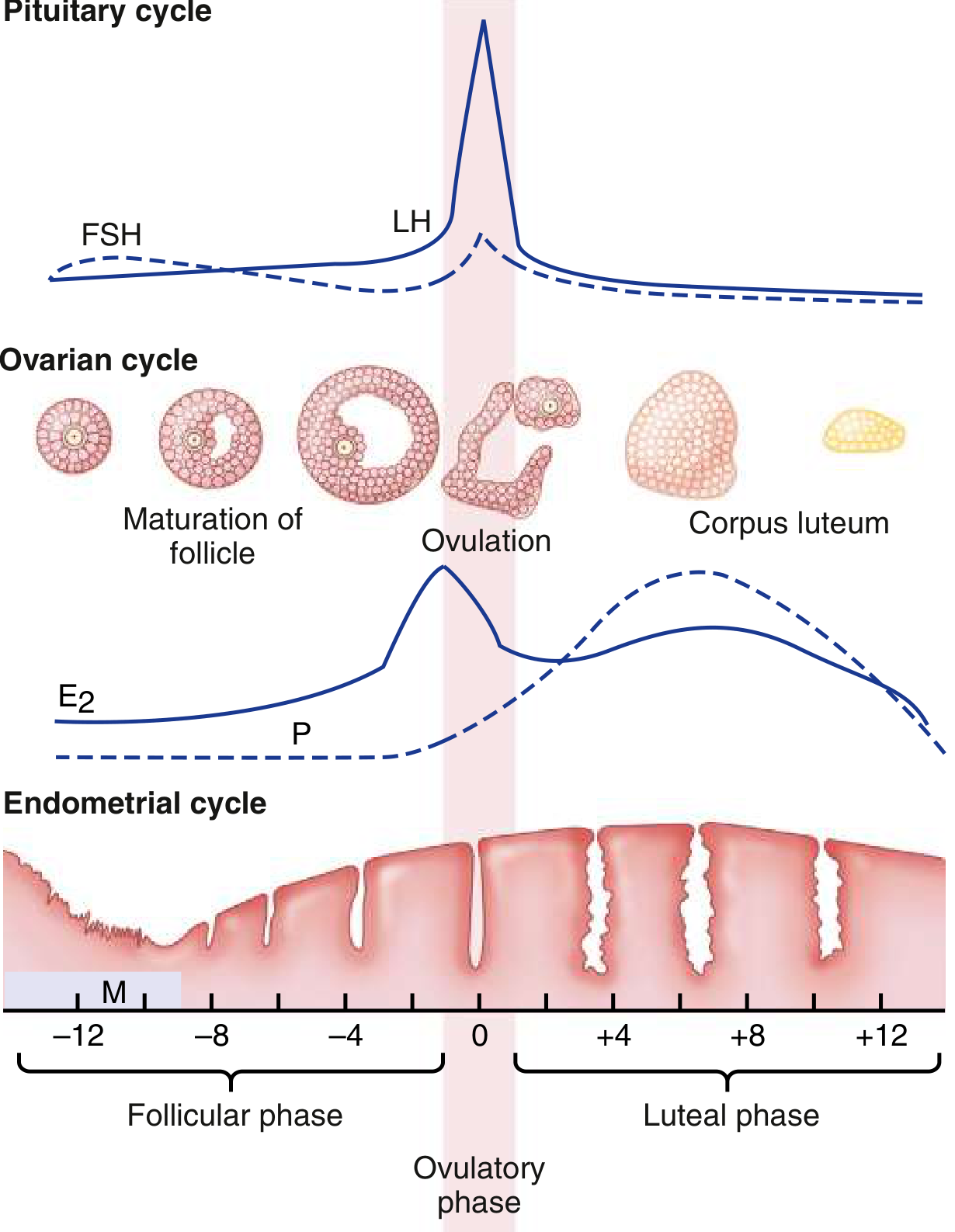
Figure: Idealized cyclic changes in gonadotropins (LH, FSH), estradiol (E2), progesterone (P), and uterine endometrium during the normal menstrual cycle. (Goldman-Cecil Medicine)
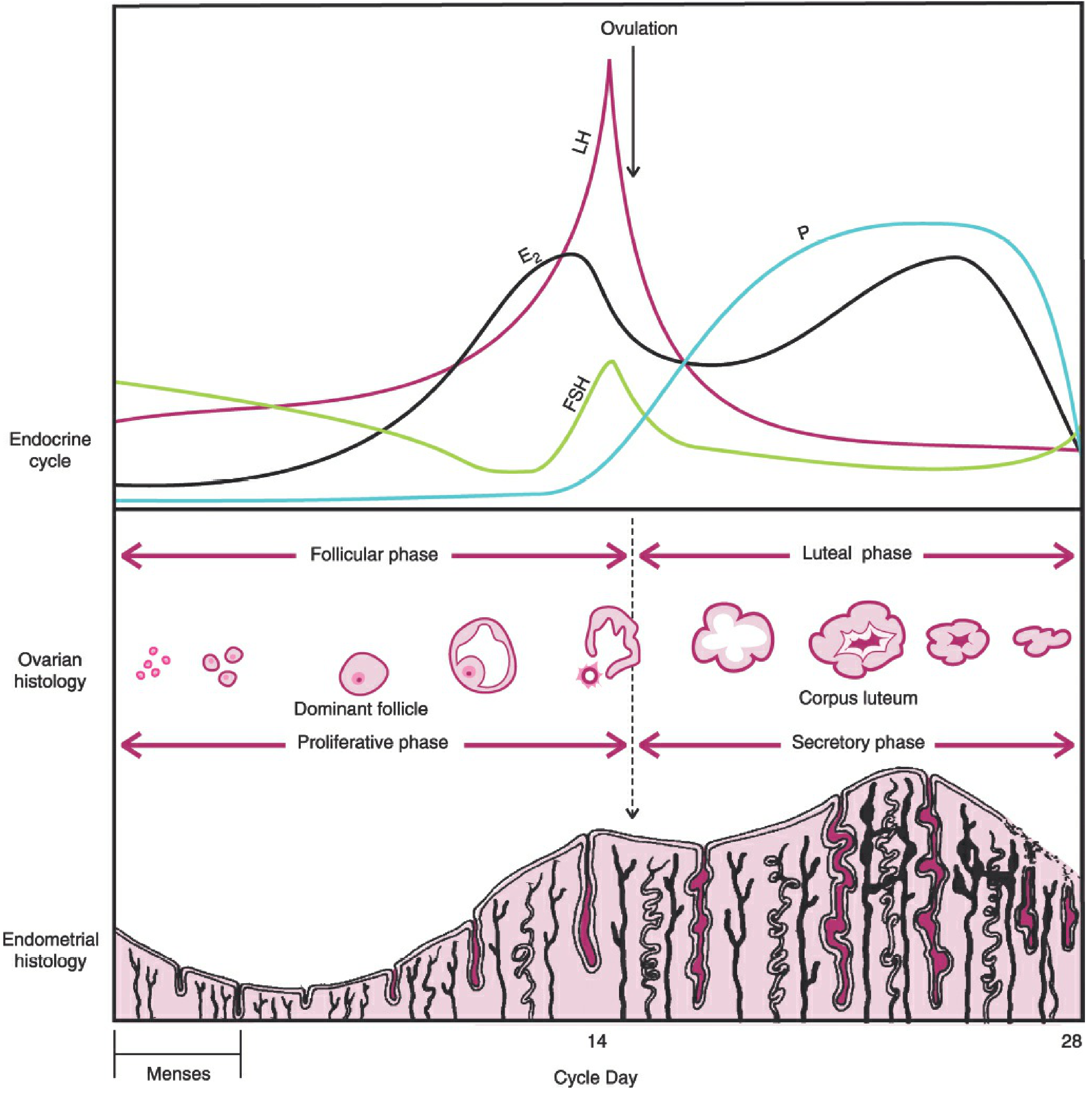
Figure: The menstrual cycle showing FSH, LH, estradiol (E2) and progesterone (P) relative to ovulation, alongside ovarian and endometrial changes. (Berek & Novak's Gynecology)
Sequential Summary of Key Events:
- Days 1-4: Menstruation; estrogen/progesterone low; FSH begins rising as corpus luteum degenerates
- Days 1-7: FSH recruits a cohort of antral follicles; estrogen begins rising from granulosa cell aromatization
- Day ~6: One dominant follicle selected; others undergo atresia
- Days 7-12: Dominant follicle grows to 18-25 mm; estradiol peaks; inhibin B suppresses FSH; endometrium proliferates
- Day ~13: Estradiol positive feedback triggers LH surge (and smaller FSH surge)
- Day ~14: Ovulation 24-36 hours after LH surge; first meiotic division completes; oocyte extruded
- Days 15-22: Corpus luteum forms; progesterone rises; endometrium converts to secretory pattern; cervical mucus thickens; BBT rises
- Day ~21: Progesterone peak; "implantation window" (~days 20-24)
- Days 24-28: Corpus luteum degenerates (if no pregnancy); progesterone/estradiol fall; FSH begins new rise; spiral arteries spasm; endometrium undergoes ischemic necrosis; menstruation begins (day 28/1)
Sources
- Berek & Novak's Gynecology (Menstrual Cycle Physiology, Chapter 7)
- Costanzo Physiology, 7th Edition (Events of the Menstrual Cycle)
- Ganong's Review of Medical Physiology, 26th Edition (The Menstrual Cycle)
- Tietz Textbook of Laboratory Medicine, 7th Edition (Normal Menstrual Cycle)
- Goldman-Cecil Medicine, International Edition (The Normal Menstrual Cycle, Chapter 218)
This is a shared conversation. Sign in to Orris to start your own chat.