Vetebral artery course
Reading File
Finding Sources
Searching the Web
vertebral artery course anatomy segments
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a detailed breakdown of the vertebral artery course, compiled from Gray's Anatomy for Students, Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22E, and Localization in Clinical Neurology.
Vertebral Artery - Course and Segments
Origin
The vertebral artery is the first and largest branch of the first part of the subclavian artery, arising medial to the anterior scalene muscle in the root of the neck. Occasionally it may arise directly from the aortic arch or thyrocervical trunk (anatomical variant).
Four Segments (V1-V4)
V1 - Preforaminal Segment
- Extends from the origin at the subclavian artery to its entry into the transverse foramen of C6 (occasionally C4, C5, or C7)
- Courses superiorly and posteriorly, passing between the longus colli (medially) and anterior scalene muscle (laterally)
- Lies posterior to the internal carotid artery and anterior to the roots of CN XII (hypoglossal nerve)
- Most susceptible to atherosclerosis - ~20-40% of cerebrovascular disease involves this segment
- Goldman-Cecil Medicine, p. 3921
V2 - Foraminal (Transverse/Cervical) Segment
- Passes through the transverse foramina of C6 to C2, ascending through successive foramina
- Accompanied by a venous plexus and sympathetic nerve fibers
- Rarely narrowed by atherosclerosis, but susceptible to dissection, fibromuscular dysplasia, and osteophytic spur compression
- Harrison's Principles 22E
V3 - Extradural (Atlantic/Suboccipital) Segment
- From exit of the C2 transverse foramen to penetration of the dura at the foramen magnum
- Exits C1 transverse foramen, curves posteriorly and medially in the suboccipital triangle, looping around the lateral mass of the atlas (C1)
- Crosses the posterior arch of C1, passes through the posterior atlanto-occipital membrane
- Issues muscular branches that anastomose with the ascending cervical and deep cervical arteries
- Most vulnerable to mechanical injury and dissection due to its mobility at this level
- Goldman-Cecil Medicine, p. 3921; Gray's Anatomy for Students
V4 - Intradural (Intracranial) Segment
- Pierces the dura and arachnoid at the foramen magnum and enters the posterior cranial fossa
- Ascends anterior to the medulla, passing anterior to the roots of CN XII
- At the pontomedullary junction, it joins its contralateral counterpart to form the basilar artery
- In some individuals, one vertebral artery ends as the PICA (posterior inferior cerebellar artery) rather than contributing to the basilar artery
- Only the V4 segment gives rise to branches supplying the brainstem and cerebellum
- Harrison's Principles 22E; Goldman-Cecil Medicine
Major Branches (from V4)
| Branch | Supply |
|---|---|
| Posterior inferior cerebellar artery (PICA) | Lateral medulla (proximal segment), inferior surface of cerebellum, vestibular nuclei |
| Anterior spinal artery | Formed by union of medial branches from both vertebral arteries; supplies anterior 2/3 of spinal cord |
| Posterior spinal artery | Posterior cord (may arise from PICA) |
| Medullary penetrating branches | Medullary pyramid, inferior olivary nucleus, medial lemniscus, CN XII fibers |
| Longer circumferential branches | Spinothalamic tracts, sympathetic fibers, sensory nuclei and descending CN V tracts, CN IX and X fibers |
| Meningeal branch | Arises as artery enters foramen magnum; supplies posterior fossa dura |
Termination
Both vertebral arteries join at the lower border of the pons (pontomedullary junction) to form the single midline basilar artery, which continues as the dominant vessel of the posterior circulation.
Circle of Willis - MR Angiogram
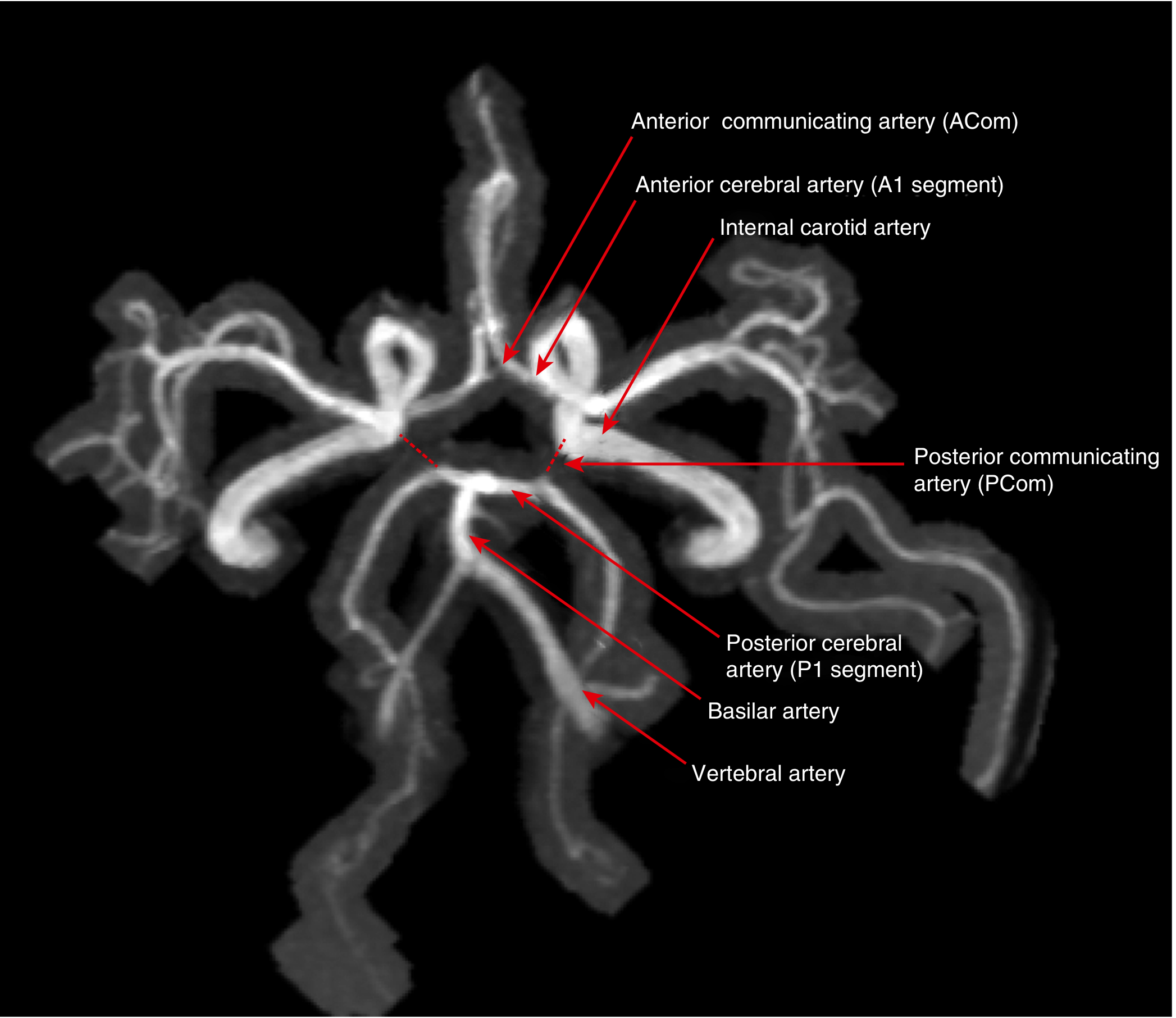
MR angiogram of the circle of Willis showing vertebral artery, basilar artery, posterior cerebral artery (P1 segment), and their connections - Goldman-Cecil Medicine
Key Clinical Points
- Subclavian steal syndrome: Subclavian artery occlusion proximal to the vertebral origin reverses blood flow in the ipsilateral vertebral artery; arm exercise may "steal" posterior circulation flow, causing brainstem TIAs
- V3 dissection: This segment is most vulnerable to mechanical injury (chiropractic manipulation, trauma, hyperextension)
- V4 occlusion - causes Wallenberg's (lateral medullary) syndrome: vertigo, ipsilateral facial numbness, contralateral limb numbness, dysarthria, dysphagia, hoarseness, ipsilateral Horner's syndrome - Harrison's 22E
- Vertebral artery hypoplasia: Asymmetry is common; the ipsilateral transverse foramina will appear smaller on imaging
- Atherosclerosis preferentially affects V1 and V4 segments
- Fractures of the upper six cervical vertebrae transverse processes can injure the V2 segment
This is a shared conversation. Sign in to Orris to start your own chat.