Osteomyelitis detailed explanation
Reading File
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative sources. Let me compile the detailed explanation.
Osteomyelitis - Detailed Explanation
Definition
Osteomyelitis is inflammation of bone and marrow, virtually always secondary to infection. It may complicate any systemic infection but frequently presents as a solitary primary focus. All types of organisms - bacteria, viruses, parasites, and fungi - can cause it, but pyogenic bacteria and mycobacteria are by far the most common.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Routes of Infection
Three pathways allow organisms to reach bone:
| Route | Description | Typical Setting |
|---|---|---|
| Hematogenous | Bacteremia seeds bone via the bloodstream | Children (long bone metaphyses), adults (vertebrae) |
| Contiguous spread | Extension from adjacent soft tissues/joints | Diabetic foot, pressure sores |
| Direct implantation | Penetrating trauma, surgery, open fractures | Post-operative, compound fractures |
In children, hematogenous spread is most common. The metaphyses of long bones are preferentially involved because the slow blood flow through looped capillaries, combined with microtrauma, encourages bacterial seeding during a bacteremia. In adults, osteomyelitis is most often a complication of open fractures, surgical procedures, or diabetes (feet).
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Microbiology / Causative Organisms
| Setting | Typical Organism(s) |
|---|---|
| General (all ages) | Staphylococcus aureus (80-90% of culture-positive cases) |
| Neonates | Group B Streptococcus, E. coli |
| Older children | S. aureus, Streptococcus pyogenes, Haemophilus influenzae |
| Sickle cell disease | Salmonella spp., gram-negative organisms |
| IV drug users / elderly | Gram-negatives, polymicrobial |
| Immunocompromised | Fungi (Coccidioides, Blastomyces, Cryptococcus), Mycobacteria |
| Post-surgical / trauma | Mixed bacterial infections |
Why S. aureus? Staphylococcal cell-wall proteins bind bone matrix components such as collagen, facilitating bacterial adherence to bone. MRSA is now the dominant organism in acute hematogenous osteomyelitis (AHO) in many regions.
- Robbins, Cotran & Kumar
Specific organisms are only identified in ~50% of patients on culture; PCR-based assays are expected to improve this rate.
Age-Related Vascular Anatomy (Key Concept)
The site of infection is determined by the osseous vascular anatomy, which changes with age:
- Neonates: Metaphyseal vessels penetrate the growth plate, so infection can spread to both the epiphysis and joint - septic arthritis frequently co-exists.
- Older children (>18 months): The growth plate acts as a barrier; metaphyseal involvement is typical, epiphysis is spared.
- Adults: After growth plate closure, anastomoses form between metaphyseal and epiphyseal vessels - infection tends to involve the epiphyses and subchondral regions. Vertebral osteomyelitis becomes more common.
- Grainger & Allison's Diagnostic Radiology
Pathology: Stages of Disease
Acute Phase (within 48 hours)
- Bacteria proliferate → neutrophilic infiltration
- Bone cell and marrow necrosis within 48 hours
- Bacteria + inflammatory cells spread via Haversian canals to reach the periosteum
- Periosteum (loosely attached in children) is elevated → subperiosteal abscess forms
- Periosteal lifting further impairs cortical blood supply → more necrosis
Subacute / Progressive Phase
- Increased pressure from abscess → pus perforates cortical bone
- Pus elevates the strong periosteum, rendering cortical bone avascular
- Periosteal elevation is a potent stimulus for new bone formation (involucrum)
- Soft tissue abscesses form; may channel to skin as draining sinuses
Chronic Phase
- Dead avascular bone = sequestrum
- New reactive bone forming a shell around the sequestrum = involucrum
- This creates the classic "bone-within-a-bone" appearance on imaging
- Marrow shows fibrosis and a chronic infiltrate of lymphocytes and plasma cells
- Pus may track through gaps (cloacae) in the involucrum to the surface
Brodie Abscess: A walled-off chronic abscess, appearing as a well-defined lytic lesion with a sclerotic rim - characteristic of subacute osteomyelitis.
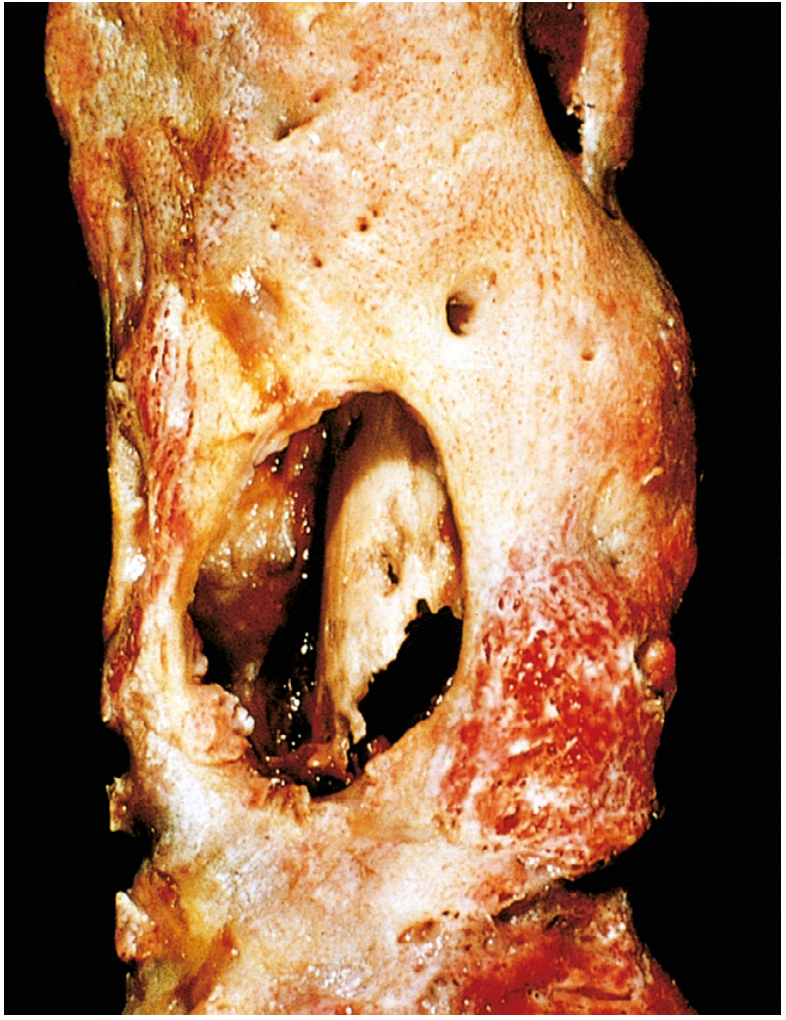
Below is a gross pathology specimen showing chronic osteomyelitis - the outer involucrum (new viable bone shell) has been opened to reveal the inner white sequestrum (necrotic cortex):
Clinical Features
Symptoms
- Fever, rigors, may appear toxic
- Systemic: headache, fatigue, malaise, anorexia (less consistent in chronic disease)
- Children: sudden limp or inability to bear weight, localized warmth, swelling, erythema
Signs
- Point tenderness over the infected segment (most consistent finding)
- Palpable warmth and soft-tissue swelling with erythema
- In chronic disease: palpable involucrum/sequestrum, sinus tracts to skin
- A sympathetic effusion in the adjacent joint may develop even without joint infection
Acute Hematogenous Osteomyelitis (AHO) in Children
- Male preponderance (2:1 to 3:1)
- Involves long bones ~80% of cases
- Distal metaphysis most common site (increased vascularity)
- Blood cultures positive in ~40% of cases
- Rosen's Emergency Medicine
Vertebral Osteomyelitis (Adults)
- Increasingly common as population ages
- Risk factors: IV access devices, indwelling lines, urinary infections, IV drug use
- Presents with back pain, low-grade fever; neurological signs if epidural extension
Investigations
Laboratory
- CBC: Leukocytosis (variable)
- ESR and CRP: Elevated - useful for monitoring response to treatment
- Blood cultures: Positive in ~40% of pediatric AHO; lower in adults
- Bone biopsy + culture: Gold standard for organism identification
- PCR assays: Emerging to improve yield above culture
Imaging
| Modality | Key Points |
|---|---|
| Plain X-ray | Lags behind disease by 10-14 days; shows soft tissue swelling, cortical irregularity, periosteal reaction, lytic destruction |
| Ultrasound | Detects subperiosteal fluid/abscess early; guides drainage; especially useful in children |
| Bone scan (scintigraphy) | Sensitive early; useful for multifocal disease screening; less specific |
| CT | Best for defining extent of cortical destruction, detecting sequestra; higher radiation |
| MRI | Highest sensitivity and specificity; best for early disease, soft tissue involvement, spinal complications, epidural abscess |
MRI features: Bone marrow edema on T1 (low signal) and T2 (high signal); periosteal reaction; soft tissue edema. The penumbra sign in subacute infection = a peripheral high-signal ring of granulation tissue surrounding a low-signal abscess cavity.
Even on appropriate therapy, radiographic signs of improvement lag behind clinical recovery.
- Grainger & Allison's Diagnostic Radiology
Classification
By Duration
- Acute: < 2-4 weeks symptoms; hematogenous; responds to antibiotics alone (often)
- Subacute: Weeks to months; Brodie abscess typical; culture often negative
- Chronic: >4-6 weeks; sequestrum/involucrum/sinus tracts; requires surgery + prolonged antibiotics
Cierny-Mader Classification (Chronic Osteomyelitis)
Used clinically to guide surgical planning:
- Stage 1 (Medullary): Endosteal infection only
- Stage 2 (Superficial): Cortical surface involvement from contiguous source
- Stage 3 (Localized): Full-thickness cortical involvement, stable bone
- Stage 4 (Diffuse): Through-and-through infection, mechanically unstable bone
Host class: A (normal), B (compromised local or systemic), C (treatment worse than disease)
Special Subsets
Diabetic Foot Osteomyelitis
- Contiguous spread from soft tissue ulcers
- Polymicrobial; often includes gram-negatives and anaerobes
- Probe-to-bone test: positive = high specificity for osteomyelitis
- MRI is imaging modality of choice
Vertebral Osteomyelitis (Spondylodiscitis)
- Usually involves two adjacent vertebral bodies + intervening disc
- Most common site: lumbar spine
- Complications: epidural abscess, spinal cord compression, vertebral collapse
- MRI is mandatory to assess intraspinal involvement
Neonatal Osteomyelitis
- Multiple sites in ~50% of cases
- Septic arthritis frequently co-exists (shared vasculature)
- Flat bones (facial bones) more commonly involved than at other ages
- Whole-body MRI or skeletal scintigraphy for multifocal screening
CRMO (Chronic Recurrent Multifocal Osteomyelitis)
- Autoinflammatory (non-infectious) form
- Multiple foci, culture-negative
- Associated with psoriasis subtypes
- Diagnosed by imaging pattern; treated with NSAIDs/bisphosphonates
Treatment
General Principles
- Identify the organism (blood cultures, bone biopsy)
- Start empirical antibiotics, then narrow based on culture
- Drain any pus surgically
- Splint/rest the affected limb
- Treat underlying conditions (sickle cell, nutritional deficiency, diabetes)
Antibiotic Therapy
| Setting | Empirical Choice |
|---|---|
| Children (MSSA suspected) | Anti-staphylococcal penicillin (flucloxacillin) or 1st-gen cephalosporin |
| MRSA suspected (most AHO) | Vancomycin IV; or clindamycin if susceptible |
| Neonates | Vancomycin + cefotaxime (cover GBS + gram-negatives) |
| Adults (vertebral/diabetic) | Vancomycin + broad gram-negative cover until cultures return |
- IV-to-oral switch: Once clinical and laboratory improvement is documented, oral step-down is appropriate in uncomplicated cases. Debate continues on exact duration.
- Total duration typically 4-6 weeks for acute; 3-6 months for vertebral or chronic.
- A 2025 meta-analysis on oritavancin (PMID 41224240) found it effective for osteomyelitis, offering the advantage of once-weekly dosing - relevant for long-course outpatient treatment.
Surgical Treatment
- Indication: Abscess formation, failure of medical treatment, chronic osteomyelitis with sequestrum, sinus tracts, unstable bone
- Procedures: Debridement, sequestrectomy, saucerization, dead space management (antibiotic-impregnated beads, bone grafting, muscle flaps), stabilization if unstable
- Shortened IV and oral regimens apply only to uncomplicated cases in patients who are clinically and hematologically improving.
- Bailey and Love's Short Practice of Surgery
Complications
| Complication | Notes |
|---|---|
| Chronic osteomyelitis | Occurs in 5-25% of acute cases; delayed diagnosis, extensive necrosis are risk factors |
| Septic arthritis | Especially neonates and when metaphysis is intracapsular |
| Bacteremia / Sepsis | Systemic spread of infection |
| Growth disturbance | Physeal damage in children → limb shortening or deformity |
| Pathologic fracture | Through sites of bone destruction |
| Secondary amyloidosis | Complication of long-standing chronic infection |
| Squamous cell carcinoma | Malignant transformation in chronic draining sinus tracts (rare, late) |
| Sarcoma | Rare malignant transformation in infected bone |
| Brain abscess / meningitis | Hematogenous spread from vertebral/skull osteomyelitis |
| Spinal cord compression | Epidural extension in vertebral osteomyelitis |
Mycobacterial Osteomyelitis (Skeletal TB)
- More destructive and resistant than pyogenic osteomyelitis
- Occurs in ~1-3% of individuals with pulmonary or extrapulmonary TB
- Typically solitary, insidious onset; years may pass before diagnosis
- Classic site: spine (Pott's disease) - involves two adjacent vertebrae + disc
- Spina ventosa: TB dactylitis - cyst-like cavities with diaphyseal expansion, predominantly in hand/foot bones
- Treatment: standard anti-TB regimen (minimum 9-12 months)
- Robbins, Cotran & Kumar
Key Terms Summary
| Term | Meaning |
|---|---|
| Sequestrum | Fragment of dead, avascular necrotic bone |
| Involucrum | Shell of new periosteal bone surrounding the sequestrum |
| Cloaca | Gap/opening in the involucrum through which pus drains |
| Brodie abscess | Walled-off subacute abscess with sclerotic rim on imaging |
| Sinus tract | Channel from the infected bone to the skin surface |
| Penumbra sign | MRI finding in subacute osteomyelitis - high-signal granulation tissue rim around abscess |
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, Ch. 26
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 44
- Rosen's Emergency Medicine, Ch. 125
- Grainger & Allison's Diagnostic Radiology, Ch. 73
- Recent evidence: Systematic review on chronic pediatric osteomyelitis (PMID 41329650, 2025); Meta-analysis on oritavancin for osteomyelitis (PMID 41224240, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.