Pleural effusion and abscess from harrison. Make a concise note with images
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the images and content needed. Let me compile the comprehensive note.
Pleural Effusion & Lung Abscess
Harrison's Principles of Internal Medicine, 22e
PART I: PLEURAL EFFUSION
Definition & Pathophysiology
A pleural effusion is excess fluid in the pleural space. Normally, fluid enters from parietal pleural capillaries and exits via parietal pleural lymphatics (which can absorb 20x normal fluid load). An effusion forms when hydrostatic-oncotic imbalance overwhelms lymphatic drainage. ~1.5 million Americans are affected per year. Presenting symptoms: dyspnea and pleuritic chest pain.
Transudate vs. Exudate: Light's Criteria
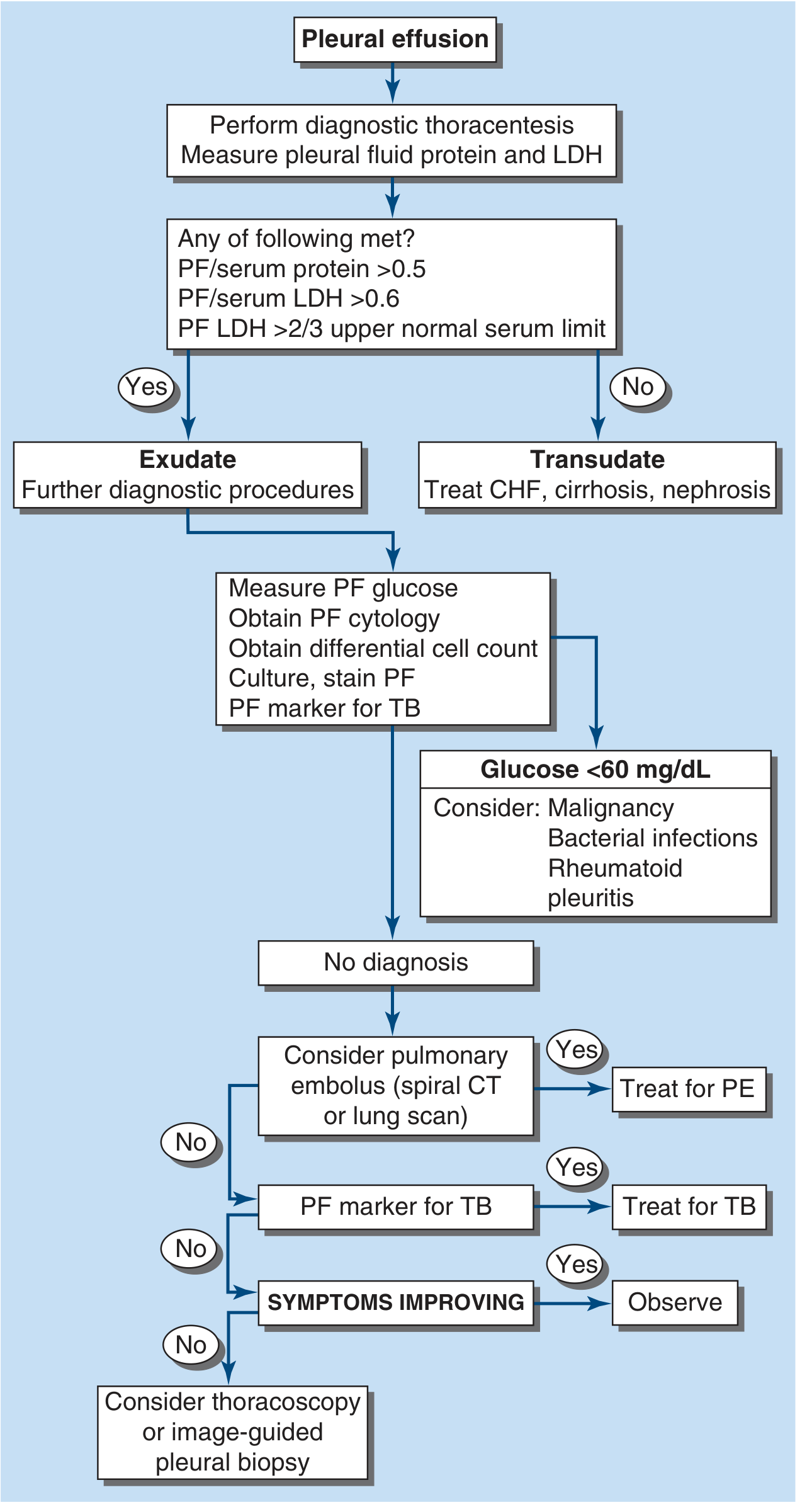
An effusion is an exudate if it meets ANY of the following (otherwise transudate):
| Criterion | Threshold |
|---|---|
| Pleural fluid protein / serum protein | >0.5 |
| Pleural fluid LDH / serum LDH | >0.6 |
| Pleural fluid LDH | >2/3 upper normal serum limit |
Pseudoexudates: Light's criteria misidentify ~25% of transudates as exudates (often "diuresed transudates"). If clinical suspicion favors a transudate, use: Serum-PF protein gradient >3.1 g/dL OR serum-PF albumin gradient >1.2 g/dL - these identify pseudoexudates with ~99-100% sensitivity.
Diagnostic Algorithm
Causes
Transudates
- Congestive heart failure (most common)
- Cirrhosis
- Nephrotic syndrome
- Peritoneal dialysis
- Superior vena cava obstruction
- Myxedema, Urinothorax
Exudates
- Bacterial pneumonia / parapneumonic (most common exudative cause in USA)
- Malignancy (lung, breast, lymphoma = 75% of malignant effusions)
- Tuberculosis (most common cause worldwide)
- Pulmonary embolism (most commonly overlooked)
- Viral infections
- Collagen vascular disease (RA, SLE)
- GI disease (esophageal perforation, pancreatitis, intra-abdominal abscess)
- Chylothorax, hemothorax
Key Specific Effusions
Parapneumonic Effusion (PPE)
- Occurs in up to 50% of community-acquired pneumonia
- Usually reactive (sterile cultures)
- 10% progress to complicated PPE or empyema (fibrinopurulent or grossly purulent fluid)
- Indicators requiring drainage (chest tube or intervention):
- Loculated fluid
- pH <7.20
- Glucose <3.3 mmol/L (<60 mg/dL)
- Positive Gram stain or culture
- Gross pus (empyema)
- PF LDH >900 IU/L
Malignant Effusion
- Second most common exudate; poor prognosis (<6-month survival)
- Lung, breast, lymphoma = ~75%
- Usually exudate; reduced glucose if high tumor burden
- Diagnosis: cytology. If negative x2, consider thoracoscopic biopsy
- Treatment: therapeutic thoracentesis, indwelling pleural catheter (IPC), or pleurodesis with talc
Tuberculous Pleuritis
- Predominantly lymphocytic exudate
- Markers: adenosine deaminase >40 IU/L or IFN-γ >140 pg/mL
- Diagnosis: pleural biopsy culture (higher yield than fluid); thoracoscopy
Chylothorax
- Thoracic duct disruption (trauma/surgery or mediastinal tumor)
- Milky fluid; triglycerides >1.2 mmol/L (110 mg/dL)
- Treatment: chest tube + octreotide + eliminate enteral fat; if refractory - percutaneous thoracic duct blockage or ligation
Hemothorax
- PF hematocrit >50% of peripheral blood hematocrit
- Most from trauma; treat with tube thoracostomy
- If bleeding >200 mL/h: consider angiographic embolization or surgery
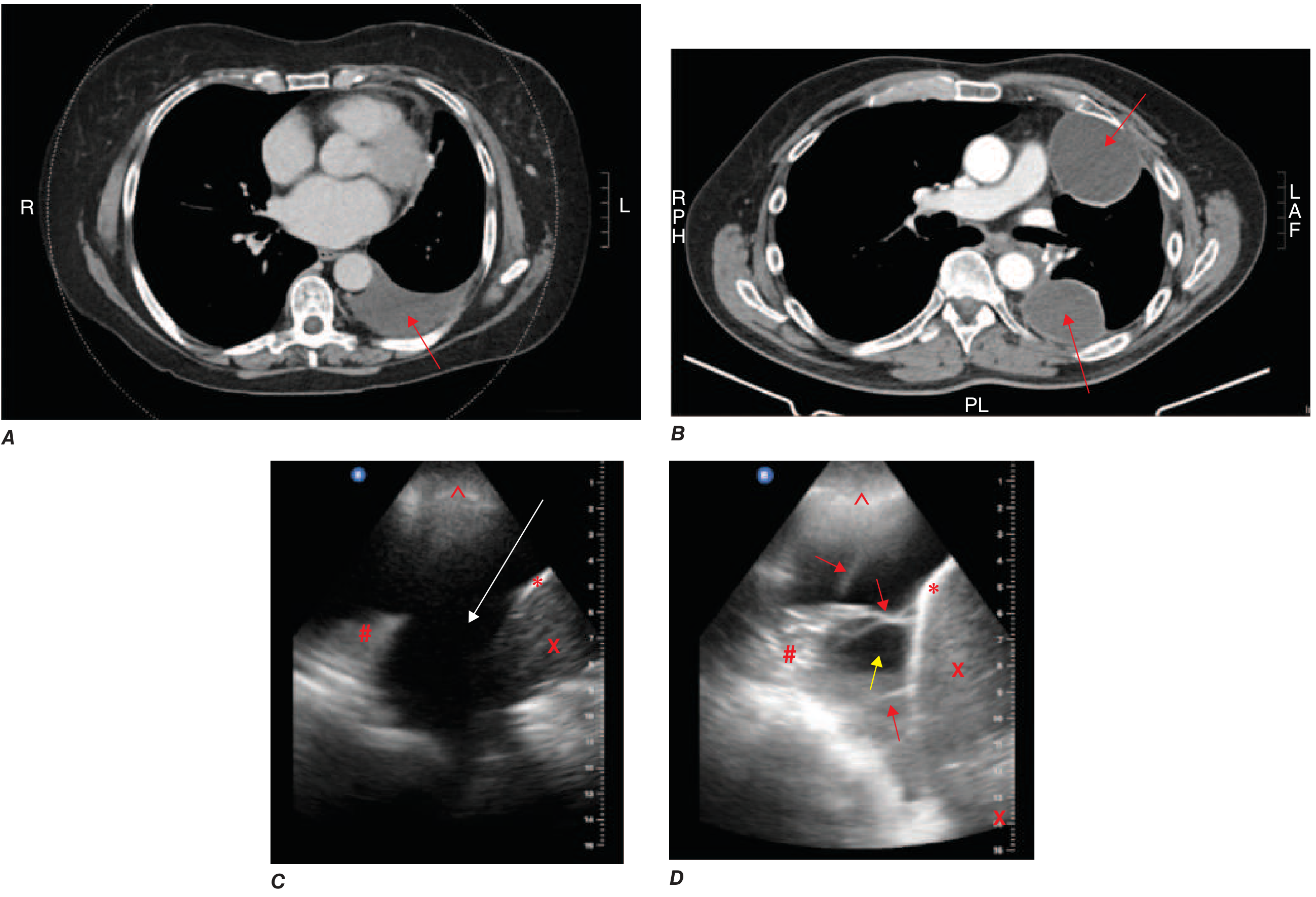
Imaging of Pleural Effusion
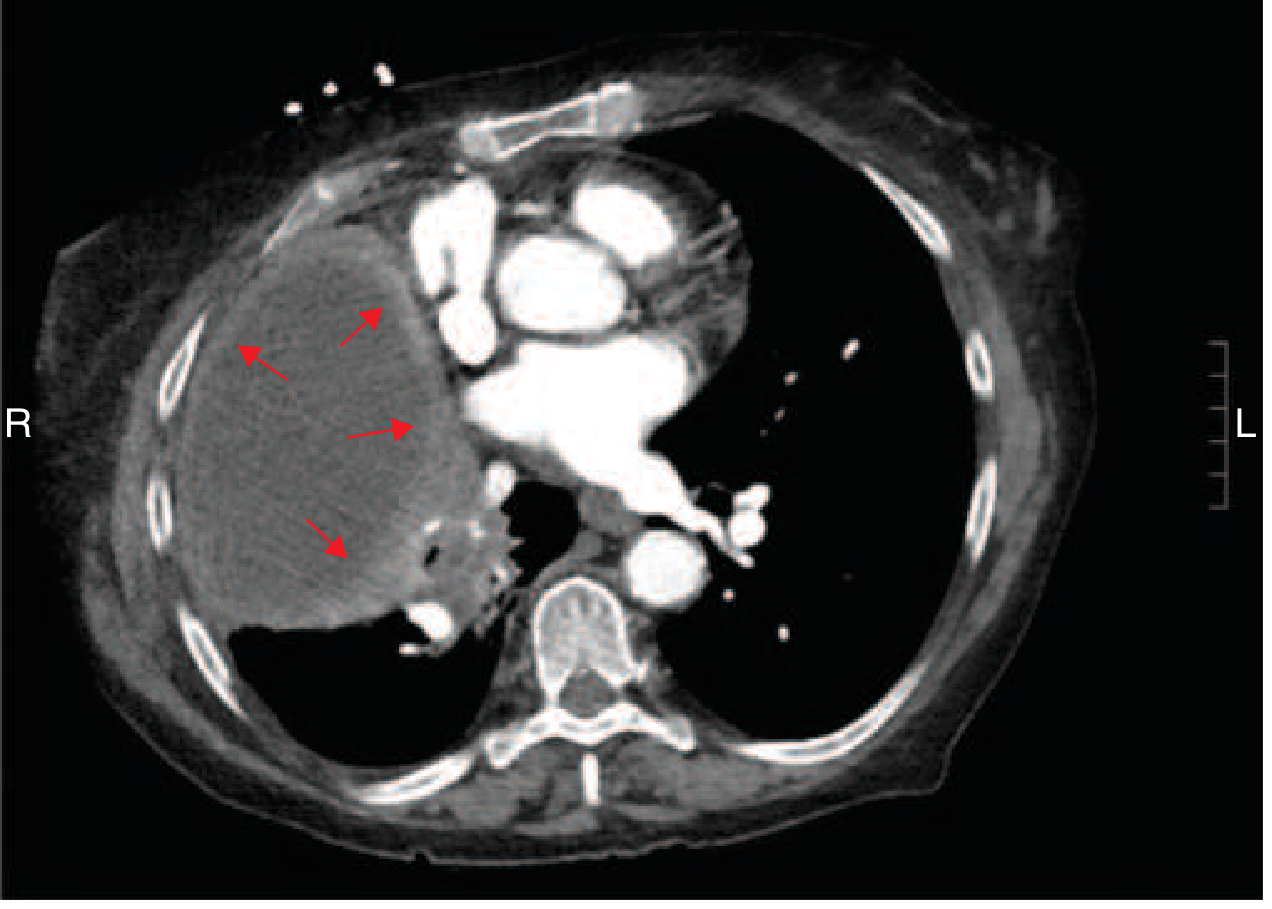
Empyema CT
Management of Parapneumonic Effusion/Empyema
- Simple PPE - antibiotic treatment of pneumonia; no drainage needed
- Complicated PPE (criteria above) - chest tube drainage
- Fibrinopurulent stage (cannot fully drain) - intrapleural tPA (10 mg) + DNase (5 mg), or VATS/thoracoscopy to break adhesions
- Organized stage (pleural peel) - surgical decortication
- Trapped lung - pleural manometry; decortication if needed
PART II: LUNG ABSCESS
Definition
Necrosis and cavitation of lung parenchyma due to microbial infection. Usually a single dominant cavity >2 cm. Can be single or multiple.
Classification
| Type | Description |
|---|---|
| Primary (~80%) | Aspiration-related; anaerobic organisms; no underlying condition |
| Secondary (~20%) | Underlying condition: obstruction (tumor, foreign body), immunocompromise |
| Acute | <4-6 weeks |
| Chronic (~40%) | >4-6 weeks duration |
Epidemiology & Risk Factors
- More common in middle-aged men
- Major risk factor: aspiration
- At-risk groups: altered mental status, alcoholism, drug overdose, seizures, bulbar dysfunction, stroke, neuromuscular disease, esophageal dysmotility/obstruction, GERD
- Periodontal disease / gingivitis - anaerobic colonization of gingival crevices is critical; lung abscess is extremely rare in edentulous patients
Microbiology (Table 132-1)
| Clinical Setting | Pathogens |
|---|---|
| Primary (aspiration) | Anaerobes: Peptostreptococcus, Prevotella, Bacteroides, milleri group streptococci; microaerophilic streptococci |
| Secondary (immunocompromise) | S. aureus, Gram-negatives (Pseudomonas, Enterobacteriaceae), Nocardia, Aspergillus, Mucorales, Cryptococcus, Legionella, Rhodococcus equi, PCP |
| Embolic lesions | S. aureus (endocarditis), Fusobacterium necrophorum (Lemierre's syndrome) |
| Endemic fungi/TB | M. tuberculosis, Coccidioides, Histoplasma, Blastomyces; parasites (E. histolytica, Paragonimus) |
| Post-viral | S. aureus after influenza; Actinomyces |
Pathogenesis
Primary: Aspirated anaerobes from gingival crevices → pneumonitis (worsened by gastric acid) → over 7-14 days → parenchymal necrosis and cavitation. Polymicrobial synergy worsens tissue destruction.
Secondary: Depends on predisposing factor (e.g., bronchial obstruction → distal infection; hematogenous seeding in immunocompromise).
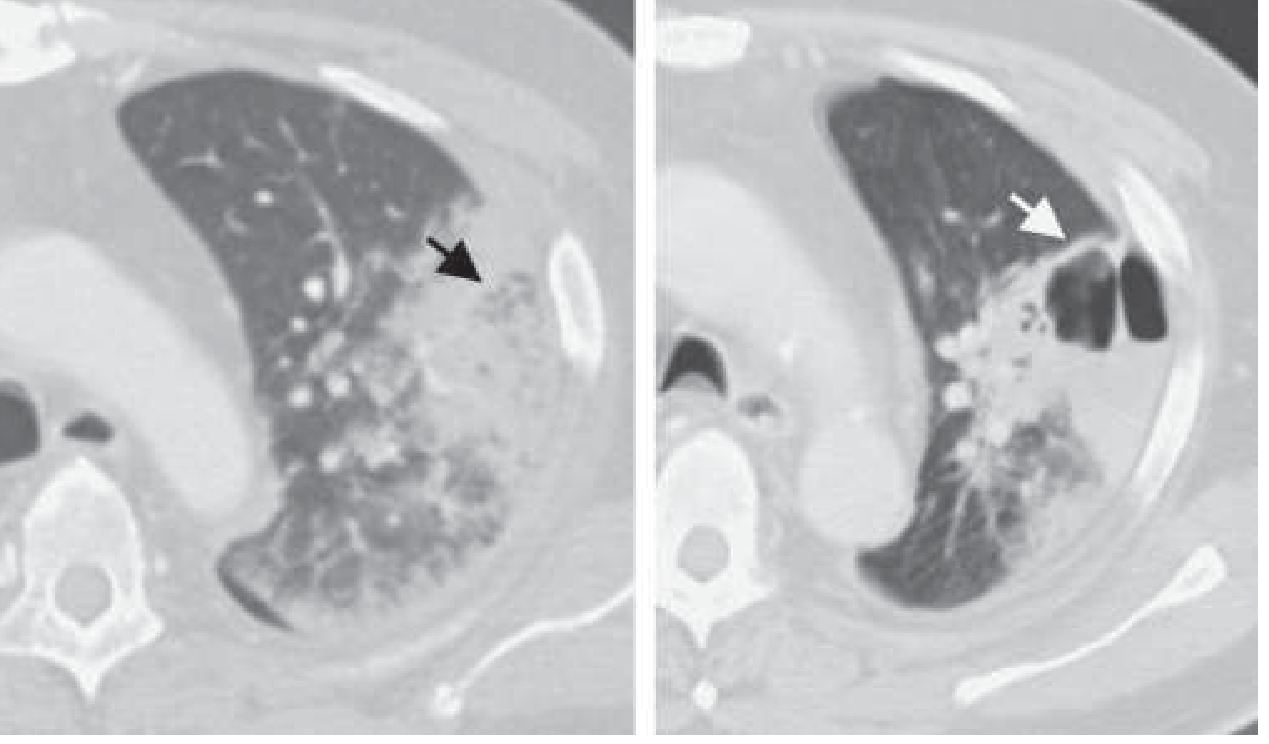
CT of Lung Abscess
Clinical Features
- Subacute presentation is typical for primary (anaerobic): weight loss, low-grade fever, mild anemia, leukocytosis, history of aspiration risk
- Putrid-smelling sputum = virtually diagnostic of anaerobic infection
- Pleuritic chest pain and productive cough
- Large effusion with minimal infiltrate may occur (especially anaerobic)
Differential Diagnosis of Cavitary Lung Lesion
- Lung infarction
- Malignancy (cavitating tumor)
- Pulmonary sequestration
- Cryptogenic organizing pneumonia
- Sarcoidosis, vasculitis (GPA/Wegener)
- Lung cysts/bullae with fluid
- Septic emboli (tricuspid endocarditis)
Diagnosis
- Chest X-ray: thick-walled cavity with air-fluid level
- CT chest: better definition; earlier cavitation; identifies underlying cause (malignancy); distinguishes peripheral lung abscess from empyema (critical distinction for treatment)
- Sputum: Gram stain + culture (may miss anaerobes; likely polymicrobial)
- Molecular methods (16S rRNA gene amplification) - increasingly used
- Secondary abscesses / failed empirical therapy: sputum + blood cultures, serology for fungi/viruses, bronchoscopy with BAL or protected brush, CT-guided needle aspiration (risks: contralateral spillage, pneumothorax, bronchopleural fistula)
- Bronchoscopy early if bronchial obstruction suspected
Treatment
Antibiotics (primary treatment):
| Regimen | Details |
|---|---|
| Clindamycin (preferred) | 600 mg IV TID → when afebrile: 300 mg PO QID |
| IV β-lactam/β-lactamase inhibitor | e.g., ampicillin-sulbactam → then oral amoxicillin-clavulanate |
| Moxifloxacin | 400 mg/d PO (evidence: as effective as ampicillin-sulbactam) |
Why clindamycin over penicillin? - Oral anaerobes can produce β-lactamases; clindamycin proved superior to penicillin in clinical trials.
Duration: Continue until imaging shows resolution or small scar.
- Typically 3-4 weeks to 14 weeks
- At least 6 weeks may be associated with better outcomes
- Chronic abscesses may need longer courses
Drainage:
- Spontaneous drainage via bronchial tree is most common
- Percutaneous CT-guided catheter drainage - systematic reviews support use for selected cases; consider when medical therapy fails or if patient is a poor surgical candidate
- Surgery (lobectomy/segmentectomy) - reserved for: failed medical therapy, massive hemoptysis, suspected malignancy, bronchopleural fistula, or inability to rule out cancer
Source: Harrison's Principles of Internal Medicine, 22e (2025) - Chapter 132: Lung Abscess; Chapter 305: Pleural Effusion
This is a shared conversation. Sign in to Orris to start your own chat.