Causes of raised alkaline phosphatase
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-structured answer.
Causes of Raised Alkaline Phosphatase (ALP)
ALP is present in multiple tissues — liver (canalicular membrane of hepatocytes), bone (osteoblasts), placenta, small intestine, and kidneys. A rise therefore may reflect hepatobiliary, osseous, or physiological sources. Confirming the origin is the first step: a concomitantly elevated GGT or 5'-nucleotidase points to a hepatic/biliary source; if both are normal, bone is the likely source.
Physiological (Non-Pathological) Causes
| Cause | Mechanism |
|---|---|
| Childhood / adolescence | Rapid bone growth elevates bone isoenzyme; levels may be twice the adult upper limit |
| Pregnancy (late) | Influx of placental ALP isoenzyme |
| Age >60 | Mild elevation (1–1.5× normal) in healthy older individuals |
| Post-fatty meal | Intestinal ALP released, particularly in blood group O and B Lewis-positive secretors; can rise 30% for up to 12 hours |
| Perimenopausal women | Values rise toward male reference range |
Hepatobiliary Causes
Cholestatic / Obstructive (typically >4× normal)
- Extrahepatic biliary obstruction — gallstones (choledocholithiasis), cholangiocarcinoma, pancreatic cancer, bile duct stricture
- Primary biliary cholangitis (PBC) — antimitochondrial antibody (AMA) positive; often the predominant liver test abnormality
- Primary sclerosing cholangitis (PSC) — especially in patients with IBD
- Secondary sclerosing cholangitis
- Ascending cholangitis
- Drug-induced cholestasis — e.g., amoxicillin-clavulanic acid, chlorpromazine, erythromycin, trimethoprim-sulfamethoxazole, nitrofurantoin, oral contraceptives
Infiltrative / Space-Occupying Liver Disease
ALP is the most sensitive marker of hepatic metastases among routine liver chemistry tests.
- Hepatic metastases (any primary)
- Primary hepatocellular carcinoma
- Hepatic granulomas — sarcoidosis, tuberculosis, fungal infections, brucellosis
- Amyloidosis
- Langerhans cell histiocytosis
- Extramedullary haematopoiesis
Other Hepatic
- Virtually any liver disease can produce mild elevation (<3×); this is not specific for cholestasis
- Cirrhosis — intestinal isoenzyme frequently elevated (>80% of cirrhotics)
- Passive congestion of the liver (right heart failure / congestive cardiac failure)
- Sepsis (intrahepatic cholestasis of sepsis)
- AIDS cholangiopathy (CMV, cryptosporidial infection)
- Diabetic hepatosclerosis — raised ALP with near-normal aminotransferases
- Liver transplant rejection
- Hodgkin's lymphoma (hepatic involvement)
- Hyperthyroidism (increased bone turnover may contribute)
Bone Causes (GGT normal; ALP fractionation shows bone isoenzyme)
| Condition | Notes |
|---|---|
| Paget's disease of bone | One of the most common causes of markedly raised ALP in adults; can exceed 10× normal |
| Osteomalacia / rickets | Increased osteoblastic activity trying to mineralise |
| Healing fractures | Transient rise |
| Bone metastases (osteoblastic) | Prostate, breast |
| Primary bone tumours | Osteosarcoma |
| Hyperparathyroidism | Increased bone resorption and remodelling |
| Hyperthyroidism | Accelerated bone turnover |
| Renal osteodystrophy | Secondary hyperparathyroidism → increased osteoblast activity |
| Acromegaly | Increased bone turnover |
Other / Miscellaneous
- Diabetes mellitus (mild elevation)
- Congestive cardiac failure (hepatic congestion)
- Lymphoma (Hodgkin's disease particularly)
- Secondary syphilis (hepatic involvement)
- Peritoneal candidiasis (persistent elevated ALP with constitutional symptoms)
Causes of Low ALP (for completeness)
- Hypophosphatasia — inborn deficiency of the enzyme; pathognomonic low ALP
- Wilson's disease — copper displaces cofactor zinc, reducing enzyme activity (especially in acute liver failure)
- Malnutrition / hypothyroidism
- Theophylline, oestrogen therapy
- Haemolysis — can falsely lower the result
Diagnostic Approach
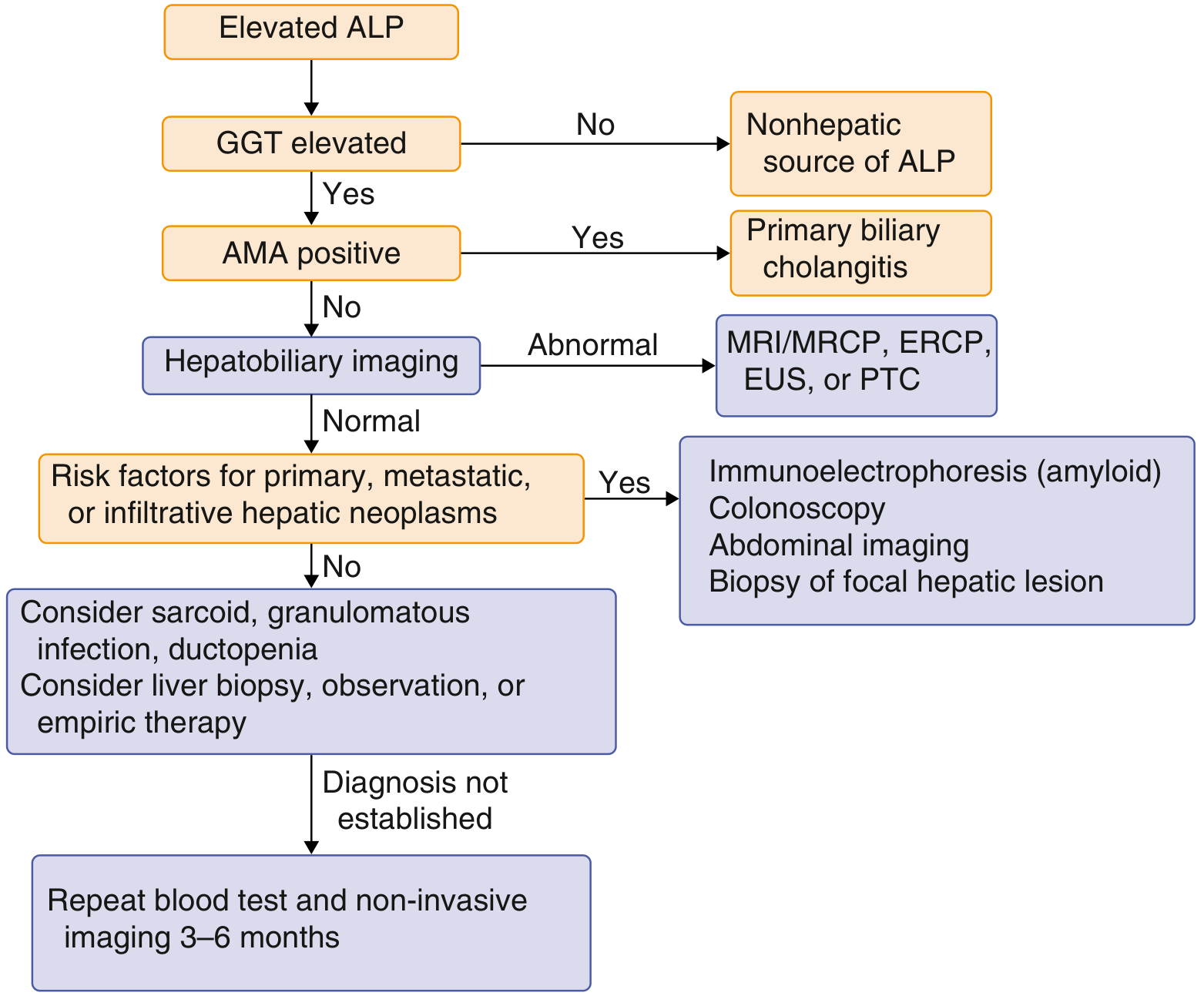
Diagnostic flowchart for elevated ALP: GGT elevation confirms hepatobiliary source → AMA for PBC → imaging for biliary/infiltrative disease — Goldman-Cecil Medicine
Key steps:
- GGT/5'-nucleotidase elevated? → Hepatobiliary source confirmed → liver ultrasound
- GGT normal? → Non-hepatic source (bone, placenta, intestine) likely
- AMA positive? → Primary biliary cholangitis
- Imaging abnormal? → MRCP/ERCP for biliary tree
- Infiltrative disease suspected? → Colonoscopy, immunoelectrophoresis (amyloid), consider liver biopsy
- No diagnosis after above? → Consider sarcoid, granulomatous infection, ductopenia; repeat in 3–6 months
Sources: Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine; Sleisenger & Fordtran's GI and Liver Disease; Washington Manual of Medical Therapeutics; Quick Compendium of Clinical Pathology 5e; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.