Uses of cholinergic drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information. Let me compile the complete answer on uses of cholinergic drugs.
Uses of Cholinergic Drugs
Cholinergic drugs mimic or enhance the action of acetylcholine (ACh). They are broadly divided into direct-acting agonists (choline esters and alkaloids) and indirect-acting agents (anticholinesterases / cholinesterase inhibitors).
Classification
| Group | Subclass | Examples |
|---|---|---|
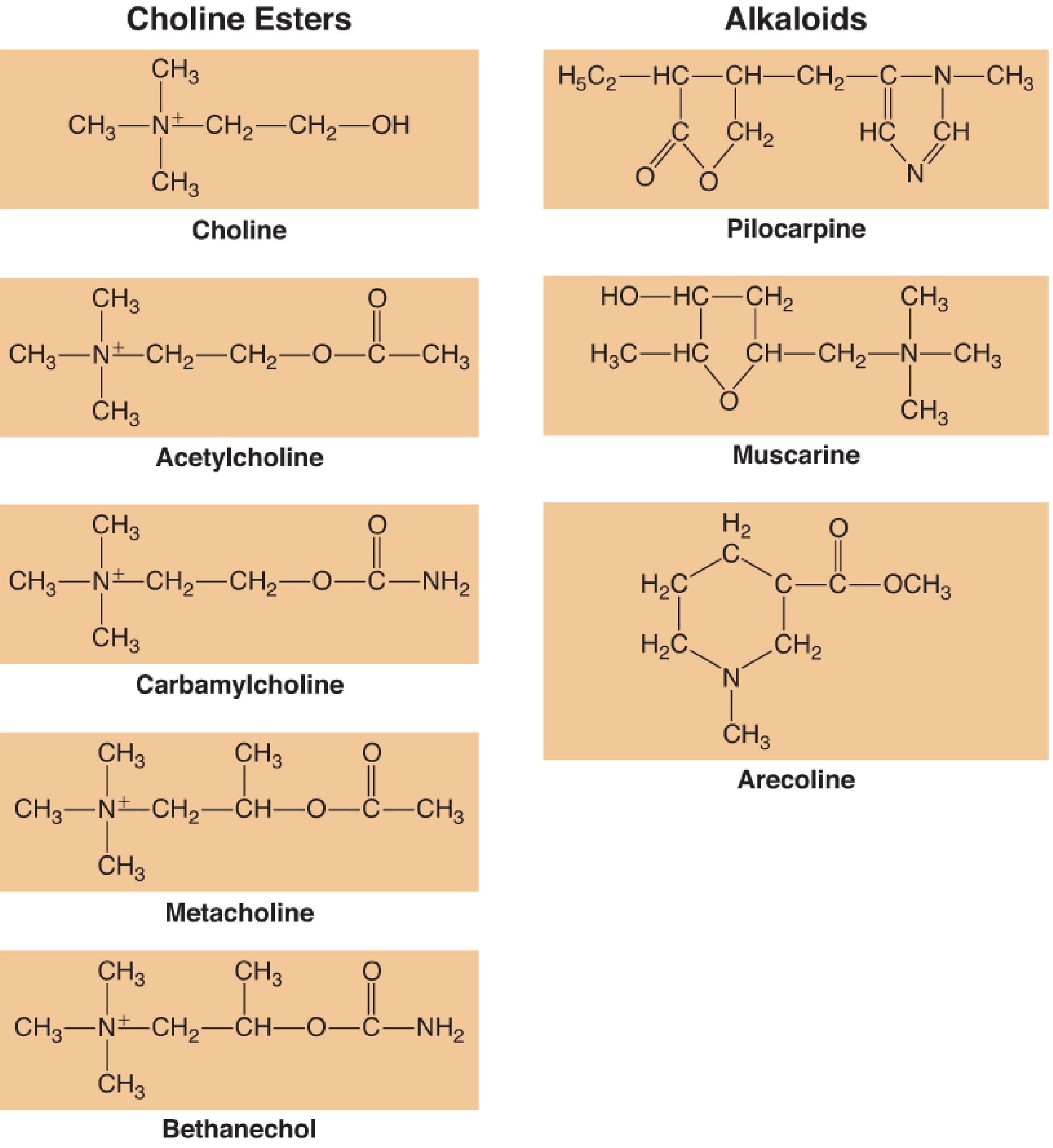
| Direct-acting | Choline esters | ACh, methacholine, bethanechol, carbamylcholine (carbachol) |
| Direct-acting | Alkaloids | Pilocarpine, muscarine, arecoline |
| Indirect-acting | Reversible anticholinesterases | Physostigmine, neostigmine, pyridostigmine, edrophonium |
| Indirect-acting | Irreversible anticholinesterases | Echothiophate, organophosphates |
Figure 14-13: Chemical structures of direct-acting cholinomimetic esters and alkaloids.
1. Direct-Acting Cholinergic Agonists
Acetylcholine (ACh)
- Has almost no systemic therapeutic use due to rapid hydrolysis by cholinesterase and diffuse, non-selective action.
- Topical ACh 1% eye drops: used during cataract extraction to produce rapid miosis (pupil constriction) intraoperatively. Systemic effects are negligible because it is hydrolyzed quickly.
Methacholine
- Primarily a muscarinic agonist; more resistant to hydrolysis than ACh.
- Bronchial provocation test (inhaled): diagnoses bronchial hyperreactivity in asthma by inducing bronchoconstriction.
- Supraventricular tachyarrhythmias (especially paroxysmal tachycardia): slows the heart when other measures fail.
- Also increases intestinal tone.
- Contraindicated in asthmatic patients and those with hypertension (may cause severe hypotension). Overdose treated with atropine.
Bethanechol
- Resistant to hydrolysis; selective for GI and urinary tracts; minimal cardiac effects.
- Urinary retention / neurogenic bladder atony: stimulates detrusor muscle contraction.
- Postoperative / postpartum GI atony: restores bowel motility.
- Gastroesophageal reflux disease (GERD): increases lower esophageal sphincter tone and gastric emptying.
Carbamylcholine (Carbachol)
- Has both muscarinic AND nicotinic activity.
- Glaucoma: topical for open-angle (wide-angle) glaucoma - reduces intraocular pressure by causing miosis and facilitating aqueous outflow.
- Intraocular miosis: used during ophthalmic surgery.
Pilocarpine (Alkaloid)
- A natural alkaloid; acts at muscarinic receptors.
- Glaucoma (open-angle and angle-closure): the most widely used miotic; lowers intraocular pressure.
- Xerostomia (dry mouth): used in patients with Sjogren's syndrome or after radiation therapy to head and neck (stimulates salivary secretion).
- Diagnosis of cystic fibrosis: pilocarpine iontophoresis sweat test - stimulates eccrine sweat glands to collect sweat for chloride measurement.
2. Indirect-Acting Agents (Anticholinesterases / Cholinesterase Inhibitors)
These drugs inhibit the enzyme acetylcholinesterase, preventing breakdown of ACh and thereby amplifying cholinergic transmission at all sites.
Physostigmine
- Tertiary amine - crosses the blood-brain barrier (BBB).
- Central anticholinergic syndrome: reversal of central effects of anticholinergic overdose (atropine, tricyclic antidepressants, antihistamines) - agitation, delirium, hallucinations.
- Glaucoma: historically used topically; largely replaced by newer agents.
Neostigmine
- Quaternary amine - does NOT cross BBB (peripheral effects predominate).
- Reversal of non-depolarizing neuromuscular blockade: most common clinical use in anesthesia (reverses vecuronium, rocuronium, atracurium). Given with glycopyrrolate to prevent muscarinic side effects.
- Myasthenia gravis: symptomatic treatment by increasing ACh at the neuromuscular junction.
- Postoperative urinary retention and paralytic ileus.
Pyridostigmine
- Quaternary amine; longer duration than neostigmine.
- Myasthenia gravis: the drug of choice for long-term symptomatic management.
- Reversal of neuromuscular blockade (less commonly than neostigmine).
- Prophylaxis against nerve agent (soman) exposure in military personnel.
Edrophonium
- Very short-acting (minutes).
- Tensilon (edrophonium) test: diagnosis of myasthenia gravis - transient improvement in muscle weakness confirms the diagnosis.
- Differentiation of myasthenic crisis vs. cholinergic crisis.
- Reversal of non-depolarizing neuromuscular blockade (short procedures).
Echothiophate (Irreversible)
- Organophosphate; available as topical ophthalmic drops.
- Glaucoma: prolonged duration of action (2-3 weeks after stopping); used when other agents fail.
- Note: reduces pseudocholinesterase activity, causing prolonged action of succinylcholine - important anesthetic concern.
Donepezil, Rivastigmine, Galantamine
- Reversible cholinesterase inhibitors; CNS-active.
- Alzheimer's disease: first-line symptomatic treatment; slow cognitive decline.
- Dementia with Lewy bodies, vascular dementia.
- Rivastigmine also approved for Parkinson's disease dementia.
3. Summary of Key Clinical Uses by Indication
| Clinical Indication | Drug(s) Used |
|---|---|
| Glaucoma | Pilocarpine, carbachol, echothiophate |
| Myasthenia gravis (acute diagnosis) | Edrophonium (Tensilon test) |
| Myasthenia gravis (long-term) | Pyridostigmine, neostigmine |
| Reversal of neuromuscular blockade | Neostigmine + glycopyrrolate |
| Alzheimer's disease / dementia | Donepezil, rivastigmine, galantamine |
| Bladder atony / urinary retention | Bethanechol |
| GERD / GI atony | Bethanechol |
| Central anticholinergic toxidrome | Physostigmine |
| Bronchial provocation (asthma Dx) | Methacholine (inhaled) |
| Xerostomia (Sjogren's, radiation) | Pilocarpine |
| Intraoperative miosis (cataract) | Topical ACh (1%) |
| Cystic fibrosis sweat test | Pilocarpine iontophoresis |
| Nerve agent prophylaxis | Pyridostigmine |
| Organophosphate poisoning antidote | Atropine + pralidoxime (antagonist approach) |
Key Points
- All cholinergic drugs act through either muscarinic or nicotinic receptors (or both), mimicking parasympathetic stimulation.
- Adverse effects of excess cholinergic activity follow the "SLUDGE" mnemonic: Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis. Bradycardia, bronchoconstriction, and miosis are also seen.
- The antidote for cholinergic toxicity/overdose is atropine (muscarinic blocker); pralidoxime is used specifically for organophosphate poisoning to reactivate cholinesterase.
- Cholinesterase inhibitors used in anesthesia (neostigmine) require co-administration of an antimuscarinic (atropine or glycopyrrolate) to block unwanted muscarinic side effects while allowing nicotinic reversal at the neuromuscular junction.
Sources: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, pp. 1076-1084; Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 413-414
This is a shared conversation. Sign in to Orris to start your own chat.