Laryngocele
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Here is a comprehensive review of laryngocele based on Cummings Otolaryngology and KJ Lee's Essential Otolaryngology.
Laryngocele
Definition
A laryngocele is an abnormal air-filled dilatation (diverticulum) of the saccule (appendix) of the laryngeal ventricle, communicating with the laryngeal lumen through a patent saccular orifice. When the orifice becomes obstructed and the sac fills with mucus, it is termed a saccular cyst; when it fills with pus, it becomes a laryngopyocele.
- Cummings Otolaryngology, p. 1127
Relevant Anatomy
The laryngeal saccule (appendix) is a small, blind outpouching at the anterior end of the laryngeal ventricle. It extends superiorly between the false vocal fold and the inner surface of the thyroid cartilage, just posterolateral to the petiole of the epiglottis. It contains numerous mucous glands whose secretions lubricate the true vocal folds. Normal saccule length is 6-8 mm in 75% of people, with 25% measuring ≥10 mm.
Classification
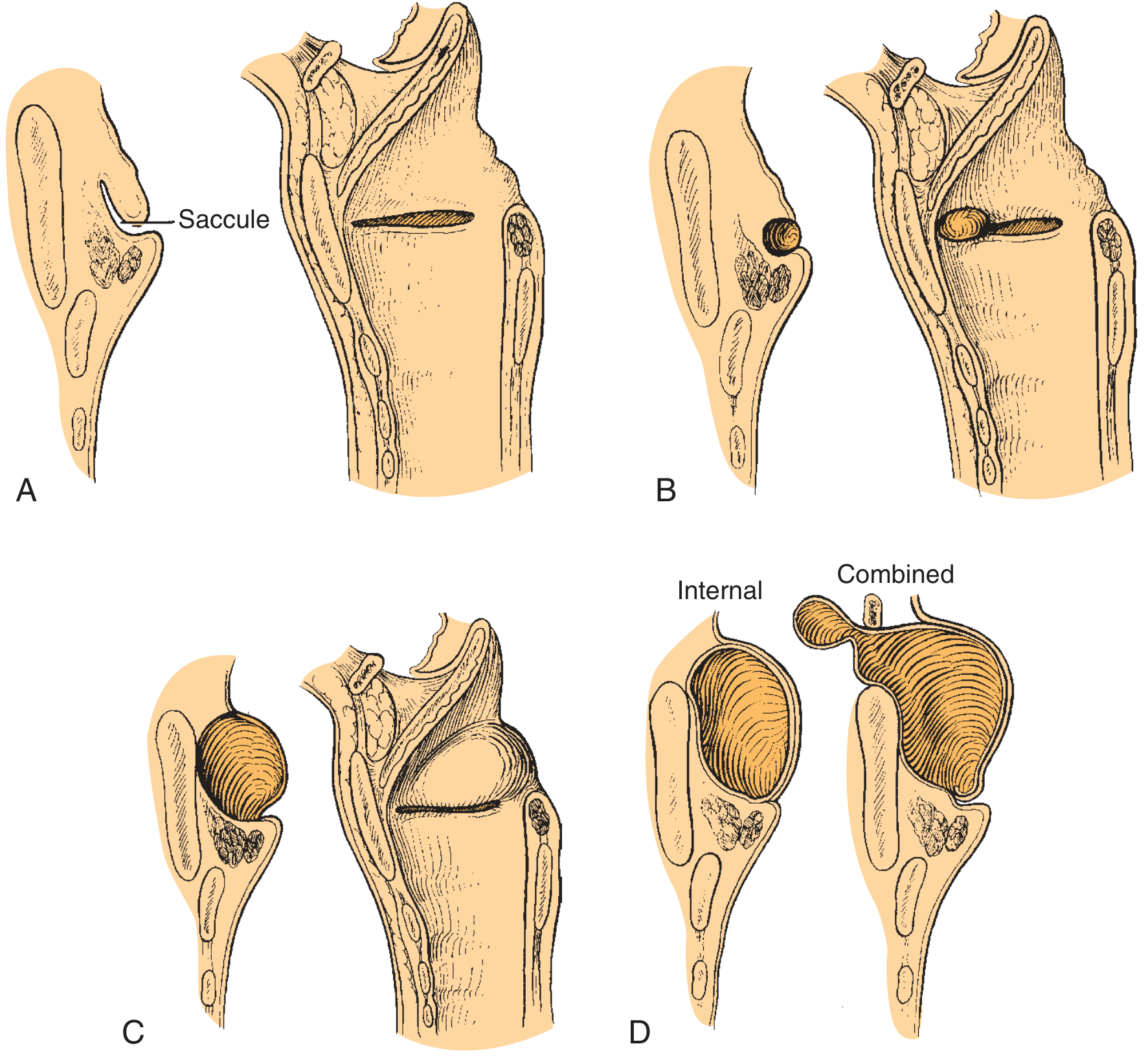
Fig. Classification of laryngocele/saccular cyst - Cummings Otolaryngology
By Contents
| Type | Contents | Orifice |
|---|---|---|
| Laryngocele | Air | Patent |
| Saccular cyst (mucocele) | Mucus | Blocked |
| Laryngopyocele | Pus | Blocked |
By Location
| Type | Description |
|---|---|
| Internal | Entirely within the thyroid cartilage framework; expands the false vocal fold and aryepiglottic fold medially, may bulge the piriform sinus laterally |
| External | Dilated air sac passes through the thyrohyoid membrane to present as a neck mass |
| Combined (mixed) | Has both internal and external components; most common type |
Almost 25% of laryngoceles are bilateral.
Etiology
-
Congenital: In infants, saccular disorders are likely congenital
-
Increased intrapharyngeal/transglottic pressure: Associated with trumpet players, glass blowers, wind instrument players, and people who use their voice forcefully (though this association may be overstated per Stell and Maran)
-
Laryngeal carcinoma: An obstructing tumor at the saccular orifice is an important and well-documented cause - 5% to 29% of laryngoceles may be associated with a small ventricular carcinoma
-
Idiopathic: Often no clear cause is identified
-
Cummings Otolaryngology, p. 1127; KJ Lee's Essential Otolaryngology, p. 924
Clinical Features
Symptoms (in order of frequency)
- Hoarseness - from downward pressure on the vocal fold or premature closure of the laryngeal vestibule at the false-fold level during phonation
- Stridor
- Dysphagia
- Sore throat
- Snoring
- Cough
- Neck mass - external component presents as a lateral neck swelling at the thyrohyoid membrane level; classically increases in size with a "puffing" (Valsalva-like) maneuver
In Infants (congenital lateral saccular cysts)
- Abnormal/weak cry
- Inspiratory stridor
- Cyanosis and dysphagia
Examination Signs
- Submucosal bulge of the false vocal fold and aryepiglottic fold on laryngoscopy
- Palpable neck mass at the thyrohyoid membrane (external component)
- Bryce sign: a gurgling sound heard over a neck mass - classic for laryngocele
Diagnosis
Diagnosis rests on a combination of clinical history, laryngoscopy, and cross-sectional imaging.
Imaging
CT scan is the investigation of choice:
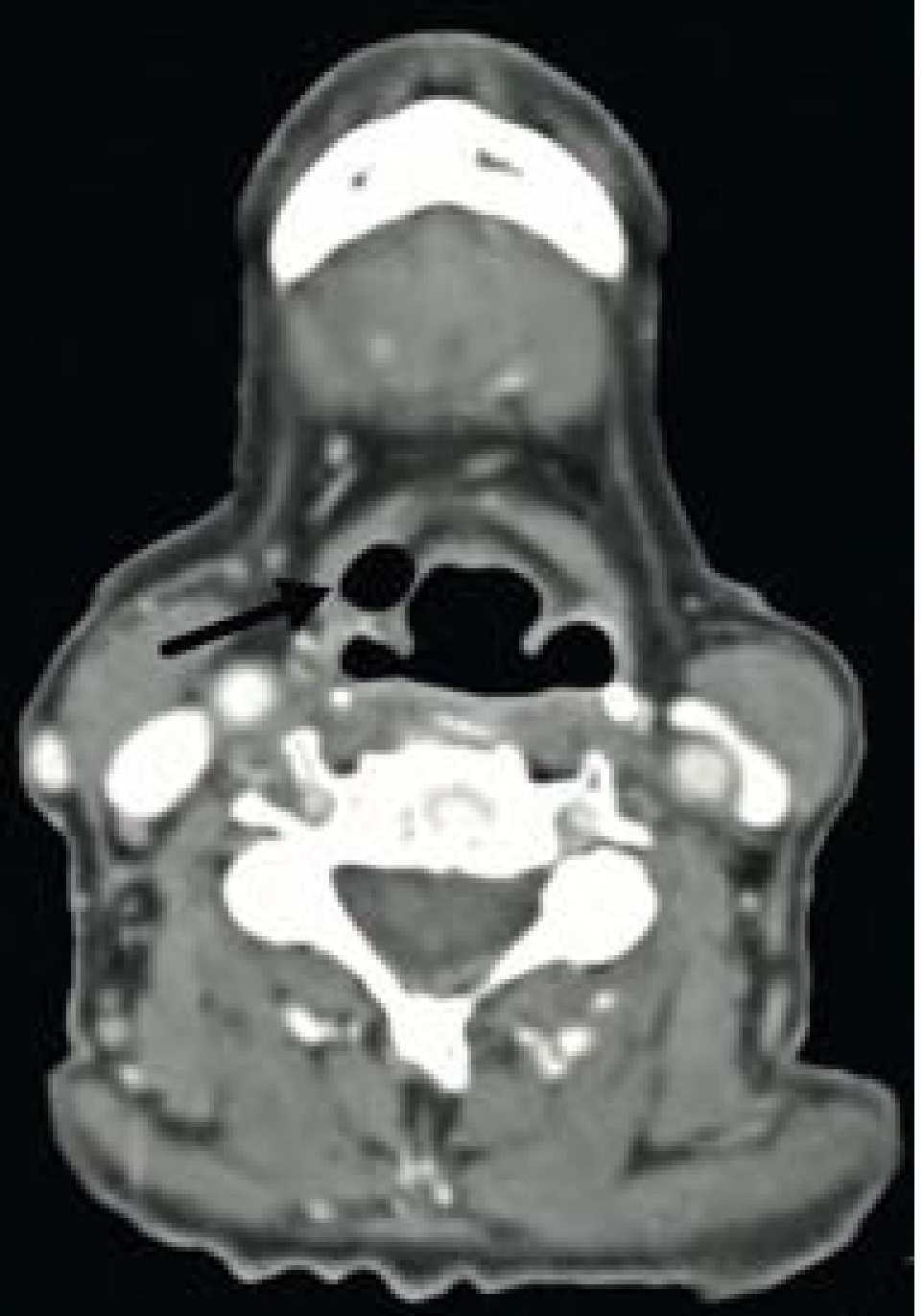
Fig. Internal laryngocele on CT - Cummings Otolaryngology. The air-filled laryngocele (arrow) is in the right paraglottic space, causing mass effect on the right piriform sinus.
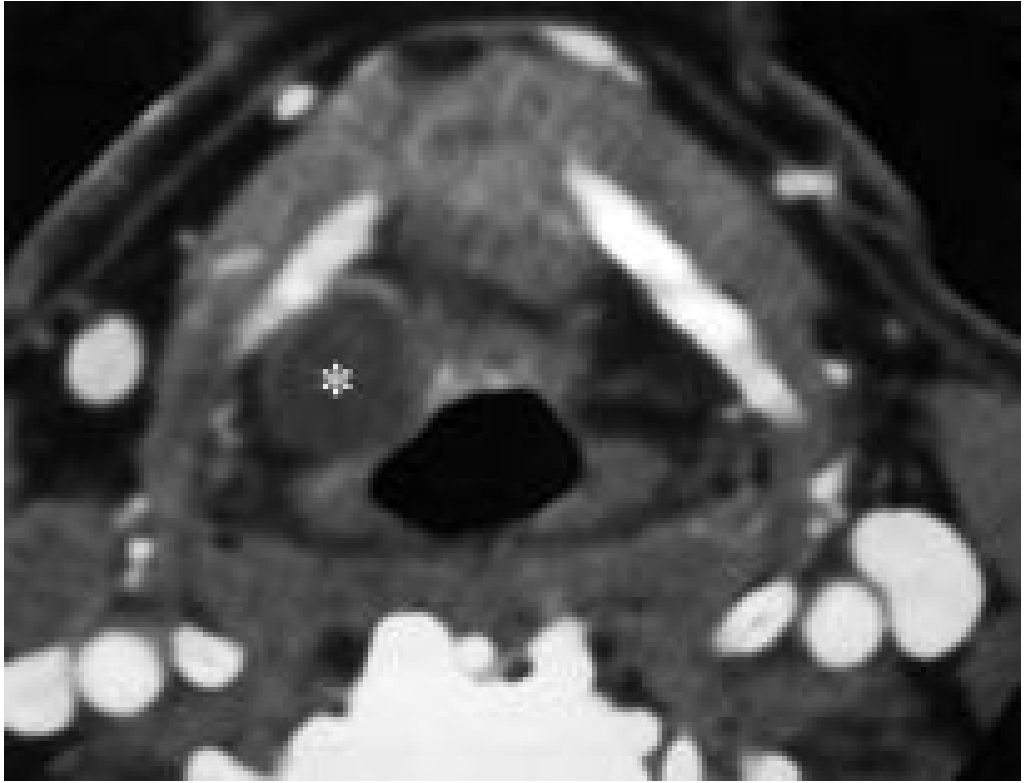
Fig. Fluid-filled laryngocele (asterisk) in the paraglottic fat on enhanced CT - Cummings Otolaryngology.
- Air-filled laryngoceles appear as sharply defined, air-containing structures on CT
- Fluid-filled mucoceles appear as soft tissue density masses; distinction from neoplasm is harder but smooth surface + healthy mucosa on laryngoscopy suggest the diagnosis
- An enhancing wall on CT suggests infection (laryngopyocele)
- A modified Valsalva maneuver during imaging can improve visualization
- CT also demonstrates the external component not apparent on physical examination
MRI: can characterize the lesion; signal varies with degree of proteinaceous debris
Endoscopy
-
Direct laryngoscopy is mandatory to rule out an obstructing laryngeal carcinoma in the ventricle, especially before surgery
-
May appear as a soft, localized bulge of the aryepiglottic fold, potentially mimicking a submucosal neoplasm
-
Cummings Otolaryngology, p. 1127-1130; KJ Lee's Essential Otolaryngology, p. 924
Association with Laryngeal Carcinoma
This is a key clinical point: 5-29% of laryngoceles may harbor an associated ventricular/supraglottic carcinoma that caused saccular obstruction. Therefore, multiple biopsies of the ventricle during endoscopy are strongly recommended before definitive surgery for any laryngocele.
Treatment
Management is surgical for symptomatic lesions.
Infants
- First secure the airway
- Aspiration of cyst contents under direct laryngoscopy, OR
- Endoscopic marsupialization (with or without stripping of cyst lining), optionally using the CO2 laser
- Simple unroofing with cup forceps followed by 3-day intubation as a stent has also been described
Adults - Internal Laryngoceles
- Endoscopic marsupialization or excision (microlaryngoscopy / CO2 laser) - preferred for internal lesions
- Complete endoscopic excision (rather than simple marsupialization) is favored for definitive treatment and lower recurrence, including for large lesions
Adults - External or Combined Laryngoceles
- External (transcervical) approach: the neck component is followed through the thyrohyoid membrane; the sac is transected at the saccular orifice; resection of part of the thyroid cartilage lamina may occasionally be needed for access
- Complete endoscopic excision has also been described for combined lesions by following the cyst wall over the top of the thyroid cartilage into the neck
Key Operative Caveat
A large lateral cyst that bulges dramatically on awake endoscopy can virtually disappear under general anesthesia. The surgeon should begin by excising the false fold, during which the cyst wall is invariably encountered.
- Cummings Otolaryngology, p. 1129-1130; KJ Lee's Essential Otolaryngology, p. 924
Summary Table
| Feature | Detail |
|---|---|
| Origin | Saccule (appendix) of laryngeal ventricle |
| Content | Air (patent orifice) / Mucus (blocked = mucocele) / Pus (blocked = pyocele) |
| Types | Internal / External / Combined |
| Most common type | Combined |
| Bilateral occurrence | ~25% |
| Key symptom | Hoarseness (most common); neck mass increases with Valsalva (external) |
| Bryce sign | Gurgling over neck mass |
| Imaging of choice | CT neck |
| Mandatory workup | Laryngoscopy + biopsy to exclude carcinoma |
| Carcinoma association | 5-29% |
| Treatment | Surgical - endoscopic excision / external approach |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 1127-1130
- KJ Lee's Essential Otolaryngology, p. 924
This is a shared conversation. Sign in to Orris to start your own chat.