A 14 years girl with abdominal pain and blood in vomit for 1 day the differential diagnosis is
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have excellent, detailed data from the textbook. Let me compose the comprehensive answer.
Differential Diagnosis: 14-Year-Old Girl with Abdominal Pain + Hematemesis (Blood in Vomit)
This is a upper GI bleeding (UGIB) presentation in an adolescent. The combination of abdominal pain + hematemesis narrows the differential considerably compared to painless bleeding. Here is a systematic breakdown:
Most Common (Likely) Causes in Adolescents
| Diagnosis | Key Features |
|---|---|
| Gastritis / H. pylori gastritis | Epigastric burning pain, nausea, history of NSAID use, H. pylori infection common in this age group |
| Peptic Ulcer Disease (PUD) | Epigastric pain, may be relieved by food; H. pylori or NSAID-related |
| Mallory-Weiss Tear | Longitudinal mucosal tear at gastro-esophageal junction after forceful vomiting; preceded by retching |
| Esophagitis | Heartburn, dysphagia, acid reflux; GERD-related |
"The adolescent will describe epigastric burning pain in a pattern more typical of adult presentations." - Tintinalli's Emergency Medicine
Less Common but Important Causes
| Diagnosis | Key Features |
|---|---|
| Esophageal / Gastric Varices | History of liver disease, portal hypertension (e.g., biliary atresia, cirrhosis); massive painless or painful bleeding |
| Coagulopathy / Bleeding Diathesis | Easy bruising, prolonged bleeding elsewhere, underlying hematologic disorder (von Willebrand, thrombocytopenia) |
| Crohn's Disease | Chronic abdominal pain, diarrhea, weight loss, perianal lesions, aphthous ulcers |
| Toxic / Caustic Ingestion | History of ingesting corrosives, medications (aspirin, NSAIDs, iron, steroids) |
| Bowel Obstruction | Vomiting, absent bowel sounds, distension |
| Henoch-Schonlein Purpura (HSP/IgA vasculitis) | Purpuric rash on lower limbs/buttocks, joint pain, abdominal pain, hematuria |
| Vascular Malformation / Dieulafoy's Lesion | Rare; sudden, massive bleeding from an aberrant submucosal vessel |
| GI Stromal Tumors | Rare but must be considered in adolescents with unexplained GI bleeding |
| Foreign Body | History of ingestion |
Symptom Complex Guide
Based directly on Table 134-3 from Tintinalli's Emergency Medicine:
- Hematemesis + abdominal/epigastric pain --> Peptic ulcer disease, H. pylori gastritis, esophagitis/gastritis, coagulopathy
- Hematemesis + underlying systemic disease --> Esophageal varices, inflammatory bowel disease
- Vomiting + hematochezia + abdominal pain --> Intussusception, malrotation/volvulus, Henoch-Schonlein purpura, ischemic bowel
Do Not Miss - Red Flags Requiring Urgent Action
- Esophageal varices - massive hemorrhage, hemodynamic instability
- Coagulopathy - check PT/INR/APTT, CBC
- Bowel obstruction / ischemia - rigid abdomen, peritoneal signs
- HSP - look for rash, joint swelling, proteinuria
Non-GI Sources to Exclude First
Before assuming GI origin, always rule out:
- Epistaxis (swallowed blood from nose)
- Oropharyngeal/dental bleeding (swallowed blood)
- Pulmonary source (hemoptysis mistaken for hematemesis)
Summary by Priority for a 14-Year-Old Girl
- H. pylori gastritis (most common cause of upper GI bleeding in adolescents)
- Peptic ulcer disease (NSAID use? Stress?)
- Mallory-Weiss tear (forceful vomiting?)
- Reflux esophagitis
- Esophageal varices (if liver disease or portal hypertension present)
- Coagulopathy (bleeding diathesis)
- IBD / Crohn's disease
- HSP / vasculitis
- Toxic ingestion (medication history)
- GI stromal tumors / vascular malformations (rare)
Initial workup should include: CBC, coagulation studies (PT/INR, APTT), metabolic panel, liver function tests, BUN/creatinine (elevated BUN with normal creatinine suggests UGIB), blood type & crossmatch, nasogastric lavage to confirm upper GI source, and urgent gastroenterology/endoscopy referral.
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Table 134-1 & 134-3
Henoch-Schonlein Purpura
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Henoch-Schonlein purpura"[MeSH Terms] AND "IgA vasculitis"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have a thorough body of data from four major textbooks. Let me deliver the comprehensive answer.
Henoch-Schonlein Purpura (IgA Vasculitis)
Note: The current preferred name is IgA Vasculitis (IgAV). The eponym "Henoch-Schonlein Purpura (HSP)" remains widely used clinically.
Definition
IgA vasculitis is an immune complex (IC)-mediated small vessel vasculitis defined by IgA-dominant immune deposits affecting capillaries, venules, and arterioles. It typically involves the skin, gut, glomeruli, and joints.
- Chapel Hill Consensus: "Vasculitis with IgA-dominant immune deposits, affecting small blood vessels; typically involves skin, gut, and glomeruli and is associated with arthralgias or arthritis."
- It is the most common vasculitis of childhood.
Epidemiology
- Peak age: 2-8 years (75% of cases are in children); adults are also affected
- Peak incidence: winter months
- Slight male predominance
- Preceded by upper respiratory tract infection in 30-50% of patients (viral or streptococcal pharyngitis most common)
- H. pylori infection implicated in some cases
Pathophysiology
The central mechanism involves aberrant IgA1 glycosylation:
- A fraction of IgA1 molecules has deficient galactosylation (galactose-deficient IgA1, Ga-IgA1) - the O-linked glycans terminate in GalNAc instead of galactose
- Anti-glycan antibodies recognize these aberrant IgA1 molecules
- IgG-IgA1 immune complexes form in circulation
- These complexes deposit in vessel walls of skin, joints, kidneys, and gut
- This triggers leukocytoclastic angiitis and inflammation
A "second hit" (infection, drug, or other environmental trigger) is required in addition to elevated Ga-IgA1 to produce clinical disease.
Classic Tetrad of Features
| System | Manifestation |
|---|---|
| Skin | Palpable purpura (lower extremities/buttocks) |
| GI Tract | Colicky abdominal pain, GI bleeding |
| Joints | Arthralgias / arthritis (knees, ankles) |
| Kidneys | Hematuria, proteinuria, glomerulonephritis |
Not all four features need to be present simultaneously.
Clinical Features in Detail
1. Skin (100% of established cases)
- Starts as macular rash, becomes hemorrhagic palpable purpura within 1 day
- Located on extensor surfaces of lower limbs, buttocks, occasionally upper extremities
- Does not blanch on pressure
- New crops may appear over weeks to months
- Urticarial lesions, vesicles, or necrotic purpura may also occur
- "Koebnerization" - linear purpura along pressure lines
- Purpura above the waist is a marker of renal involvement
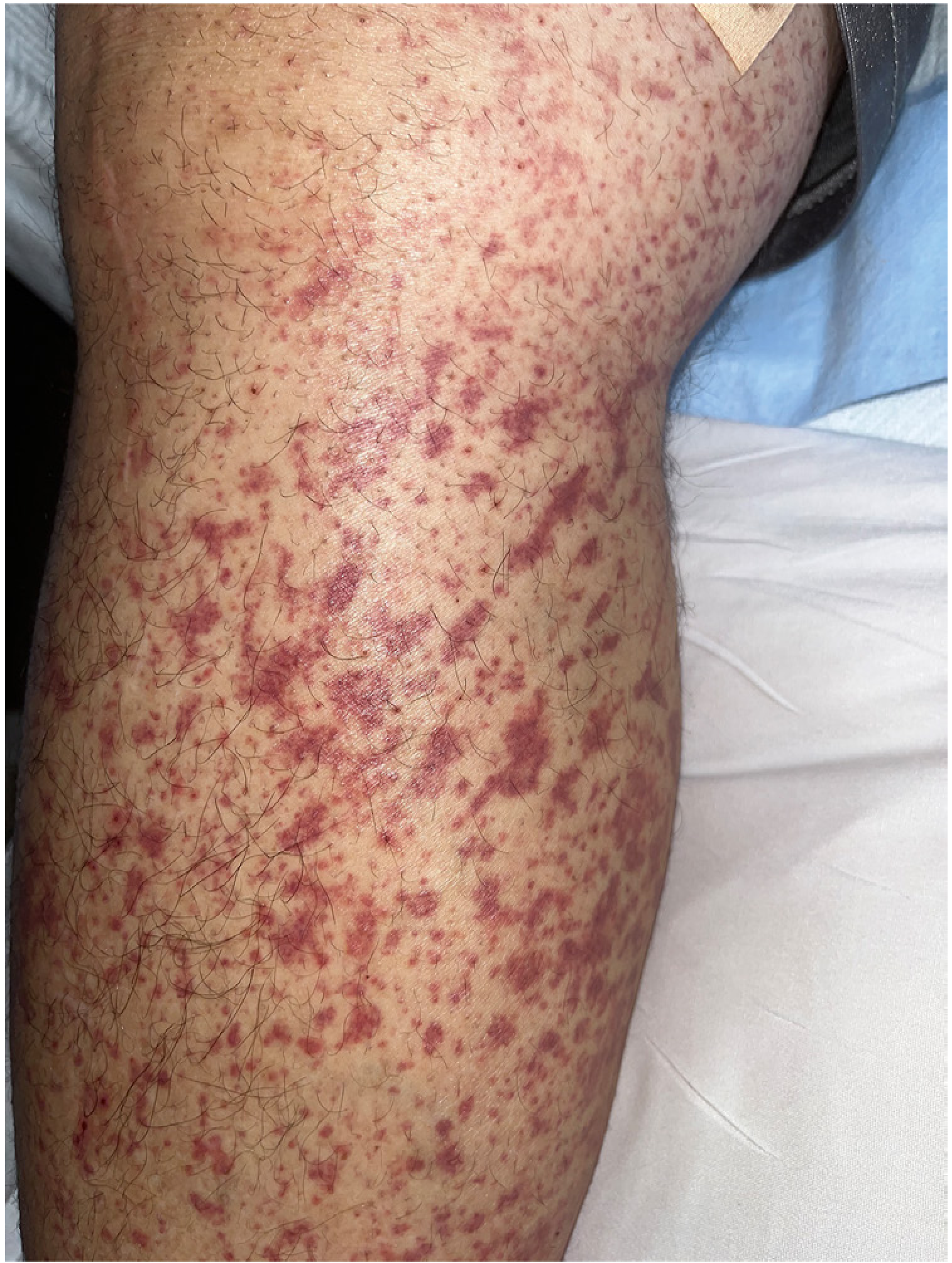
Palpable purpura in IgA vasculitis (Firestein & Kelley's Rheumatology)

HSP purpura on buttock/shoulder in a child (Andrews' Diseases of the Skin)
2. GI Tract (25-90% of patients)
- Colicky abdominal pain - most common; occurs within a week of rash onset
- GI bleeding: melena, hematochezia, hematemesis (~18% of patients)
- Nausea, vomiting, distension, rebound tenderness
- Endoscopy shows purpuric lesions in the upper or lower intestinal tract
- GI radiographs: "spiking" or "cobblestone" mucosal appearance
- Critical point: GI symptoms can precede the rash by days to weeks - creating a diagnostic dilemma mimicking acute surgical abdomen and occasionally leading to unnecessary exploratory surgery
- Complications: paralytic ileus, intussusception (rare), perforation (rare)
3. Joints (63% of patients)
- Periarticular swelling around knees and ankles predominantly; also elbows, wrists
- Ranges from arthralgias to frank arthritis with effusions
- No joint deformity or erosive arthritis (distinguishes from rheumatoid arthritis)
4. Kidneys (20-60% of patients)
- Usually occurs within days to weeks after systemic manifestations (mean 14 days)
- Presentations:
- Microscopic hematuria (most common)
- Gross hematuria
- Proteinuria (may reach nephrotic range)
- Nephritic syndrome (hypertension, oliguria, edema)
- Rarely: rapidly progressive GN with crescents
- Renal disease is more severe in older children and adults
- Renal biopsy findings are identical to IgA nephropathy (mesangial IgA deposits)
Laboratory Findings
| Test | Finding |
|---|---|
| Platelet count | Normal (distinguishes from thrombocytopenic purpura) |
| Serum complement (C3, C4) | Normal |
| ANA, ANCA | Negative |
| Serum IgA | Elevated in up to 50% during active disease |
| Ga-deficient IgA1 | Elevated |
| Urinalysis | Hematuria, proteinuria (if renal involved) |
| Renal function | Usually normal; may be impaired in severe nephritis |
| Stool occult blood | Positive if GI bleeding |
| Throat culture / ASO titer | To identify streptococcal trigger |
Diagnosis
1990 ACR Classification Criteria (Table 92.4):
- Age at onset ≤ 20 years
- Palpable purpura
- Acute abdominal pain
- Biopsy showing granulocytes in arteriolar/venular walls
Histopathology (biopsy of skin or kidney):
- Skin: Leukocytoclastic angiitis with IgA, IgG, C3 deposition on direct immunofluorescence (DIF)
- Kidney: Mesangial proliferative GN with dominant mesangial IgA deposits on immunofluorescence
- DIF showing florid IgA deposition is diagnostic in the proper clinical setting
"Histamine trap test": In patients with abdominal pain but no skin lesions yet - intradermal histamine injection followed by 4-hour biopsy to identify IgA in vessel walls.
Differential Diagnosis
- Meningococcemia (purpura + fever + septic appearance)
- Thrombocytopenic purpura (platelet count will be low)
- SLE (ANA positive, complement low)
- Microscopic polyangiitis (ANCA positive)
- Cryoglobulinemic vasculitis
- Acute appendicitis / surgical abdomen (when GI symptoms precede rash)
- IgA nephropathy (renal-limited form; no systemic features)
Treatment
| Severity | Management |
|---|---|
| Mild (skin only) | Supportive care; no specific therapy needed |
| Abdominal pain | H2 blockers + prednisone 1 mg/kg/day (more effective than analgesia alone) |
| Skin lesions only, requiring treatment | Dapsone 50-200 mg/day OR colchicine 0.6-1.2 mg/day |
| Renal disease (mild-moderate) | Monitor; controversial role for steroids |
| Severe renal / crescentic GN | High-dose glucocorticoids + mycophenolate mofetil (steroid-sparing); cyclophosphamide also used |
| Refractory disease / rapidly progressive GN | IVIG |
| Variceal/major GI bleeding | As per GI bleeding protocol |
- NSAIDs should be avoided - risk of renal and GI complications
- Octreotide for variceal bleeding if endoscopy unavailable
Prognosis
- Self-limited in most children - usual illness duration 6-16 weeks
- Recurrences are common (5-30%), often over months with crops of purpura
- Virtually all children recover completely
- Less than 5% develop renal failure
- Adults have a worse prognosis - higher rates of renal insufficiency (32% of adults have renal insufficiency at presentation) and prolonged disease
- Risk factors for poor renal outcome: nephrotic-range proteinuria (>1 g/day), baseline renal impairment, crescents on biopsy, hypertension
- Follow-up: serial urinalysis and blood pressure monitoring for at least 6 months after diagnosis
Sources: Firestein & Kelley's Textbook of Rheumatology; Brenner & Rector's The Kidney; Andrews' Diseases of the Skin; Goldman-Cecil Medicine
A 14 years girl with abdominal pain and blood in vomit for 1 day the differential diagnosis is with reason
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive textbook data. Let me deliver the full answer with reasoning for each differential.
Differential Diagnosis: 14-Year-Old Girl with Abdominal Pain + Hematemesis (with Reasoning)
Key clinical facts to hold in mind:
- Age: 14 years (adolescent) - adult-pattern diseases become relevant
- Sex: Female - consider pregnancy-related causes (ectopic rupture can cause abdominal pain; Mallory-Weiss from hyperemesis)
- Symptom duration: 1 day (acute)
- Two cardinal symptoms: abdominal pain + blood in vomit (hematemesis)
The combination of hematemesis + abdominal pain localizes the source to the upper GI tract (above the ligament of Treitz) and significantly narrows the differential compared to painless bleeding.
COMMON CAUSES
1. Gastritis / H. pylori-Associated Gastritis
Reason: H. pylori is the single most common cause of secondary gastritis and peptic disease in older children and adolescents. The organism colonizes the gastric antrum, triggers a neutrophilic-then-lymphocytic mucosal inflammatory infiltrate (gastritis), disrupts the protective mucus layer, and causes diffuse mucosal erosion - which bleeds. Epigastric burning pain is the hallmark. In a 14-year-old, this pattern closely resembles adult peptic disease.
Supporting features: Epigastric pain, burning or gnawing quality, nausea, anorexia. History of NSAID use amplifies risk. Diagnosis by endoscopy with biopsy + CLO test or urea breath test.
2. Peptic Ulcer Disease (PUD)
Reason: By adolescence, peptic ulcers present in a pattern nearly identical to adults - epigastric pain, classically relieved by food (duodenal ulcer) or worsened by food (gastric ulcer). The pain is due to acid acting on a denuded mucosal surface where the mucus barrier has been breached (either by H. pylori or NSAIDs). When the ulcer erodes into a submucosal vessel (most commonly the gastroduodenal artery in a posterior duodenal ulcer), it produces hemorrhage and hematemesis. Abdominal pain precedes or accompanies bleeding.
Supporting features: Family history of PUD, NSAID/aspirin use, positive H. pylori serology. Coffee-ground or bright red vomit depending on volume/acuity.
3. Mallory-Weiss Tear
Reason: A longitudinal mucosal laceration at or just below the gastroesophageal junction, caused by a sudden rise in intragastric pressure during forceful retching or vomiting. The mechanism: forceful vomiting raises intragastric pressure against a closed glottis, generating a pressure gradient that tears the relatively inelastic mucosa at the cardia. This is very common in adolescents after episodes of forceful vomiting - including from alcohol ingestion, food poisoning, or bulimia. The blood appears bright red and typically follows several episodes of non-bloody vomiting.
Supporting features: History of repeated retching before the blood appeared; epigastric or chest discomfort. Ask about alcohol use, eating disorders, or recent viral illness with vomiting.
4. Reflux Esophagitis / GERD
Reason: Acid reflux causes inflammatory damage to the esophageal squamous epithelium. In severe esophagitis, the mucosa becomes eroded and ulcerated (erosive esophagitis), producing bleeding mixed with vomit. Associated epigastric and substernal burning pain. Adolescents with obesity or dietary habits promoting reflux are at risk.
Supporting features: Heartburn, dysphagia, waterbrash, worse after meals or lying down. Diagnosis by endoscopy.
LESS COMMON BUT IMPORTANT CAUSES
5. Esophageal / Gastric Varices
Reason: Portal hypertension (from liver disease - cirrhosis, biliary atresia, extrahepatic portal vein obstruction) causes back-pressure in the portal system, diverting blood through portosystemic collaterals including the submucosal veins of the lower esophagus and gastric fundus. These veins dilate into varices - thin-walled, poorly supported vessels that can rupture suddenly, causing massive, life-threatening hematemesis. Even in children, conditions like portal vein thrombosis, Wilson's disease, or autoimmune hepatitis can cause varices.
Supporting features: History of liver disease, jaundice, splenomegaly on examination, spider angiomata, caput medusae, ascites. Often painless massive bleeding but can have abdominal discomfort from distension. Elevated serum bilirubin, AST/ALT, low albumin, prolonged PT.
6. Coagulopathy / Bleeding Diathesis
Reason: In the absence of a structural GI lesion, a systemic defect in hemostasis can cause bleeding from any mucosal surface, including the stomach. Causes include von Willebrand disease (most common inherited bleeding disorder), thrombocytopenia (ITP, leukemia, aplastic anemia), liver failure (reduced clotting factor synthesis), or drug-induced coagulopathy (warfarin, rodenticide poisoning). The stomach and esophagus are lined with a fragile mucosa; even normal-pressure contact vessels will bleed if coagulation is inadequate.
Supporting features: Easy bruising elsewhere, prolonged bleeding from cuts, gum bleeding, heavy menstrual periods, family history of bleeding disorder, medications. Labs: low platelets, prolonged PT/APTT, low fibrinogen.
7. Henoch-Schonlein Purpura (IgA Vasculitis)
Reason: HSP causes IgA immune complex deposition in small vessel walls throughout the body, including the GI tract submucosa. This triggers leukocytoclastic vasculitis of the intestinal microvasculature, producing mucosal ischemia, ulceration, and hemorrhage. Colicky abdominal pain and GI bleeding are present in up to 65% of patients. Critically - GI symptoms (including hematemesis and abdominal pain) can precede the characteristic skin purpura by days to weeks, making early diagnosis very difficult and sometimes mimicking a surgical abdomen.
Supporting features: Ask about recent URTI, joint pains, and rash on legs/buttocks. Look for palpable purpura, periarticular swelling around knees/ankles, hematuria. Serum IgA elevated in 50%. Diagnosis confirmed by skin/renal biopsy showing IgA deposits.
8. Inflammatory Bowel Disease (Crohn's Disease)
Reason: Crohn's disease can involve any part of the GI tract from mouth to anus, including the stomach and duodenum (upper GI Crohn's). Transmural inflammation causes ulceration, which bleeds. Upper GI involvement in Crohn's is more common in children than adults. Additionally, systemic inflammation and weight loss are hallmarks. IBD presenting with hematemesis in an adolescent is a red flag for extensive disease.
Supporting features: Chronic or recurrent abdominal pain, diarrhea, weight loss, mouth ulcers, perianal disease, delayed puberty, elevated CRP/ESR, low albumin, positive fecal calprotectin. Family history of IBD.
9. Toxic / Caustic Ingestion or Drug-Induced Mucosal Injury
Reason: Ingestion of NSAIDs, aspirin, iron tablets, corticosteroids, or alcohol directly damages the gastric mucosa by inhibiting prostaglandin synthesis (NSAIDs/aspirin), generating free radicals (iron), or direct contact toxicity (alcohol). Caustic ingestion (acid or alkali) causes severe mucosal necrosis with immediate hematemesis and severe pain. In a 14-year-old, both accidental and intentional ingestions must be considered.
Supporting features: Medication history (NSAIDs for dysmenorrhea are very common in adolescent girls), alcohol use history, mental health assessment (self-harm/suicide attempt), iron supplementation.
10. Intestinal Obstruction / Ischemia
Reason: Any cause of bowel obstruction (malrotation with volvulus, adhesions from prior surgery, internal hernia) can cause ischemia of the bowel wall. Ischemic mucosa becomes friable and hemorrhagic, producing bloody vomit along with severe colicky abdominal pain. Volvulus is a surgical emergency.
Supporting features: Bilious (green) vomiting, absent bowel sounds, abdominal distension, peritoneal signs, prior abdominal surgery. Urgent imaging (X-ray, CT, upper GI contrast study).
11. Pregnancy-Related (Ectopic Pregnancy / Hyperemesis)
Reason: In a 14-year-old sexually active female, ectopic pregnancy must not be missed. A ruptured ectopic causes peritoneal irritation and severe abdominal pain. Hyperemesis (severe vomiting of pregnancy) can cause a Mallory-Weiss tear. Always check a urine/serum βhCG in any adolescent girl presenting with acute abdominal pain.
Supporting features: Last menstrual period, sexual activity history, βhCG (mandatory), pelvic pain, shoulder tip pain (diaphragmatic irritation from haemoperitoneum in ruptured ectopic).
12. Dieulafoy's Lesion / Vascular Malformation
Reason: A Dieulafoy's lesion is an aberrant, large-caliber submucosal artery (most often in the gastric fundus) that erodes through an otherwise intact mucosa and bleeds massively. It accounts for 1-2% of GI bleeds but can present dramatically with sudden, massive hematemesis and minimal or no abdominal pain. Vascular malformations (angiodysplasia, arteriovenous malformations) are another rare structural cause.
Supporting features: Sudden massive hematemesis with no prior symptoms, no NSAID use, no H. pylori. Diagnosis only by endoscopy.
Summary Table with Reasoning
| Diagnosis | Why it Causes Abdominal Pain | Why it Causes Hematemesis | Key Distinguishing Feature |
|---|---|---|---|
| H. pylori Gastritis | Mucosal inflammation, acid on inflamed antrum | Mucosal erosion bleeds | Most common cause; epigastric burning |
| Peptic Ulcer Disease | Acid on exposed submucosa | Erosion into submucosal vessel | Rhythmic epigastric pain; NSAID/H. pylori history |
| Mallory-Weiss Tear | Epigastric/chest pain from laceration | Tear of cardia mucosa after retching | Blood only AFTER repeated vomiting |
| Esophagitis (GERD) | Acid injury to esophagus | Erosive mucosal bleeding | Heartburn, dysphagia |
| Esophageal Varices | Distension, portal hypertension | Variceal rupture | Liver disease signs, massive bleed |
| Coagulopathy | Mucosal oozing from any site | Failure of hemostasis | Easy bruising, abnormal PT/APTT/platelets |
| HSP (IgA Vasculitis) | GI vasculitis causing ischemia/ulceration | GI mucosal hemorrhage | Purpura + arthralgia; GI can precede rash |
| Crohn's Disease | Transmural GI inflammation | Upper GI ulceration | Chronic symptoms, weight loss, perianal disease |
| Drug/Toxic Ingestion | Direct mucosal injury | Mucosal necrosis | Medication or ingestion history |
| Bowel Obstruction/Ischemia | Obstruction and ischemia | Ischemic mucosa hemorrhage | Bilious vomiting, distension |
| Ectopic Pregnancy | Peritoneal irritation | Mallory-Weiss from vomiting | βhCG positive |
| Dieulafoy's / AVM | Minimal pain | Aberrant artery rupture | Sudden massive painless bleed |
First investigations in the ED:
CBC, PT/INR/APTT, LFTs, BUN/creatinine (elevated BUN:creatinine ratio >30 suggests UGIB), serum lipase, urine βhCG, blood group & crossmatch, urinalysis (hematuria for HSP), and urgent upper GI endoscopy once stabilized.
Sources: Tintinalli's Emergency Medicine (Table 134-1 & 134-3); Firestein & Kelley's Rheumatology; Brenner & Rector's The Kidney
Write a provisional and some differential diagnosis of a pediatric male of 6 years with chief complaints of abnormal body movement with stiffness and clonus, loss of consciousness, up rolling of eyes and drooling of saliva form the mouth without any fecal and urinary continence and each seizure episode lasting about a minute
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have rich textbook content to build a thorough, well-reasoned answer. Let me compose it.
Provisional & Differential Diagnoses
6-Year-Old Male | Abnormal Body Movements with Stiffness, Clonus, Loss of Consciousness, Uprolling of Eyes, Drooling of Saliva, No Incontinence | ~1 Minute Duration
Clinical Analysis of the Presentation
First, let's decode what is being described symptom by symptom:
| Symptom | Clinical Interpretation |
|---|---|
| Abnormal body movements with stiffness | Tonic phase - sustained rigid muscle contraction |
| Clonus | Clonic phase - rhythmic repetitive jerking contractions |
| Loss of consciousness | Cortical involvement is bilateral and generalized |
| Uprolling of eyes | Oculogyric deviation - tonic deviation of globes upward as extraocular muscles seize |
| Drooling of saliva | Autonomic excess + inability to swallow during unconsciousness |
| No fecal/urinary incontinence | Bladder and bowel sparing - less severe tonic involvement; or early/brief event |
| Duration ~1 minute | Self-limited; consistent with typical seizure duration (not status epilepticus) |
This is a classic Generalized Tonic-Clonic (GTC) seizure - the sequence of stiffness (tonic) → rhythmic jerking (clonic) → loss of consciousness + uprolling eyes + hypersalivation is the textbook description.
"The initial motor signs are typically a brief flexion of the trunk, an opening of the mouth and eyelids, and upward deviation of the eyes... followed by a more protracted extension (tonic) phase... There then occurs a transition from the tonic to the clonic phase... Autonomic signs are prominent: the pulse is rapid, blood pressure is elevated, pupils are dilated, and salivation and sweating are prominent."
- Adams & Victor's Principles of Neurology, 12th Ed.
PROVISIONAL DIAGNOSIS
Generalized Tonic-Clonic (GTC) Seizure - First Episode / Idiopathic Generalized Epilepsy (IGE)
Reason: The clinical triad of:
- Tonic rigidity (stiffness) → clonic jerking (clonus) - the hallmark sequence
- Loss of consciousness from onset (generalized, not focal onset)
- Autonomic features - uprolling eyes, hypersalivation
- Self-limited (~1 minute) with no post-ictal focal deficit described
...in a 6-year-old boy is most consistent with a primary generalized tonic-clonic seizure, either as:
- A first unprovoked seizure (awaiting investigation to classify)
- Or an established epilepsy syndrome such as Childhood Epilepsy with Centrotemporal Spikes (BECTS/Benign Rolandic Epilepsy) - the most common childhood epilepsy, onset typically 3-13 years
The absence of fecal/urinary incontinence in a GTC is notable but does not exclude the diagnosis - incontinence occurs in roughly 50-60% of GTC seizures and its absence does not rule out a seizure.
DIFFERENTIAL DIAGNOSES (with Reasoning)
1. Benign Childhood Epilepsy with Centrotemporal Spikes (BECTS / Benign Rolandic Epilepsy)
Reason: This is the most common focal epilepsy syndrome of childhood, representing 10-20% of all childhood epilepsies, with peak onset at 5-10 years. It is caused by focal discharges in the rolandic (centrotemporal) cortex which can secondarily generalize, producing a GTC seizure indistinguishable from a primary generalized one. The EEG shows characteristic centrotemporal spike-wave discharges, increased during sleep. Seizures often occur at night or on awakening. The condition is self-limited, resolving by mid-adolescence, and is pharmacoresponsive if treatment is needed at all.
Key distinguishing features: Focal onset signs (orofacial twitching, tongue numbness, hypersalivation) preceding generalization; nocturnal predominance; normal neurodevelopment; characteristic EEG.
2. Febrile Seizure (with Fever Not Mentioned - Must Exclude)
Reason: Febrile seizures are the most common seizure type in children aged 6 months to 6 years (peak 14-18 months, but can occur up to 6 years). A high fever lowers the seizure threshold in genetically predisposed children - the mechanism involves fever-induced neuronal hyperexcitability, particularly in the immature brain. The seizure itself is indistinguishable in semiology from an idiopathic GTC. This diagnosis requires a measured or reported fever - if the child had a concurrent febrile illness, this becomes the primary consideration.
Key distinguishing features: Presence of fever >38°C, age 6 months-6 years, no prior afebrile seizures, no CNS infection. Simple febrile seizure: <15 minutes, generalized, single episode in 24 hours.
3. Symptomatic / Structural Epilepsy (Secondary Generalized Seizure)
Reason: Any structural brain lesion (cortical dysplasia, perinatal hypoxic-ischemic injury, post-traumatic scar, low-grade tumor, cavernous malformation) can be epileptogenic by generating abnormal focal discharges that secondarily generalize. The immature brain is particularly susceptible to epileptogenesis from acquired structural lesions. In a 6-year-old with a first GTC, a focal-to-bilateral tonic-clonic seizure must be distinguished from primary generalized onset, as the former implies an underlying structural cause requiring imaging.
Key distinguishing features: History of birth trauma, neonatal hypoxia, head injury, developmental regression, focal neurological deficits on examination, asymmetric seizure features (head/eye turning to one side, unilateral clonic activity), focal EEG abnormality, abnormal MRI.
4. Viral Meningo-Encephalitis
Reason: Inflammation of the brain parenchyma (encephalitis) from viral pathogens (HSV, enterovirus, EBV, influenza) directly irritates cortical neurons, lowering the seizure threshold and triggering seizures. In children, viral encephalitis typically presents with fever, altered sensorium, and new-onset seizures. This is a medical emergency - HSV encephalitis in particular carries high mortality if untreated.
Key distinguishing features: Fever, headache, neck stiffness (meningism), altered consciousness between seizure episodes (not just postictal confusion), CSF pleocytosis, elevated CSF protein, abnormal MRI (temporal lobe involvement in HSV). Must be actively excluded in any child with a first seizure and altered consciousness.
5. Bacterial Meningitis
Reason: Bacterial infection of the meninges causes cerebral edema, cortical irritation, and electrolyte disturbances (SIADH with hyponatremia), all of which promote seizures. Seizures in bacterial meningitis are a sign of serious intracranial inflammation and carry a worse prognosis.
Key distinguishing features: Fever (often high), severe headache, photophobia, phonophobia, neck stiffness (Kernig's and Brudzinski's signs), petechial/purpuric rash (Neisseria meningitidis), toxic appearance. Lumbar puncture is diagnostic (turbid CSF, high neutrophils, high protein, low glucose).
6. Metabolic / Electrolyte-Induced Seizures
Reason: The brain requires a tightly regulated ionic environment to maintain the resting membrane potential and action potential threshold. Disruptions in serum sodium (hyponatremia - most common), calcium (hypocalcemia), magnesium (hypomagnesemia), glucose (hypoglycemia), or phosphate cause neuronal membrane instability and spontaneous firing. Hypoglycemia in particular (from insulin excess, fasting, inborn errors of metabolism) is a common and reversible cause of childhood seizures.
Key distinguishing features: No postictal state with hypoglycemia (seizure stops quickly with glucose correction), tetanic signs with hypocalcemia (Chvostek's, Trousseau's signs), history of metabolic disease or diabetes. Serum glucose, electrolytes, calcium, magnesium must be checked in every child with a first seizure.
7. Childhood Absence Epilepsy (Atypical / with GTC)
Reason: Childhood absence epilepsy (CAE) typically presents with brief (5-30 second) staring spells in children aged 4-10 years. However, GTC seizures can occur in CAE (approximately 30-40% of patients with CAE eventually develop GTC seizures). CAE is caused by generalized 3-Hz spike-and-wave discharges from thalamocortical circuits. If absence seizures were not noticed previously (brief, may be mistaken for daydreaming), the GTC may be the presenting event.
Key distinguishing features: History of brief staring spells, automatic eye blinking, brief lapses of awareness in school; generalized 3-4 Hz spike-and-wave on EEG precipitated by hyperventilation.
8. Lennox-Gastaut Syndrome (LGS)
Reason: LGS is a severe childhood epileptic encephalopathy characterized by multiple seizure types (tonic, atonic, atypical absence, GTC), cognitive impairment, and a characteristic EEG pattern of slow spike-and-wave (<2.5 Hz). Onset is typically 1-7 years. A 6-year-old presenting with a first apparent GTC may in fact have LGS if there is history of other seizure types (drop attacks, staring spells) or developmental regression.
Key distinguishing features: Multiple seizure types, cognitive/developmental impairment, slow spike-wave on EEG, history of prior epileptic encephalopathy (West syndrome).
9. Intracranial Space-Occupying Lesion (Brain Tumor / Abscess)
Reason: A tumor (astrocytoma, PNET, ependymoma) or brain abscess in the motor cortex or its projection pathways can generate seizures by direct cortical irritation. In children, brain tumors are the second most common solid tumor. New-onset seizures in a child, especially if accompanied by headache (worse in morning), vomiting, papilledema, or personality change, mandate urgent neuroimaging.
Key distinguishing features: Subacute headache (worse on waking, with Valsalva), vomiting, papilledema, focal neurological deficit, personality change. MRI with contrast is diagnostic.
10. Neurocysticercosis (Endemic regions)
Reason: In endemic areas (parts of Asia, Africa, Latin America), Taenia solium larval cysts (cysticerci) lodge in the brain parenchyma and cause cortical irritation when the cyst degenerates, triggering seizures. It is the most common cause of secondary epilepsy worldwide and a major cause of new-onset seizures in children in endemic regions.
Key distinguishing features: Relevant geographical/travel/exposure history, calcified lesions or ring-enhancing lesions on CT/MRI, positive serology (ELISA), eosinophilia.
Summary Table
| Diagnosis | Provisional/Differential | Key Reason |
|---|---|---|
| Idiopathic GTC Seizure / IGE | Provisional | Classic tonic-clonic sequence, LOC, autonomic features, self-limited |
| Benign Rolandic Epilepsy (BECTS) | Differential 1 | Most common childhood focal epilepsy, age 5-10, secondarily generalized |
| Febrile Seizure | Differential 2 | Most common at this age; requires fever to be present |
| Structural/Symptomatic Epilepsy | Differential 3 | Focal lesion causing secondary generalization; needs MRI |
| Viral Encephalitis (HSV etc.) | Differential 4 | Cortical irritation from inflammation; emergency |
| Bacterial Meningitis | Differential 5 | Cortical irritation + SIADH; signs of meningism |
| Metabolic/Electrolyte Imbalance | Differential 6 | Disrupted ionic homeostasis; reversible |
| Childhood Absence Epilepsy + GTC | Differential 7 | GTC can coexist in CAE; history of staring spells |
| Lennox-Gastaut Syndrome | Differential 8 | Multiple seizure types, cognitive impairment |
| Brain Tumor / Abscess | Differential 9 | Space-occupying lesion irritating cortex |
| Neurocysticercosis | Differential 10 | Most common cause of epilepsy worldwide in endemic areas |
Recommended Immediate Investigations
- Blood glucose (bedside, immediate) - exclude hypoglycemia
- Serum electrolytes - Na, K, Ca, Mg, phosphate
- CBC + CRP - infection screen
- Lumbar puncture - if fever, meningism, or altered consciousness persists (after imaging if raised ICP suspected)
- EEG - characterize seizure type and epilepsy syndrome
- MRI brain - exclude structural, infectious, and malignant causes
- βhCG - not applicable here (male patient)
Sources: Adams & Victor's Principles of Neurology, 12th Ed.; Bradley & Daroff's Neurology in Clinical Practice; Rosen's Emergency Medicine; Harriet Lane Handbook 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.