Atrial fibrillation ecg changes with findings shows
Reading File
Finding Sources
Finding Sources
Searching Images
atrial fibrillation ECG findings electrocardiogram
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of Atrial Fibrillation (AF) — ECG Changes & Findings, drawn from authoritative medical textbooks (Tintinalli's Emergency Medicine, Guyton & Hall Physiology, and Fuster & Hurst's The Heart).
Atrial Fibrillation — ECG Findings
🔑 Three Cardinal ECG Features
| Feature | Description |
|---|---|
| 1. Absent P waves | No discernible P waves; replaced by a flat, chaotic, or fine undulating (fibrillatory) baseline |
| 2. Fibrillatory (f) waves | Rapid, low-amplitude, irregular baseline oscillations (best seen in V1 and inferior leads); rate 350–600/min |
| 3. Irregularly irregular ventricular rhythm | R-R intervals vary randomly — the hallmark diagnostic feature |
Detailed ECG Analysis
1. P Waves — Absent
Numerous small depolarization waves spread simultaneously in all directions through the atria. Because these waves are weak and many are of opposite polarity at any given time, they electrically neutralize one another. The result is no organized P waves — only a chaotic or near-flat isoelectric baseline.
"One can see either no P waves from the atria or only a fine, high-frequency, very low voltage wave record." — Guyton & Hall Textbook of Medical Physiology
2. Fibrillatory (f) Waves
- Fine, irregular oscillations replace the isoelectric baseline
- Best seen in leads V1 and V2, and sometimes in lead II
- Vary in amplitude, morphology, and timing
- Atrial rate: 350–600 impulses/min
3. Irregularly Irregular R-R Intervals
- The AV node receives impulses randomly and unpredictably
- Refractory period of ~0.35 sec means not all impulses conduct
- Ventricular rate typically 110–160 beats/min (uncontrolled)
- The beat-to-beat variation has no repeating pattern — distinguishing AF from other arrhythmias
4. QRS Complexes
- Usually narrow (normal duration ≤120 ms), because ventricular conduction is normal
- Wide QRS occurs only if:
- Pre-existing bundle branch block (BBB)
- Rate-related aberrant conduction
- Wolff-Parkinson-White (WPW) syndrome / pre-excitation — produces wide, bizarre QRS
Complete ECG Feature Summary (Tintinalli's TABLE 18-8)
TABLE 18-8 — ECG Features of Atrial Fibrillation (Tintinalli's Emergency Medicine)
- Absence of discernible P waves with flat or chaotic isoelectric baseline
- QRS complexes narrow unless pre-existing bundle branch block or pre-excitation syndrome
- Irregularly irregular ventricular rhythm
ECG Images
Figure 1 — Lead II strip showing AF (Guyton & Hall)
The ventricular QRS and T waves are visible, but no P waves — only chaotic undulation of the baseline between beats with clearly variable R-R intervals.

Figure 2 — 12-lead ECG of AF (Fuster & Hurst's The Heart, Fig. 36-5)
Note the rapid, irregular, low-amplitude fibrillatory waves with varying morphology and an irregularly irregular ventricular response across all 12 leads.
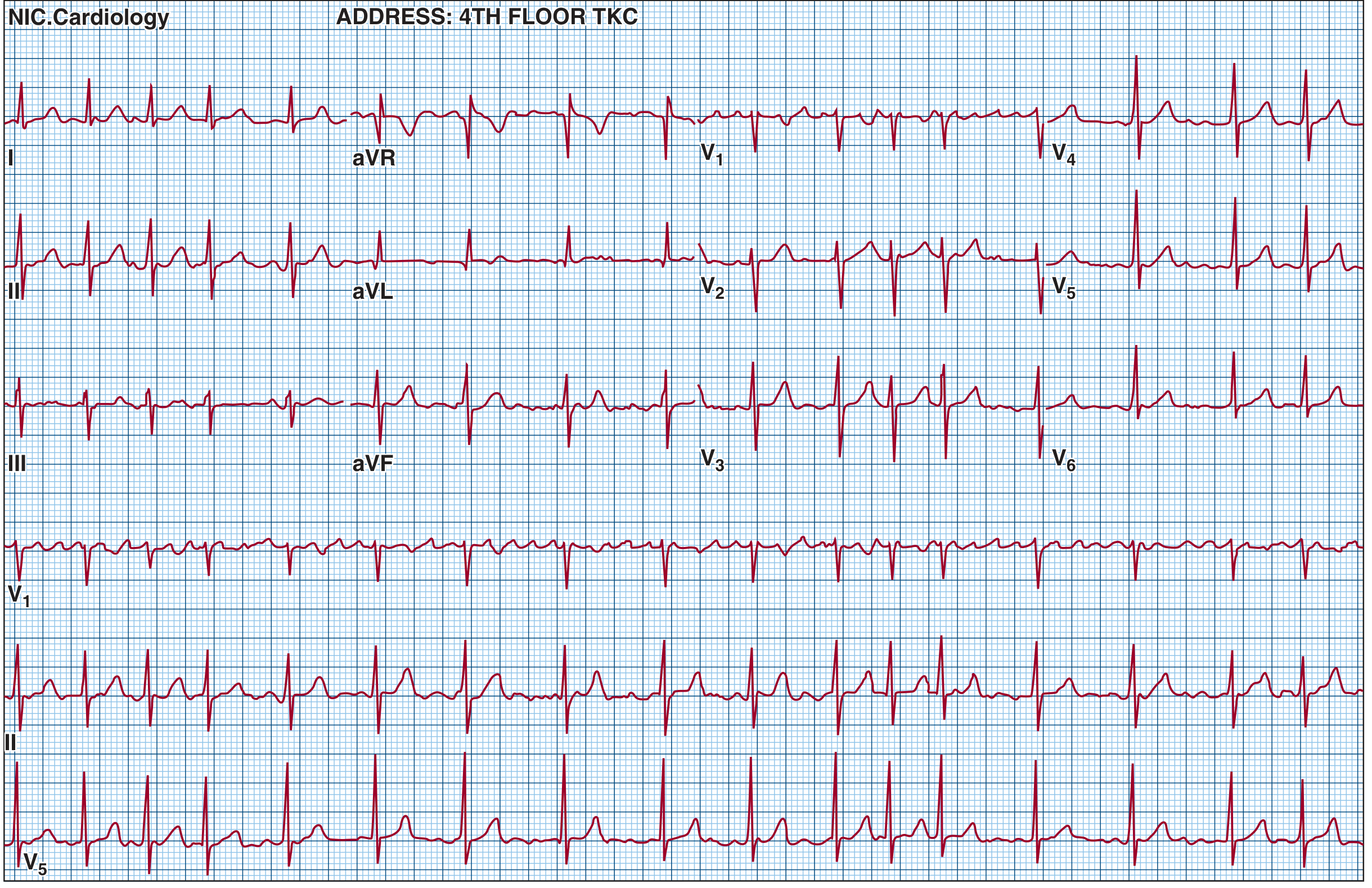
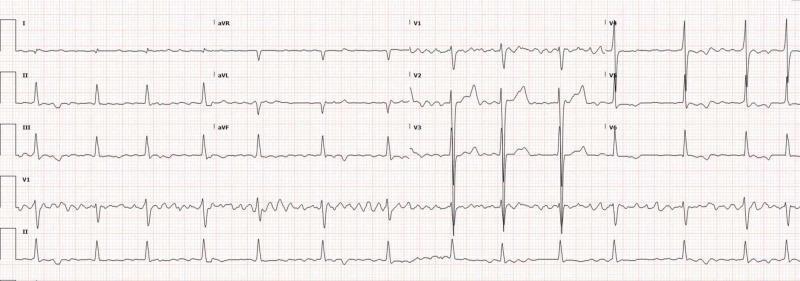
Figure 3 — AF with Rapid Ventricular Response (RVR)
Ventricular rate ~147 bpm. No P waves, fine fibrillatory baseline most visible in inferior leads, narrow QRS, irregularly irregular rhythm.
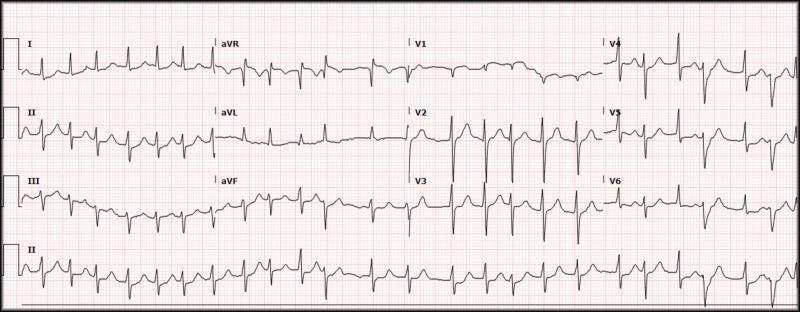
Figure 4 — Rate-controlled AF (12-lead)
Irregularly irregular R-R intervals, complete absence of organized P waves, fine f-waves best visible in V1–V2, narrow QRS complexes with normal ventricular conduction.
Physiology Behind the ECG Changes
The AV node acts as a gatekeeper: it will not transmit a second impulse for ~0.35 seconds after the preceding one. Random atrial impulses arrive unpredictably, so the interval from one QRS to the next varies between ~0.35 and ~0.95 seconds — creating the classic irregularly irregular ventricular rhythm.
Special Situations
| Situation | ECG Appearance |
|---|---|
| AF + WPW | Wide, bizarre QRS (delta wave); very rapid rate; dangerous (can degenerate to VF) |
| AF + BBB | Wide QRS, but rhythm remains irregularly irregular |
| AF + Digitalis toxicity | Regularized ventricular rate (70–130 bpm) with QRS complexes superimposed on fibrillatory waves — suggests complete heart block |
| AF with slow ventricular rate | Suggests AV nodal disease or drug effect |
Quick Diagnostic Checklist
- No P waves visible anywhere in 12 leads
- Baseline shows chaotic/fine undulating f-waves (look in V1, II)
- R-R intervals completely irregular with no repeating pattern
- QRS narrow (unless BBB or WPW co-exists)
- Ventricular rate typically 110–160/min if uncontrolled
Sources: Tintinalli's Emergency Medicine (Table 18-8), Guyton and Hall Textbook of Medical Physiology (Fig. 13.20), Fuster and Hurst's The Heart 15th Ed. (Fig. 36-5)
This is a shared conversation. Sign in to Orris to start your own chat.