Osteomyelitis orthopedic
Reading File
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND "orthopedic"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive material. Let me synthesize a complete, well-organized answer.
Osteomyelitis — Orthopedic Review
Definition & Pathogenesis
Osteomyelitis is inflammation of bone and marrow, virtually always caused by infection. Organisms reach bone via three routes:
- Hematogenous spread — most common in children; bacteremia from trivial mucosal injuries or minor skin infections
- Contiguous focus — spread from adjacent soft tissue infection, diabetic foot ulcers, pressure sores
- Direct implantation — open fractures, surgical procedures, joint arthroplasty
Staphylococcus aureus causes 80–90% of culture-positive pyogenic osteomyelitis; its cell-wall proteins bind collagen and other bone matrix components, facilitating bacterial adherence. — Robbins Pathologic Basis of Disease
Classification
| Type | Key Feature | Typical Route |
|---|---|---|
| Acute hematogenous (AHO) | Children, long bones, metaphysis | Hematogenous |
| Subacute | Insidious onset, Brodie abscess | Hematogenous |
| Chronic | Sequestrum, involucrum, sinus tracts | Any |
| Contiguous / post-traumatic | Open fracture, surgery, bite | Direct / contiguous |
| Vertebral (spondylodiscitis) | Adults, lumbar > cervical | Hematogenous |
| Prosthetic joint / device | Pain after arthroplasty | Direct / hematogenous |
| Diabetic foot | Polymicrobial, poor vascularity | Contiguous |
Age-Based Microbiology
| Population | Organisms |
|---|---|
| Neonates | Group B Streptococcus, E. coli, S. aureus |
| Children (>1 mo) | S. aureus (MRSA most common in AHO), Streptococcus pyogenes, Kingella kingae |
| Adults (healthy) | S. aureus (MSSA or MRSA) |
| Sickle cell disease | Salmonella spp., S. aureus |
| IV drug users | Pseudomonas aeruginosa, S. aureus |
| Open fractures / surgery | Polymicrobial (gram-negatives, anaerobes) |
| Diabetic foot | Polymicrobial |
Anatomy of Infection by Age
The osseous vascular circulation determines location:
- Neonates: Metaphyseal vessels penetrate the growth plate → metaphysis, epiphysis, and joint involvement all common → risk of septic arthritis and permanent joint damage
- Older children: Metaphysis predominates (distal femur, proximal tibia, proximal humerus)
- Adults: After growth plate closure, metaphyseal-epiphyseal anastomoses form → epiphyseal and subchondral involvement; vertebrae are the most common adult site
Pathological Stages
Acute (< 2 weeks)
- Bacteria proliferate → neutrophilic infiltrate
- Bone cell/marrow necrosis within 48 hours
- Spread through Haversian canals to periosteum
- Subperiosteal abscess (especially in children, where periosteum is loosely attached)
- Lifting of periosteum impairs blood supply → further necrosis
Subacute
- Brodie abscess: well-defined lytic lesion with a sclerotic rim, usually in metaphysis
- "Penumbra sign" on MRI: peripheral high-signal ring (granulation tissue) surrounding low-signal central abscess cavity
Chronic
- Sequestrum: fragment of necrotic dead bone separated from viable bone
- Involucrum: periosteal new bone that forms around and encases the sequestrum
- Sinus tracts: channels from medullary cavity through involucrum gaps to the skin surface
- Refractory to antibiotics alone; requires surgical debridement
Clinical Features
Acute: Fever, rigors, point tenderness over infected bone, localized warmth, soft tissue swelling and erythema. Children may limp or refuse to bear weight.
Chronic: More indolent; palpable involucrum or sequestrum may be felt; draining sinus tracts; less systemic toxicity.
Vertebral osteomyelitis (adults): Back pain ± radicular pain, sensory loss, lower extremity weakness, urinary/bowel dysfunction — cord compression signs = emergency.
Investigations
Laboratory
- ESR and CRP — elevated (low specificity, but valuable for monitoring treatment response; CRP is more reliable)
- WBC — may be normal in chronic disease
- Blood cultures — positive in ~40% of pediatric AHO, guides therapy
Imaging Algorithm
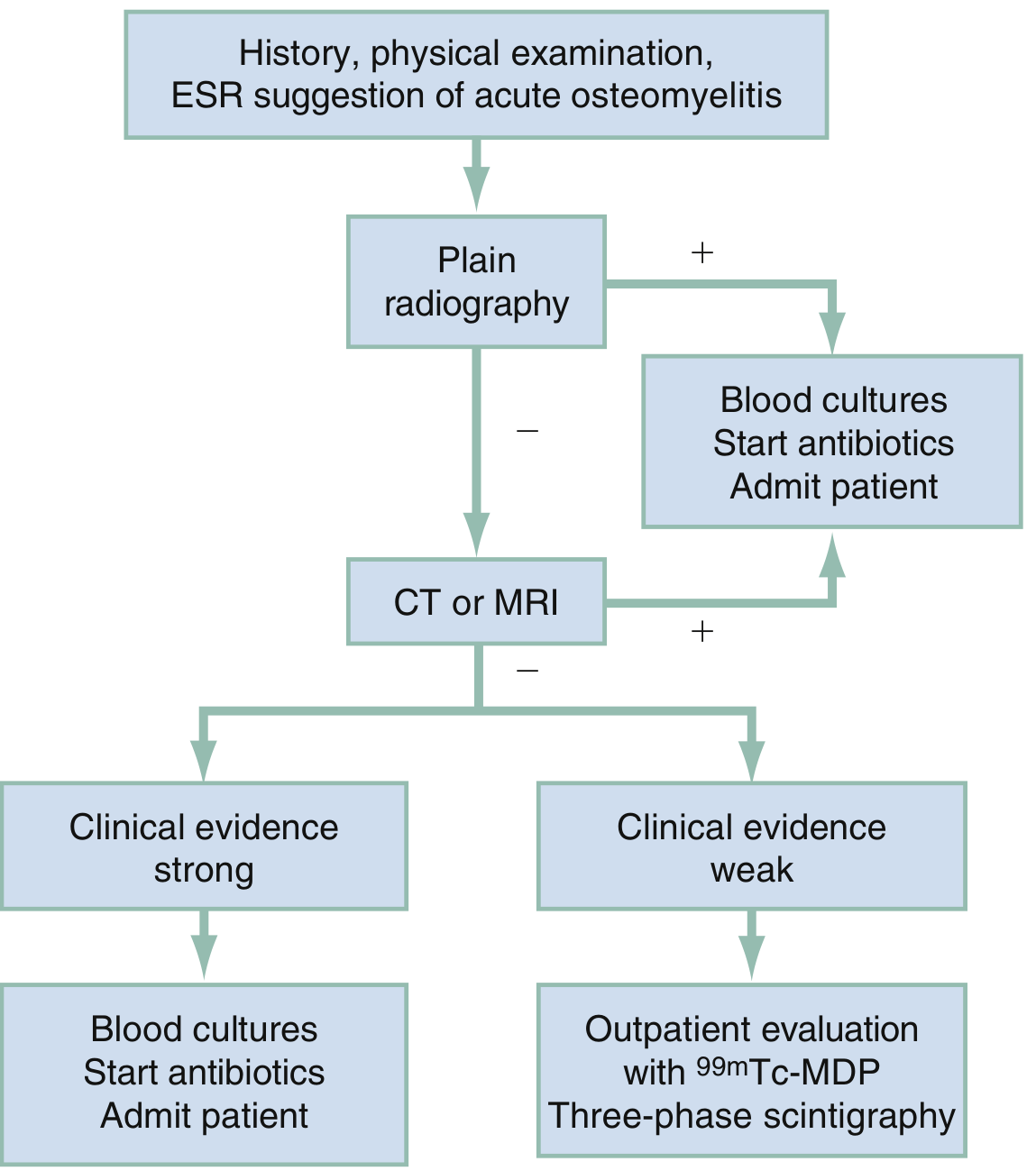
| Modality | Role | Findings |
|---|---|---|
| Plain X-ray | First-line; may miss early disease | Soft tissue swelling, cortical irregularity, periosteal reaction — changes lag 2 weeks |
| MRI | Gold standard — highest sensitivity and specificity | Bone marrow edema, periosteal reaction, soft tissue extension, abscess; contrast defines abscess rim |
| CT | Best for cortical detail and sequestrum | Cortical destruction, sequestra; guides needle aspiration in vertebral disease |
| Ultrasound | Children; non-invasive | Subperiosteal abscess, fluid collection; guides aspiration |
| ³⁹ᵐTc-MDP bone scan | Outpatient when MRI unavailable | Three-phase scintigraphy; sensitive but not specific; useful for multifocal disease |
MRI signal: T1 low signal replacing normal fatty marrow; T2/STIR high signal edema; post-gadolinium enhancement of granulation tissue. — Grainger & Allison's Diagnostic Radiology
Treatment
Antibiotic Principles
- Obtain blood cultures and tissue/bone cultures before starting antibiotics whenever safe
- Empiric coverage directed at S. aureus; adjust by culture/sensitivity
- Duration: 4–6 weeks total (IV initially, then oral once clinical improvement is documented and no further debridement needed)
- CRP and ESR used to monitor response; failure to normalize within 2–3 weeks → consider inadequate source control
Empiric Antibiotic Selection
| Setting | Empiric Regimen |
|---|---|
| Children / healthy adults (MSSA suspected) | Anti-staphylococcal penicillin (oxacillin/nafcillin) or cefazolin |
| MRSA suspected (community-acquired, endemic areas) | Vancomycin or daptomycin |
| Sickle cell disease | Cover both Salmonella and S. aureus (e.g., fluoroquinolone + MSSA cover) |
| Open fracture / polymicrobial | Broad-spectrum (piperacillin-tazobactam or carbapenem) |
| Vertebral osteomyelitis | Await culture; vancomycin empirically |
Surgical Indications
- Chronic osteomyelitis — all necrotic bone (sequestrum) and soft tissue must be debrided; antibiotics alone are insufficient
- Subperiosteal or soft tissue abscess that fails to resolve with antibiotics
- Spinal cord compression — urgent surgical decompression
- Prosthetic joint infection (acute, <3 months): Debridement, irrigation, and prosthetic retention (DAIR) with antibiotic therapy; hardware retained if stable and fracture not yet healed
- Prosthetic joint infection (chronic or unstable hardware): Hardware removed; two-stage revision preferred
Orthopedic Hardware Decisions
- Infected hardware over an unhealed fracture → retain if stable (hardware provides structural stability); convert to external fixation if unstable
- Infected hardware over a healed fracture → remove hardware + debride all necrotic bone/tissue — Schwartz's Principles of Surgery
Complications
| Complication | Notes |
|---|---|
| Septic arthritis | Especially in neonates (joint directly invaded); also contiguous spread |
| Chronic osteomyelitis | Sequestrum/involucrum; refractory to antibiotics alone |
| Growth disturbance | If epiphysis involved in children → limb-length discrepancy, angular deformity |
| Pathologic fracture | Through infected/weakened bone |
| Bacteremia / sepsis | Hematogenous dissemination |
| Spinal cord compression | Vertebral osteomyelitis + epidural abscess |
| Sinus tracts | Chronic draining cutaneous fistulae |
| Squamous cell carcinoma | Rare, Marjolin's ulcer at chronic sinus tract (long-standing cases) |
Special Scenarios
Diabetic Foot Osteomyelitis: Peripheral vascular disease + neuropathy create a hostile environment; diagnosis confirmed with "probe-to-bone" test, MRI, and biopsy; often requires prolonged antibiotic therapy and vascular intervention alongside debridement.
Vertebral Osteomyelitis / Discitis: In adults, back pain + elevated inflammatory markers; MRI confirms disc-space involvement + endplate erosion. CT-guided aspiration for culture (positive 30–60%). Usually resolves with conservative antibiotics; surgery for neurological compromise, instability, or failed medical therapy.
CRMO (Chronic Recurrent Multifocal Osteomyelitis): Non-bacterial, autoinflammatory; predominantly adolescents; sterile bone lesions at multiple sites; treated with NSAIDs, bisphosphonates, or biologics (TNF inhibitors).
Sources: Rosen's Emergency Medicine 9e · Robbins & Kumar Pathologic Basis of Disease · Grainger & Allison's Diagnostic Radiology · Schwartz's Principles of Surgery 11e · Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.