Grade 1 2percent burn management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"first degree burn" OR "superficial burn" treatment management
I now have comprehensive information to provide a thorough answer. Here is the management of a Grade 1 (First-Degree), ~2% TBSA Burn:
Grade 1 (First-Degree) Burn — 2% TBSA: Management
Definition & Pathology
A first-degree (superficial/epidermal) burn involves only the epidermis — no dermal injury, no blistering. Classic example: sunburn.
| Feature | First-Degree Burn |
|---|---|
| Depth | Epidermis only |
| Appearance | Erythematous, red, dry — no blisters |
| Sensation | Painful and tender |
| Healing | ~7 days, no scarring |
| Included in TBSA? | No — first-degree burns are excluded from TBSA calculations |
Classification by Severity
A 2% first-degree burn falls firmly into the minor burn category:
| Class | Criteria | Disposition |
|---|---|---|
| Minor | Partial-thickness <15% BSA (age 10–50 y); Full-thickness <2% | Outpatient |
| Moderate | Partial-thickness 15–25% BSA | Hospitalization |
| Major | >25% BSA or special site / special type | Burn center |
A pure first-degree 2% burn requires no hospitalization and no burn center referral.
Acute Management
1. First Aid (Immediate)
- Cool the burn promptly with cold tap water or ice water and continue until pain does not return on stopping — this reduces heat propagation and provides analgesia.
- Do not apply ice directly (risk of frostbite on damaged skin).
- Remove clothing and jewelry from the burned area.
2. Wound Care
- First-degree burns require only symptomatic / local treatment — no dressings are mandatory.
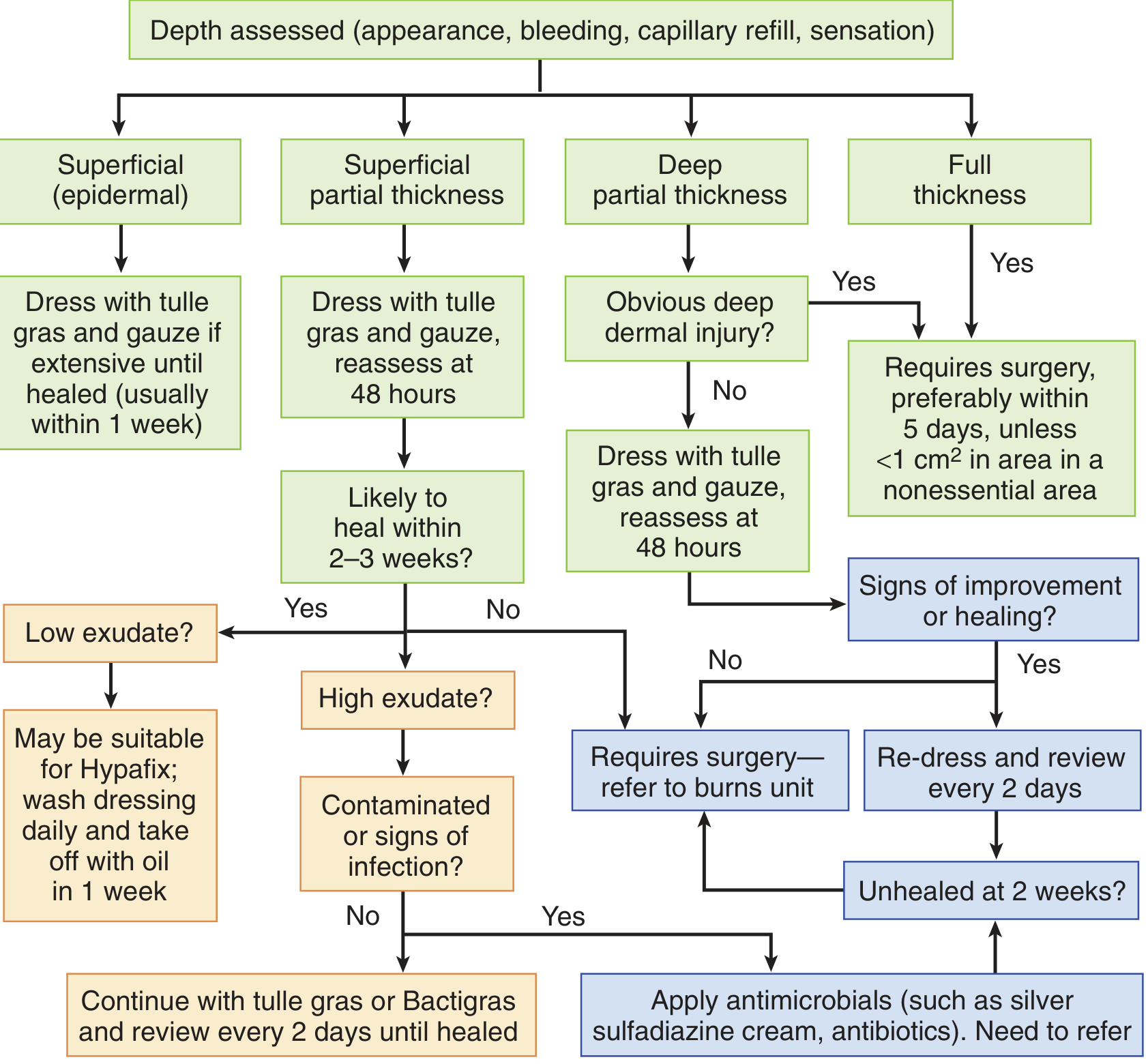
- If the burn is extensive (even for 1°), a light non-adherent (paraffin/tulle gras) dressing with gauze may be applied until healed (usually within 1 week).
- No debridement needed — no blistering is present.
- Keep the area clean; gentle washing with mild soap and water is appropriate.
3. Topical Agents
- Emollients / moisturizers (e.g., aloe vera gel, petroleum jelly) soothe the skin and reduce pain and dryness.
- Greasy gauze (paraffin gauze / Vaseline gauze) can be used for symptomatic comfort on larger superficial burns.
- Silver-containing dressings and topical antibiotics (e.g., silver sulfadiazine) are not indicated for pure first-degree burns — these are reserved for partial-thickness (2nd-degree) wounds.
- No prophylactic antibiotics are needed.
4. Pain Control
- Oral NSAIDs (ibuprofen) or acetaminophen (paracetamol) are the mainstay — adequate for first-degree burn pain.
- Topical cool compresses provide additional symptomatic relief.
- Opioids are not indicated.
5. Sun Protection
- Protect the healing area from further UV exposure; use sunscreen once re-epithelialized.
Burn Depth Assessment Algorithm
What to Monitor / When to Escalate
| Red Flag | Action |
|---|---|
| Wound not healed by 7–10 days | Re-evaluate — may be deeper than initially assessed |
| Signs of infection (increased erythema, warmth, purulent exudate, fever) | Wound culture; consider topical/systemic antibiotics; refer |
| Involvement of face, hands, feet, genitalia, perineum, or major joints | Burn center referral even for smaller burns |
| Patient age <10 or >50 with larger burns | Lower threshold for referral |
Key Points Summary
- First-degree burns are excluded from TBSA calculations — the "2%" does not change fluid resuscitation thresholds (which apply to partial/full-thickness burns).
- No IV fluids needed — resuscitation formulas (Parkland, Brooke) apply only to second- and third-degree burns.
- No surgical intervention — no grafting, no debridement.
- Heals spontaneously in ~7 days with minimal to no scarring.
- Treatment is entirely outpatient and symptomatic: cooling, emollients, analgesia, light dressing if needed.
Sources: Tintinalli's Emergency Medicine (9e), Current Surgical Therapy (14e), Schwartz's Principles of Surgery (11e), Andrews' Diseases of the Skin, Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.