Describe the various techniques of phonosurgery in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
phonosurgery techniques vocal fold
Searching the Web
RGUHS phonosurgery techniques 50 marks ENT question answer
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
PHONOSURGERY - TECHNIQUES IN DETAIL
(50 Marks Answer - RGUHS Pattern)
Sources: Scott-Brown's Otorhinolaryngology HNS, Cummings Otolaryngology HNS, Dhingra, Hazarika, Stell & Maran, Zakir Hussain, and recent literature
DEFINITION
Phonosurgery (Hirano, 1975) refers to any surgery with the primary goal of improving, restoring, or maintaining voice quality. The term was formally introduced by Hirano M (Otologia 21:239, 1975) and encompasses any procedure that alters laryngeal structure or dynamics to achieve the desired voice outcome.
Scott-Brown's ORL HNS, Ch. 67: "Phonosurgery refers to any surgery designed primarily for the maintenance, restoration or enhancement of the voice."
CLASSIFICATION / OVERVIEW FLOWCHART
PHONOSURGERY
|
┌───────────────────┼────────────────────┐
│ │ │
PHONOMICROLARYNGOSCOPY INJECTION LARYNGEAL
(Microlaryngeal Surgery) LARYNGOPLASTY FRAMEWORK
SURGERY
│ │
┌───────┴───────┐ ┌────────┴────────┐
Temporary Permanent Isshiki Types I-IV
Materials Materials + Arytenoid
(Gelfoam, HA) (Silicone, Adduction
Fat) + Cricothyroid
Approximation
PLUS:
└─ RLN REINNERVATION (Selective / Non-selective)
└─ LARYNGEAL PACING
└─ VOCAL FOLD AUGMENTATION (Recent advances)
I. PRE-OPERATIVE ASSESSMENT
Before any phonosurgery is undertaken, the following are mandatory:
- Perceptual voice assessment - GRBAS scale (Grade, Roughness, Breathiness, Asthenia, Strain)
- Videolaryngostroboscopy - gold standard; evaluates mucosal wave, glottic closure, symmetry
- Acoustic analysis - fundamental frequency (F0), jitter, shimmer, NHR
- Aerodynamic analysis - MPT (Maximum Phonation Time), phonation threshold pressure
- Patient-reported outcomes - Voice Handicap Index (VHI), Voice-Related Quality of Life (V-RQOL)
- Radiology - CT larynx in selected cases
Cummings, p.1153: Percutaneous medialization by injection should be considered in patients with short life expectancy and aspiration or severe dysphonia.
II. PHONOMICROSURGERY (Microlaryngoscopy Surgery)
A. History
- 1852: Horace Green - first direct laryngeal surgery (polyp in a child)
- 1960s: Oskar Kleinsasser - adaptation of operating microscope to direct laryngoscopy
- 1970s-80s: Vaughan, Jako, Strong - CO2 laser applied to larynx
- 1990s: Zeitels - cold dissection microflap techniques
B. Anatomy - Vocal Fold Microstructure (Hirano's Body-Cover Model)
LAYERS OF VOCAL FOLD (Hirano 1974):
┌─────────────────────────────┐
│ EPITHELIUM (squamous) │ ← Cover
├─────────────────────────────┤
│ SUPERFICIAL LAMINA │ ← Cover (Reinke's space)
│ PROPRIA (SLP) │
├─────────────────────────────┤ ← Transition zone
│ INTERMEDIATE LP │
├─────────────────────────────┤
│ DEEP LP (vocal ligament) │
├─────────────────────────────┤
│ THYROARYTENOID MUSCLE │ ← Body (vocalis)
└─────────────────────────────┘
KEY PRINCIPLE: All surgery must preserve SLP (Reinke's space)
and vocal ligament to prevent scarring and dysphonia
C. Equipment Required (Scott-Brown's key points)
- Laryngoscope: Lindholm, Kleinsasser, Dedo, or Zeitels universals scope
- Suspension system: Lewy arm or Boyles table
- Microscope: Operating microscope, 400 mm lens
- 0° and 30° telescopes for inspection
- Microinstruments: Atraumatic grasping forceps, microscissors, sickle knife, angled suction
- CO2 laser or angiolytic laser (KTP, PDL) as adjunct
- Anaesthesia: TIVA (total IV anaesthesia) with muscle relaxation; jet ventilation or apnoeic technique
D. Techniques for Specific Pathologies
1. VOCAL FOLD NODULES
SURGICAL STEPS - Cold Dissection:
Step 1: Suspend laryngoscope - expose both vocal folds
Step 2: Inspect with 70° telescope - confirm bilateral mid-membranous location
Step 3: Grasp centre of nodule with atraumatic forceps
Step 4: Retract medially toward opposite cord
Step 5: Cut mucosa at base with microscissors (cold)
→ Produces straight vibratory edge
→ Prevents secondary notching
Step 6: Repeat contralateral side if needed
(no contraindication to bilateral excision at same sitting)
NOTE: Preserves vocal ligament; avoids Reinke's space entry
Indications: Failure of voice therapy (nodules should RARELY require surgery)
2. VOCAL FOLD POLYP
SURGICAL STEPS:
Step 1: Suspend + inspect
Step 2: Grasp polyp with atraumatic forceps
Step 3: Apply gentle, steady traction toward opposite cord
Step 4: Section base of polyp (cold instruments or CO2 laser)
Step 5: Check for contact lesion on contralateral fold
(usually should NOT be addressed)
NOTE: Superficial to vocal ligament; wide base = microflap technique
3. REINKE'S OEDEMA (Polypoid Corditis)
SURGICAL STEPS (Cordotomy technique):
Step 1: Make cordotomy incision on SUPERIOR aspect of VF
(NOT medial edge - preserves vibratory margin)
Step 2: Elevate mucosa carefully with elevator
Step 3: Aspirate or remove myxoedematous/gelatinous contents
Step 4: Replace mucosal flaps
Step 5: Trim excess epithelium
Step 6: Lay flap onto surface; heals by surface tension
IMPORTANT: Only after smoking cessation; bilateral at same setting is safe
4. VOCAL FOLD CYSTS
Two types:
- Epidermoid (retention) cysts - true capsule; within epithelium
- Ductal retention cysts - mucous gland obstruction
MICROFLAP TECHNIQUE (Bouchayer-Cornut):
Step 1: Sickle knife incision along superior surface of VF
(lateral to medial edge)
Step 2: Elevate epithelial-SLP mucosal flap
Step 3: Dissect cyst from surrounding SLP bluntly
Step 4: Remove intact cyst (avoid rupture to prevent recurrence)
Step 5: Replace mucosal flap; no sutures needed
CRITICAL: Preserve vocal ligament; no raw areas on vibratory edge
5. RECURRENT RESPIRATORY PAPILLOMATOSIS (RRP)
- Caused by HPV types 6 and 11 (Dhingra; Hazarika)
- Surgical goal: maintain an airway and preserve voice - NOT cure
- Excision repeated as needed (no definitive cure)
Options:
| Method | Advantage | Disadvantage |
|---|---|---|
| CO2 Laser | Precise, haemostatic | Scarring risk, no histology |
| KTP/PDL Laser (angiolytic) | Targets vasculature, less thermal spread | Office procedure |
| Microdebrider (powered shaver) | Fast, tissue preservation, histology possible | Bleeding |
| Cold steel | No thermal damage | Bleeding |
Adjuvant treatments: Cidofovir (intralesional), interferon-alpha, bevacizumab (recent), HPV vaccination (Gardasil - preventive)
6. SULCUS VOCALIS
- Sulcus = longitudinal groove in VF where epithelium is adherent to vocal ligament
- Classified by Ford: Type I (physiological furrow), Type II (sulcus vergeture), Type III (pit/pocket)
Surgical options:
- Intralesional steroid injection
- Fat augmentation injection
- Collagen injection
- Slicing mucosal technique (Pontes): parallel mucosal incisions in cephalad-to-cordal direction to break linear scar
- Microflap elevation with lateral undermining
7. VOCAL FOLD SCAR
- Most challenging phonosurgical problem
- Options: steroid injection, fat injection, hyaluronic acid injection, cover-body dissection
III. INJECTION LARYNGOPLASTY
History
- 1911: Brunings - first intracordal injection of paraffin
- 1962: Arnold - technique of intracordal injection using Teflon
- Current: Many safer materials available
Indications
- Unilateral vocal fold paralysis (cord in lateral/paramedian position)
- Vocal fold atrophy (presbylaryngis)
- Glottic insufficiency
- Sulcus vocalis
- Soft tissue defects post-excision
Injectable Materials
INJECTABLE MATERIALS FOR LARYNGOPLASTY:
┌──────────────────┬──────────────┬──────────────────────────────┐
│ Material │ Duration │ Notes │
├──────────────────┼──────────────┼──────────────────────────────┤
│ Gelfoam │ 6-8 weeks │ Temporary; reversible │
│ Cymetra (acell. │ 6-12 months │ Micronized AlloDerm; good │
│ dermal matrix) │ │ results; no inflammation │
│ Hyaluronic acid │ 6-12 months │ Favorable viscoelastic props │
│ (Restylane/Juv.) │ │ │
│ Autologous fat │ Long-term │ Slight over-injection needed;│
│ │ │ unpredictable resorption │
│ Collagen │ 3-6 months │ Bovine - inflammatory stiff- │
│ │ │ ness; now largely replaced │
│ Calcium hydroxy- │ Long-term │ Radiesse; granuloma risk; │
│ apatite (CaHA) │ │ caution advised (Cummings) │
│ Silicone │ Permanent │ PTFE/Teflon - DISCOURAGED; │
│ (PTFE/Teflon) │ │ granuloma; airway compromise │
└──────────────────┴──────────────┴──────────────────────────────┘
Note: Calcium hydroxyapatite has REPLACED Teflon as standard (Scott-Brown's)
Scott-Brown's, Key Points: "Materials such as calcium hydroxyapatite have replaced Teflon for vocal fold injection laryngoplasty."
Approaches to Injection
APPROACHES TO VOCAL FOLD INJECTION:
INJECTION LARYNGOPLASTY
│
┌───────────────┼───────────────┐
│ │ │
TRANSORAL PERCUTANEOUS LARYNGOSCOPIC
(Indirect) (Transcutaneous) (Microlaryngoscopy)
│ │ │
Curved laryn- Three routes: Under GA with
geal needle; 1) Lateral suspension; Brunings
topical through syringe; direct
anaesthesia; thyroid ala visualization
patient holds (preferred -
tongue out Cummings)
2) Anterior
via CTM
(subglottic)
3) Transthyrohyoid
Percutaneous Lateral Approach (Preferred - Cummings):
- Patient awake, no sedation; local anaesthesia
- Flexible fiberoptic laryngoscopy for visualization
- Needle passed through thyroid ala at level of vocal fold (midpoint of thyroid notch to inferior border of ala)
- Inject just anterior and lateral to vocal process
- Plane: lower border of medial edge of vocal fold
- Optimal: 0.5-1.0 mL Cymetra; slight over-injection preferred
- Immediate voice assessment
Key Principle: Inject into body of vocal fold (paraglottic space) - NOT into Reinke's space (SLP) - to avoid stiffening the cover
IV. LARYNGEAL FRAMEWORK SURGERY (LFS)
Definition & History
- First described by Isshiki (1974) - "Surgical alteration of vocal pitch"
- Defined as a procedure on the laryngeal cartilage to change position or tension on the vocal cords
- Performed under local anaesthesia (original description) for intra-operative auditory feedback
- Four types described by Isshiki
Isshiki's Four Types of Thyroplasty
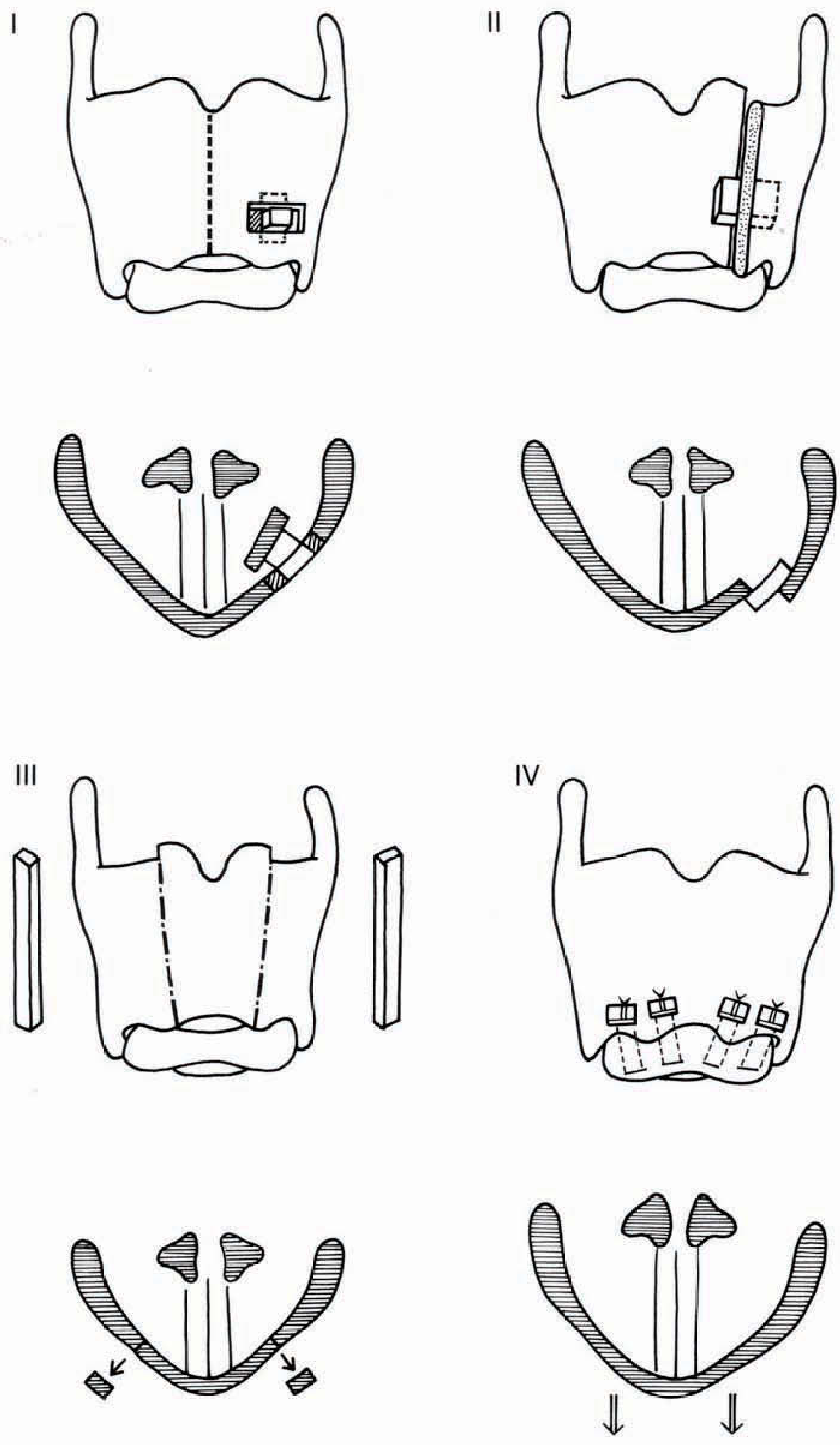
Figure: Isshiki Types I-IV Laryngeal Framework Thyroplasties. Top row - anterior views of thyroid cartilage showing implant positions. Bottom row - axial cross-sections showing resultant cord positions.
ISSHIKI CLASSIFICATION:
TYPE I - MEDIALIZATION THYROPLASTY (Lateral Compression)
├── Goal: Medialize a laterally positioned vocal fold
├── Indications: Unilateral VF paralysis, vocal fold atrophy, sulcus
├── Window dimensions: ~5mm x 13mm, located in inferior half of thyroid ala
├── Implants: Silastic (carved), hydroxyapatite (VoCoM), Gore-Tex
└── Effect: Cord moves medially → improved glottic closure → better voice
TYPE II - LATERALIZATION THYROPLASTY (Expansion)
├── Goal: Open/lateralize the vocal folds (expand glottis)
├── Indication: Bilateral adductor spasmodic dysphonia (adductor SD)
├── A lateral-spreading implant is placed to open the thyroid cartilage
└── Effect: Reduced VF tension and contact → less spasm
TYPE III - RELAXATION THYROPLASTY (Shortening)
├── Goal: Lower pitch by relaxing/shortening the VF
├── Indication: Mutational falsetto (puberphonia), excessively high pitch
├── Technique: Removes small thyroid cartilage section to approximate
│ arytenoids to anterior commissure (shorten VF)
└── Effect: VF shortening → lower fundamental frequency (F0)
TYPE IV - TENSION THYROPLASTY / CRICOTHYROID APPROXIMATION
├── Goal: Raise pitch (increase VF tension)
├── Indication: MTF (Male-to-Female transsexuals), feminization laryngoplasty
│ Unilateral VF paralysis (pitch elevation)
├── Technique: Suture between inferior border of thyroid cartilage and
│ superior border of cricoid cartilage anteriorly
│ (approximates the two cartilages, stretching the VF)
└── Effect: VF elongation → raised F0 → higher (feminine) pitch
Thyroplasty Type I - Detailed Technique (Scott-Brown; Cummings)
THYROPLASTY TYPE I - STEP BY STEP:
Pre-op: Voice assessment, stroboscopy, CT larynx (optional)
Step 1: Patient supine; paramedian horizontal neck incision
(5 cm) over middle of thyroid lamina
Step 2: Subplatysmal flaps; split strap muscles in midline;
retract off ipsilateral thyroid lamina
(preserve outer perichondrium if using Gore-Tex)
Step 3: Define landmarks:
- Thyroid notch (superior)
- Inferior border of thyroid ala
- Midline
Step 4: Window position:
- CRITICAL: Inferior half of thyroid ala
- NOT too superior (displaces false cord - common error)
- Approximate dimensions: 5 mm (height) x 10-13 mm (width)
- Vocal cord lies at midpoint of window
Step 5: Score outer perichondrium with template
Step 6: Create cartilage window (preserve or remove cartilage island)
Preserve inner perichondrium
Step 7: Temporarily displace inner perichondrium medially to assess voice
Step 8: Shape implant (Silastic block or prefabricated system)
VoCoM implants: 3-7 mm displacement variants
Netterville system; Montgomery implants
Step 9: Insert implant while patient phonates (local anaesthesia)
Adjust position until optimal voice achieved
Step 10: Close in layers; drain optional
(NO suturing of implant - remains in window by compression)
Common Error: Window placed TOO HIGH → displaces false cord,
not true cord → poor voice outcome
Arytenoid Adduction (Isshiki, 1978)
ARYTENOID ADDUCTION - TECHNIQUE:
Indications: Large posterior glottic gap; paralyzed cord at different
vertical level to normal cord
Access: Extended neck incision; approach posterior thyroid lamina
Step 1: Expose posterior thyroid ala
Step 2: Identify and dissect muscular process of arytenoid
Step 3: Divide attached muscles (posterior cricoarytenoid, interarytenoid)
Step 4: Place suture through muscular process
Step 5: Rotate arytenoid to adducted position by pulling suture anteriorly
(simulates adductor muscle pull)
Step 6: Fix suture to inferior horn of thyroid cartilage
Step 7: Combine with Type I thyroplasty for optimal results
Result: Closes posterior glottic gap; corrects vertical height discrepancy
Zeitels Modification: Arytenoid fixation + cricothyroid subluxation
- Arytenoid fixed in midline position
- Suture placed between inferior horn of thyroid cartilage and cricoid cartilage anteriorly
- Provides both tension and bulk to paralyzed cord
- Combined with medialization thyroplasty
V. CRICOTHYROID APPROXIMATION (CTA) / TYPE IV THYROPLASTY
Most common indication: Male-to-female gender affirming laryngoplasty (feminization)
CTA - TECHNIQUE:
Step 1: Horizontal incision at level of CTM
Step 2: Expose cricoid and inferior thyroid borders anteriorly
Step 3: Place 2-3 permanent sutures between thyroid inferior border
and cricoid superior border
Step 4: Tie under phonation until desired pitch achieved
(local anaesthesia - patient phonates "ee")
Step 5: Final F0 increase: typically 50-100 Hz above baseline
Alternative: Glottoplasty (Wendler); Laser vocal fold shortening (recent)
VI. REINNERVATION PROCEDURES
A. Non-selective Reinnervation (Scott-Brown)
- Indication: Hoarseness from unilateral adductor VF paralysis
- Donor nerve: Ansa cervicalis (ansa hypoglossi)
- Technique: Neck incision at cricoid level; ansa cervicalis anastomosed to RLN using 9/0 nylon
- Goal: Maintain muscle bulk (prevent atrophy), not restore motion
- Takes 6-12 months for effect
B. Selective Reinnervation (Scott-Brown)
- Indication: Stridor from bilateral abductor VF paralysis
- Technique: Complex; uses C3 root of phrenic nerve with cable graft (great auricular nerve - Y-shaped) inserted into BOTH posterior cricoarytenoid muscles; ansa hypoglossi-RLN anastomosis bilaterally
- Goal: Selective reinnervation of abductor muscles (PCA)
REINNERVATION FLOWCHART:
VF PARALYSIS
│
├── UNILATERAL
│ │
│ ├── Short-term/uncertain recovery
│ │ └── INJECTION LARYNGOPLASTY (temporary)
│ │
│ └── Permanent/12 months wait
│ ├── TYPE I THYROPLASTY ± Arytenoid adduction
│ └── ANSA-RLN REINNERVATION (± thyroplasty)
│
└── BILATERAL
│
├── Airway compromise → TRACHEOSTOMY (acute)
│
└── Long-term management:
├── Laser posterior cordotomy / arytenoidectomy
└── SELECTIVE REINNERVATION (PCA)
VII. LARYNGEAL PACING
- Concept: Functional electrical stimulation of laryngeal muscles
- Indication: Bilateral VF paralysis to restore phasic abduction during inspiration
- Device: Implantable neurostimulator; electrodes placed on PCA muscles
- Synchronized with respiratory cycle via respiratory sensors
- Experimental but promising; avoids permanent tracheostomy/arytenoidectomy
VIII. SURGICAL LASERS IN PHONOSURGERY
LASER OPTIONS:
┌──────────────────┬────────────┬────────────────────────────────┐
│ Laser Type │ Wavelength │ Application │
├──────────────────┼────────────┼────────────────────────────────┤
│ CO2 │ 10,600 nm │ Standard; precise ablation; │
│ (gold standard) │ │ vaporizes tissue; no histology │
│ KTP (532 nm) │ 532 nm │ Angiolytic; vasc. lesions; │
│ │ │ RRP; hemorrhagic polyps; │
│ │ │ office-based procedure │
│ Pulsed dye laser │ 585 nm │ Angiolytic; RRP; papillomatosis│
│ (PDL) │ │ │
│ Nd:YAG │ 1064 nm │ Deeper penetration; hemangioma │
│ Diode │ 810/980 nm │ Contact cutting; hemostasis │
└──────────────────┴────────────┴────────────────────────────────┘
CO2 Laser Parameters (Scott-Brown):
- Spot size: 0.5-1.0 mm (microspot = 0.2-0.3 mm)
- Power: 2-5 W for VF surgery
- Mode: Pulsed/SuperPulse preferred (less thermal spread)
- Tissue effect: Vaporization > coagulation
HAZARDS: Endotracheal tube fire; eye protection; smoke plume
Microspot CO2 laser vs cold dissection (Benninger, Laryngoscope 2000):
- Prospective RCT: Both achieve equivalent voice outcomes for benign VF lesions
- Cold steel = less thermal injury, allows histology
- Laser = haemostasis, precision; risk of over-ablation
IX. OFFICE-BASED (AWAKE) PHONOSURGERY - Recent Advances
A growing trend in modern phonosurgery:
- Performed in clinic under topical anaesthesia (4% lidocaine nebulized)
- Visualized via chip-tip flexible laryngoscope
- Uses: KTP laser, PDL laser, injection procedures (CaHA, HA)
- Advantages: No GA risk, immediate voice feedback, repeat visits, cost-effective
- Indications: RRP, hemorrhagic polyps, vocal fold augmentation, Reinke's edema
X. RECENT ADVANCES (2020-2026)
| Advance | Details |
|---|---|
| Stem cell therapy | Mesenchymal stem cells + hyaluronic acid scaffolds for VF scar repair (experimental) |
| Platelet-rich plasma (PRP) | Autologous PRP injection for VF scar and sulcus; promotes lamina propria regeneration |
| Biomaterial scaffolds | HA-based hydrogels with viscoelastic properties matching native SLP (e.g., Prolaryn, Juvederm Vocal) |
| Robotic phonosurgery | Transoral robotic surgery (TORS) extending to microsurgery; increased precision |
| Laser refinements | Thulium laser (2013 nm); 532 nm KTP/PDL for office RRP with reduced scarring vs CO2 |
| Glottoplasty modifications | Wendler's laser glottoplasty and anterior glottal web creation for pitch elevation in MTF |
| Nerve transfer innovations | Hypoglossal-RLN anastomosis; combined reinnervation + thyroplasty approaches |
| 3D-printed implants | Patient-specific thyroplasty implants using 3D printing for optimal medialization |
| Bevacizumab (Avastin) | Anti-VEGF intralesional injection for recurrent RRP (PMID 37433709) |
| HPV vaccination | Gardasil 9 reduces RRP recurrence rates; prophylactic for juvenile-onset RRP |
Recent systematic review (Maniaci et al., Am J Otolaryngol 2024, PMID 38071789): Surgical techniques for sulcus vocalis show variable outcomes; no single technique definitively superior; combination of mucosal techniques with augmentation shows best perceptual and acoustic results.
XI. COMPLICATIONS OF PHONOSURGERY
COMPLICATIONS:
PHONOMICROSURGERY:
├── Immediate: Dental trauma, laryngospasm, subglottic edema
├── Early: Hematoma, infection, granuloma at contact areas
└── Late: VF scar (most dreaded), synechiae (anterior commissure
web), incomplete excision → recurrence
INJECTION LARYNGOPLASTY:
├── Over-injection → airway compromise, stiff voice
├── Under-injection → persistent dysphonia
├── Misplaced injection into Reinke's space → stiffness
├── Teflon/PTFE granuloma (historical)
├── CaHA granuloma (rare, reported in literature - Cummings)
└── Infection, haematoma
FRAMEWORK SURGERY:
├── Implant extrusion (Gore-Tex reported - Cummings)
├── Implant malposition (too superior = most common error)
├── Airway compromise (over-medialization)
├── Infection of implant
└── Granulomatous reaction (foreign body)
XII. MANAGEMENT ALGORITHM - DYSPHONIA
PATIENT WITH DYSPHONIA
│
▼
FULL ASSESSMENT
(History, stroboscopy, acoustic analysis, VHI)
│
▼
DIAGNOSIS
┌──────────────────────────────────────────────┐
│ │
BENIGN LESIONS VOCAL FOLD PARALYSIS
(Nodule, Polyp, ┌──────────┴──────────┐
Cyst, Reinke's) UNILATERAL BILATERAL
│ │ │
▼ │ Airway threatened?
VOICE THERAPY (SLT) │ YES → Tracheostomy
│ ▼ NO → Laser arytenoidectomy
▼ <12 months? / Selective reinnervation
FAILS or Injection
RECURS? laryngoplasty
│ (temporary)
▼ │
PHONOSURGERY >12 months
• Microflap (permanent)
• Cold dissection │
• Laser ▼
• Cordotomy TYPE I THYROPLASTY
(Reinke's) ± Arytenoid adduction
± Reinnervation
SUMMARY TABLE - ISSHIKI PROCEDURES AT A GLANCE
| Type | Name | Goal | Indication | Effect on Pitch |
|---|---|---|---|---|
| I | Medialization thyroplasty | Medialize VF | Unilateral VF paralysis, atrophy | Mild rise (closures better) |
| II | Lateralization thyroplasty | Open glottis | Adductor spasmodic dysphonia | Lower |
| III | Relaxation thyroplasty | Shorten VF | Puberphonia, mutational falsetto | Lower F0 |
| IV | Cricothyroid approximation | Tighten/lengthen VF | MTF transsexual; VF paralysis (pitch) | Raise F0 |
KEY POINTS (for RGUHS exam)
- Term "Phonosurgery" coined by Hirano (1975); defined by Ford and Bless
- Videolaryngostroboscopy is mandatory pre-op assessment
- The microflap technique (Bouchayer-Cornut) preserves Reinke's space - gold standard for cysts and sulcus
- Nodules should RARELY need surgery; voice therapy is first line
- Isshiki Type I = medialization thyroplasty; window in inferior half of thyroid ala
- Ansa cervicalis-RLN anastomosis = maintains VF bulk in unilateral paralysis
- Calcium hydroxyapatite has replaced Teflon for injection laryngoplasty
- KTP/PDL laser = preferred for angiolytic office phonosurgery (RRP, vascular polyps)
- Type IV thyroplasty/CTA = pitch elevation for MTF transsexuals (feminization laryngoplasty)
- Complications: over-injection → airway; implant too high → false cord displaced; VF scar = most feared phonosurgical complication
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (8th Ed.), Chs. 67, 78, 79 - Phonosurgery; Medialization; Injection laryngoplasty
- Cummings Otolaryngology Head and Neck Surgery (7th Ed.), Ch. 62 - Paralysis of the larynx; Vocal fold injection; Medialization thyroplasty
- Dhingra PL - Diseases of Ear, Nose and Throat (7th Ed.) - Phonosurgery
- Hazarika P - Textbook of ENT and Head & Neck Surgery
- Stell & Maran's Head and Neck Surgery - Laryngeal surgery
- Zakir Hussain - ENT for entrance examinations
- Hirano M. Phonosurgery - basic and clinical investigations. Otologia 1975;21:239
- Isshiki N et al. Thyroplasty type I. Acta Otolaryngol 1975;80:465
- Benninger MS. Microdissection or microspot CO2 laser for limited vocal fold benign lesions. Laryngoscope 2000;110:1-17
- Maniaci A et al. Perceptual, aerodynamic and acoustic outcomes of surgical technique for sulcus vocalis: A systematic review and meta-analysis. Am J Otolaryngol 2024 [PMID 38071789]
- IJHNS - Principles of Phonosurgery - Review article
This is a shared conversation. Sign in to Orris to start your own chat.