Images of ecgs explanations management of most common and important ICU cases
ECG ventricular fibrillation VF ICU
ECG STEMI ST elevation myocardial infarction 12 lead
ECG hyperkalemia peaked T waves widened QRS
ECG ventricular tachycardia VT wide complex
ECG complete heart block third degree AV block
ECG atrial fibrillation irregular rhythm absent P waves
ECG pulmonary embolism S1Q3T3 right heart strain
ECG Torsades de Pointes long QT twisting polymorphic VT
ECG pericarditis diffuse ST elevation saddle shape PR depression
- VF → unsynchronized shock; VT (unstable) → synchronized cardioversion; TdP → MgSO₄ first
- Hyperkalemia has a predictable ECG progression — calcium gluconate stabilizes the membrane before shifting K⁺
- Tamponade produces electrical alternans — the alternating QRS is almost pathognomonic
- STEMI vs. Pericarditis: reciprocal changes favor STEMI; PR depression + saddle morphology favor pericarditis
- VT vs. SVT with aberrancy: AV dissociation, capture/fusion beats, and concordance all point to VT
More
ECG inferior STEMI ST elevation leads II III aVF right ventricular infarction
ECG Wolff-Parkinson-White WPW delta wave pre-excitation
ECG hypokalemia U wave flattened T wave
ECG cardiac tamponade electrical alternans low voltage
ECG digoxin toxicity sagging ST depression reverse tick sign
ECG hypothermia Osborn J wave bradycardia
ECG SVT supraventricular tachycardia narrow complex AVNRT
ECG left bundle branch block LBBB new wide QRS
ECG Brugada syndrome type 1 coved ST elevation V1 V2 right precordial
ECG de Winter T waves LAD occlusion STEMI equivalent
More Critical ICU ECG Cases — Part 2
10. Inferior STEMI + Right Ventricular (RV) Infarction
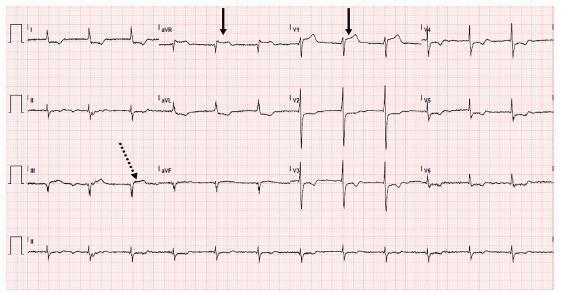
ECG Features
- ST elevation in II, III, aVF — inferior territory
- ST III > ST II = strongly suggests RCA (right coronary artery) occlusion over LCx
- Reciprocal ST depression in I and aVL — essential to recognize
- ST elevation in V1 and aVR — flags proximal RCA occlusion with RV involvement
- Confirm RV infarct: Apply right-sided leads → ST elevation ≥1 mm in V3R–V4R is diagnostic
- AV block is a frequent complication (AV node is supplied by RCA in 85% of people)
Why RV Infarction Changes Management Critically
| Feature | Implication |
|---|---|
| RV infarct = preload-dependent | NEVER give nitrates or diuretics — precipitates catastrophic hypotension |
| Hypotension after inferior MI | Give IV fluid bolus (500 mL NS) first |
| Bradycardia/AV block | Atropine; temporary pacemaker if needed |
| Reperfusion | Primary PCI urgently (same as anterior STEMI) |
Classic triad of RV infarction: Hypotension + Elevated JVP + Clear lung fields (no pulmonary edema)
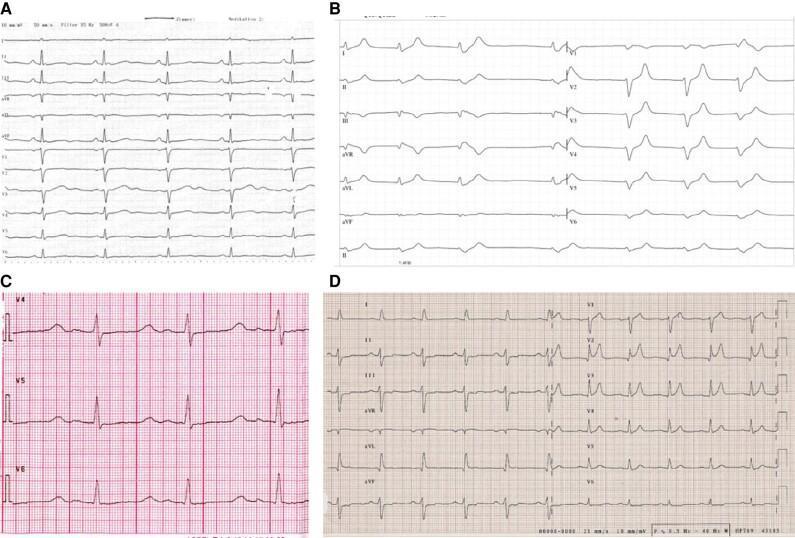
11. Cardiac Tamponade — Electrical Alternans
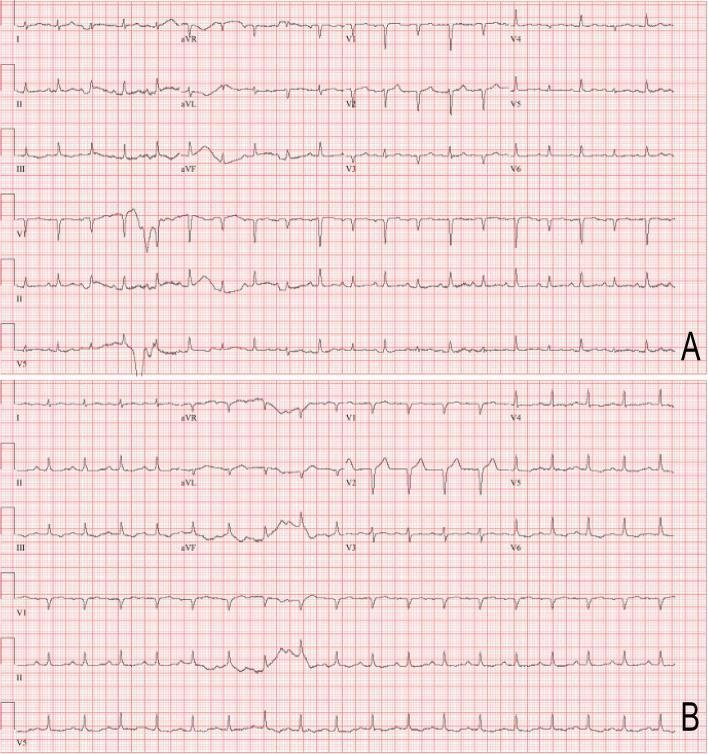
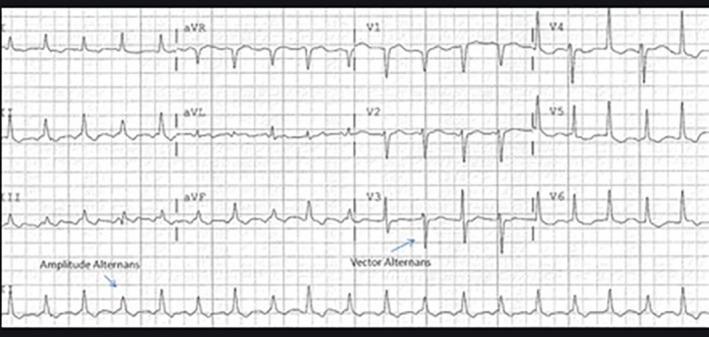
ECG Features
- Sinus tachycardia — compensatory
- Low voltage — QRS <5 mm in all limb leads AND <10 mm in all precordial leads
- Electrical alternans — beat-to-beat variation in QRS axis/amplitude (heart "swinging" in pericardial fluid)
- Total electrical alternans (P + QRS + T alternating) = pathognomonic for large effusion with tamponade
Beck's Triad (clinical diagnosis)
- Hypotension + Raised JVP + Muffled heart sounds
- Pulsus paradoxus >10 mmHg drop in SBP on inspiration
Management
| Step | Action |
|---|---|
| 1 | IV fluid bolus (500–1000 mL) — maintain preload while preparing |
| 2 | Avoid positive pressure ventilation / PEEP if possible |
| 3 | Emergency pericardiocentesis — echo-guided; subxiphoid approach |
| 4 | Send fluid for cytology, culture, protein, LDH (Light's criteria if exudate) |
| 5 | Pericardial window (surgical) for recurrent/malignant effusions |
In the ICU, tamponade is commonly caused by: post-cardiac surgery, aortic dissection, malignancy, uremia, or post-MI (Dressler syndrome)
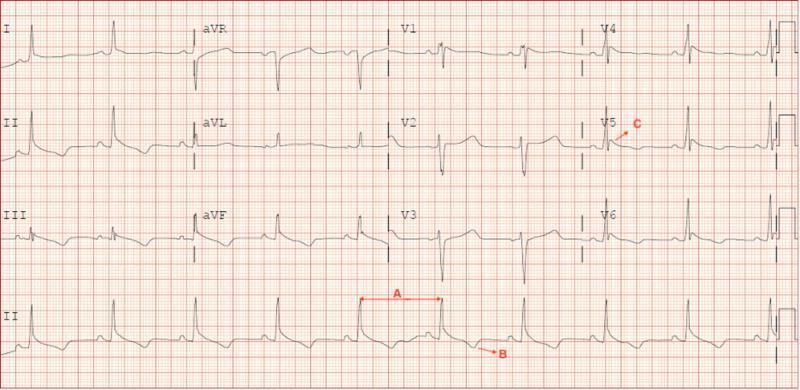
12. SVT — Narrow Complex Tachycardia (AVNRT/AVRT)
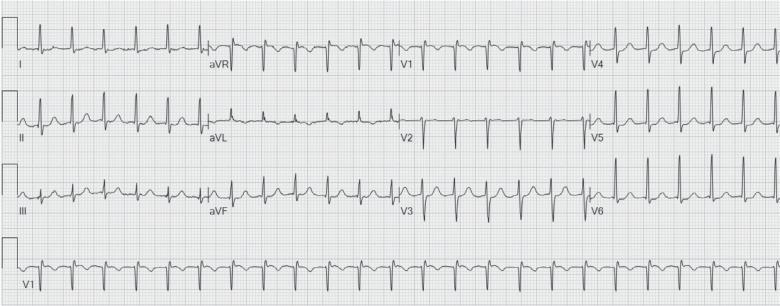
ECG Features
- Regular, narrow QRS tachycardia (QRS <120 ms) at rate 150–280 bpm
- P waves absent, buried in QRS (AVNRT — "short RP"), or just after QRS as pseudo-S or pseudo-R' in V1
- Perfectly regular R-R intervals (distinguish from AF which is irregular)
- Rate ~150 bpm → always check for atrial flutter with 2:1 block (look for flutter waves in V1, II)
- Rate >200 bpm + wide QRS → consider WPW (antidromic AVRT — treat differently!)
Management
| Step | Intervention |
|---|---|
| 1st | Vagal maneuvers — Valsalva (modified: legs up), carotid sinus massage |
| 2nd | Adenosine 6 mg rapid IV push + flush; if no response → 12 mg × 2 |
| Unstable | Synchronized cardioversion 50–100J |
| Recurrent | Metoprolol or Verapamil IV for rate control; RF ablation for definitive cure |
Adenosine terminates re-entry through AV node (AVNRT/AVRT). It does NOT work for atrial flutter/VT — but can unmask flutter waves or reveal VT (AV dissociation). Do NOT give adenosine in WPW with AF (risk of degeneration to VF).
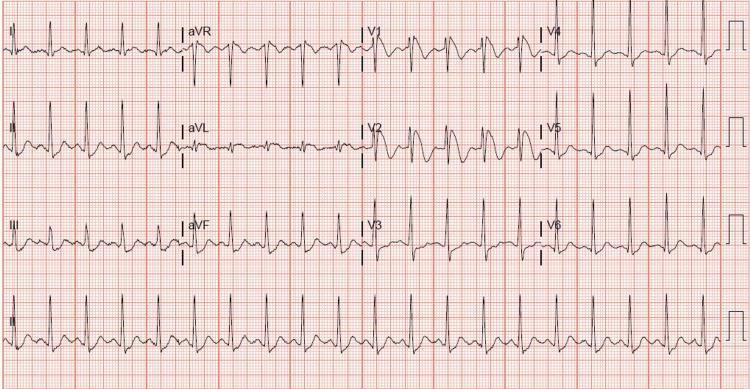
13. Wolff-Parkinson-White (WPW) Syndrome

ECG Features (Sinus Rhythm)
- Short PR interval (<120 ms) — bypass of AV node delay
- Delta wave — slurred, upsloping initial QRS deflection
- Wide QRS (>120 ms) — combined normal + accessory pathway conduction
- Discordant ST-T changes — secondary to abnormal depolarization
The ICU Emergency: WPW + Atrial Fibrillation
- If AF occurs in WPW, impulses conduct via accessory pathway at full rate (no AV node protection)
- Results in extremely rapid, irregular, wide-complex tachycardia (can approach 300 bpm)
- Can degenerate to VF and sudden cardiac death
- ECG shows: irregular, wide, bizarre-looking QRS at very rapid rate
Management
| Situation | Treatment |
|---|---|
| WPW + AF (unstable) | Unsynchronized DC cardioversion immediately |
| WPW + AF (stable) | Procainamide 15–17 mg/kg IV over 30–60 min (blocks accessory pathway) |
| WPW + AF — AVOID | Adenosine, Digoxin, Beta-blockers, Verapamil, Diltiazem (all block AV node → force all conduction through accessory pathway → VF) |
| Definitive | Radiofrequency catheter ablation |
14. Hypokalemia
ECG Features (K⁺ <3.5 mEq/L)
| K⁺ Level | ECG Change |
|---|---|
| 3.0–3.5 | Flattened T waves, mild ST depression |
| 2.5–3.0 | Prominent U waves (best seen V2–V4), T–U fusion |
| <2.5 | ST depression, markedly tall U waves, apparent "QU prolongation" |
| Severe | Ventricular ectopy, TdP, VF risk |
U wave = deflection after T wave, same polarity as T, best seen in V2–V4. When U > T amplitude = significant hypokalemia.
Management
- Oral KCl if mild and patient can take PO
- IV KCl (central line preferred for concentrated solutions):
- Rate: max 20 mEq/h via central line (10 mEq/h via peripheral)
- Monitor ECG continuously during infusion
- Replenish Magnesium simultaneously (hypoMg drives renal K⁺ wasting — refractory hypokalemia until Mg corrected)
- MgSO₄ 1–2 g IV over 15–30 min
- Identify cause: diuretics, vomiting, NGT losses, mineralocorticoid excess, RTA
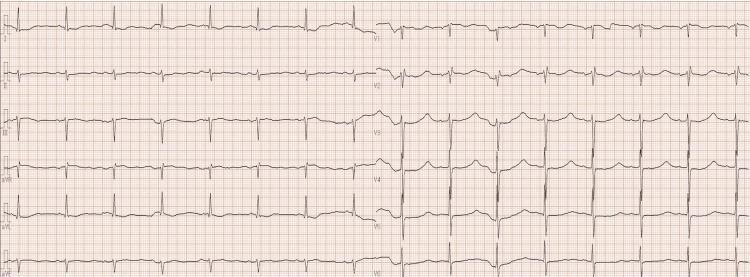
15. New Left Bundle Branch Block (LBBB) — STEMI Equivalent

ECG Features
- Wide QRS >120 ms
- Broad, notched "M-shaped" R waves in lateral leads (I, aVL, V5, V6)
- Deep QS pattern in right precordial leads (V1–V3)
- Discordant ST-T changes — ST and T wave go opposite to the main QRS deflection (NORMAL in LBBB)
Sgarbossa Criteria — Diagnosing MI in LBBB
| Criterion | Points | Sensitivity |
|---|---|---|
| Concordant ST elevation ≥1 mm in any lead (same direction as QRS) | 5 | High specificity |
| Concordant ST depression ≥1 mm in V1–V3 | 3 | Moderate |
| Discordant ST elevation ≥5 mm (>25% of S wave depth) | 2 | Less specific |
Modified Sgarbossa (Smith criteria): ST/S ratio < −0.25 in any lead (excessive discordant STE) is more sensitive and has largely replaced the original ≥5 mm criterion.
Management
- New LBBB + ischemic symptoms = treat as STEMI (activate cath lab, primary PCI)
- Pre-existing LBBB: apply Sgarbossa/modified Sgarbossa criteria
16. Hypothermia — Osborn (J) Waves
ECG Features (Progressive with Falling Temperature)
| Core Temp | ECG Finding |
|---|---|
| <35°C | Sinus bradycardia + prolonged PR/QT |
| <32°C | Osborn waves (J waves) — positive hump at J-point in inferior/lateral leads + QRS widening |
| <28°C | Atrial fibrillation (very common; often spontaneously reverts on rewarming) |
| <25°C | VF — most common cause of death in severe hypothermia |
Osborn wave amplitude correlates inversely with temperature — larger waves = colder patient
Management
| Severity | Core Temp | Rewarming Strategy |
|---|---|---|
| Mild | 32–35°C | Passive external (warm blankets, remove wet clothing) |
| Moderate | 28–32°C | Active external (forced warm air, heating pads to trunk) |
| Severe | <28°C | Active internal — warm IV fluids (42°C), warm humidified O₂, bladder/gastric lavage |
| Cardiac arrest | Any | ECMO (extracorporeal rewarming) — ideal for hypothermic arrest |
Golden rule: "Not dead until warm and dead" — CPR must continue until core temperature ≥32°C. VF in hypothermia is resistant to defibrillation until temperature >30°C.
17. Digoxin Toxicity
ECG Features
- Sagging/scooped "reverse tick" or "hockey stick" ST depression in V4–V6 and inferior leads
- Shortened QT interval
- T-wave flattening/inversion
- Prolonged PR interval (slows AV conduction)
- Bradyarrhythmias: Sinus bradycardia, all degrees of AV block, junctional escape rhythms
- Tachyarrhythmias: PAT (paroxysmal atrial tachycardia) with block is classic; accelerated junctional rhythm; bidirectional VT (pathognomonic — alternating QRS axis, seen with severe toxicity)
- "Regularization" of AF (junctional rhythm emerges) — sign of toxicity
Management
| Step | Action |
|---|---|
| 1 | Stop digoxin immediately |
| 2 | Correct electrolytes — hypokalemia and hypomagnesemia worsen toxicity |
| 3 | Bradycardia/heart block — Atropine 0.5–1 mg IV; temporary pacing if severe |
| 4 | Digoxin-specific Fab antibody fragments (Digibind/DigiFab) — definitive antidote |
| Dose: 10 vials empirically for life-threatening toxicity; or calculated by serum level | |
| 5 | Avoid calcium gluconate (may worsen cardiac toxicity — "stone heart") |
Digibind indication: VT/VF, complete heart block, K⁺ >5.5 mEq/L in acute toxicity, hemodynamic instability
18. Brugada Syndrome — Type 1 Pattern
ECG Features
- "Coved" ST elevation ≥2 mm in V1–V2 (or V1–V3 when leads placed in 2nd–3rd intercostal space)
- Convex downsloping ST segment → inverted T wave
- No ischemic symptoms needed for diagnosis
- Type 2 = "saddleback" pattern (≥2 mm STE with saddle shape) — not diagnostic alone, may unmask Type 1 with fever/sodium channel blockers
| Feature | Brugada Type 1 | Anterior STEMI |
|---|---|---|
| Lead distribution | Only V1–V2 (right precordial) | V2–V5 or more |
| ST morphology | Coved (convex down) | Convex up ("tombstone") |
| Reciprocal changes | Absent | Present (inferior leads) |
| Symptoms | Often syncope/nocturnal arrest | Chest pain |
ICU Significance
- Often presents as resuscitated VF/VT or unexplained syncope
- Triggers in ICU: Fever (unmasks pattern), hyponatremia, vagotonia, TCA overdose, cocaine, class Ic drugs
Management
- Acute VF/VT: Unsynchronized defibrillation + Isoproterenol infusion (increases HR, suppresses early repolarization)
- Quinidine — only oral drug shown to suppress VF in Brugada (blocks Ito channel)
- ICD — definitive therapy for symptomatic patients (aborted SCA, syncope with documented VT/VF)
- Avoid: Sodium channel blockers (flecainide, procainamide), beta-blockers, excess alcohol, treat fever aggressively
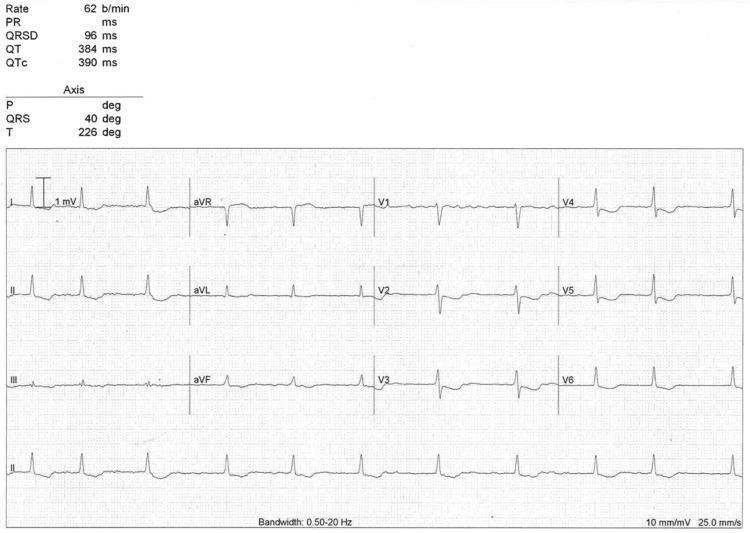
19. De Winter T-Waves — STEMI Equivalent (Proximal LAD)
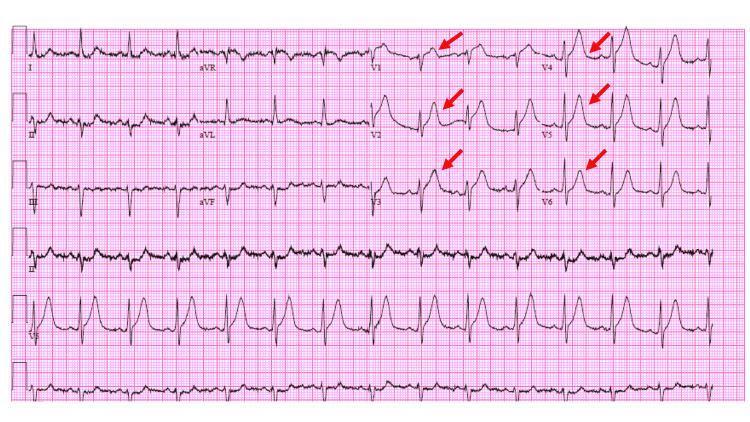
ECG Features
- J-point (ST) depression 1–3 mm at takeoff of QRS in V1–V6 (upsloping ST depression)
- Transitions into tall, symmetrical, hyperacute T waves in precordial leads
- Mild ST elevation in aVR (~0.5–1 mm)
- No classic ST elevation in anterior leads — does NOT meet STEMI criteria but IS a STEMI equivalent
- Represents ~2% of LAD occlusions — static pattern (doesn't evolve to STE)
Clinical Significance
- Indicates acute proximal LAD occlusion with extensive anterior wall ischemia
- Carry same urgency as anterior STEMI
- Commonly missed because no ST elevation — high-yield exam and clinical pearl
Management
- Activate cath lab immediately — treat as anterior STEMI
- Same antiplatelet, anticoagulation, and PCI protocol as STEMI
- Do NOT wait for troponin results
Expanded Quick Reference Table
| # | Condition | Pathognomonic ECG Sign | Do This First |
|---|---|---|---|
| 1 | VF | Chaotic no QRS | Shock 200J (unsynchronized) |
| 2 | Monomorphic VT | Wide QRS, AV dissociation | Cardioversion or Amiodarone |
| 3 | Torsades de Pointes | Twisting QRS, long QT | MgSO₄ 2g IV |
| 4 | Anterior STEMI | STE V1–V4, reciprocal depression | PCI <90 min |
| 5 | Inferior STEMI + RVI | STE II/III/aVF + V1/aVR | IV fluids, NO nitrates; urgent PCI |
| 6 | AF with RVR | Irregular, absent P waves | Rate control or cardioversion |
| 7 | 3° AV Block | AV dissociation, slow escape | Atropine + pacing |
| 8 | Hyperkalemia | Peaked T → sine wave | Calcium gluconate IV |
| 9 | Hypokalemia | U waves, flat T waves | KCl + Magnesium IV |
| 10 | Pulmonary Embolism | S1Q3T3, RV strain, tachycardia | UFH + consider tPA if massive |
| 11 | Cardiac Tamponade | Electrical alternans, low voltage | Pericardiocentesis |
| 12 | Pericarditis | Diffuse saddle STE + PR depression | NSAIDs + Colchicine |
| 13 | SVT (AVNRT) | Narrow regular tachycardia, no P | Adenosine 6 mg IV push |
| 14 | WPW + AF | Irregular very wide bizarre QRS | Cardioversion or Procainamide |
| 15 | New LBBB | Wide QRS, M-shaped R in lateral | Treat as STEMI (Sgarbossa) |
| 16 | Hypothermia | Osborn J waves + bradycardia | Active rewarming; ECMO if arrest |
| 17 | Digoxin Toxicity | Sagging ST + bradyarrhythmias | Digibind; correct K⁺/Mg²⁺ |
| 18 | Brugada | Coved STE V1–V2 | ICD; Isoproterenol for acute VF |
| 19 | De Winter T-waves | Upsloping ST dep + tall T V1–V6 | Treat as STEMI, activate cath lab |