Renal physiology mbbs 1st yr
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from the textbooks. Let me now compose the complete, detailed MBBS 1st year renal physiology notes.
Renal Physiology - MBBS 1st Year Complete Notes
Sources: Guyton & Hall Textbook of Medical Physiology, Ganong's Review of Medical Physiology (26th Ed.)
1. FUNCTIONS OF THE KIDNEYS
The kidneys serve multiple homeostatic roles beyond just excretion:
| Function | Details |
|---|---|
| Excretion of waste | Urea (amino acid metabolism), creatinine (muscle creatine), uric acid (nucleic acids), bilirubin metabolites |
| Fluid & electrolyte balance | Precisely matches excretion to intake over time |
| Osmolality regulation | Produces hypertonic or hypotonic urine as needed |
| Acid-base balance | Excretes H⁺, reabsorbs HCO₃⁻ |
| Blood pressure regulation | Renin-angiotensin-aldosterone system (RAAS), pressure natriuresis |
| Erythropoiesis | Secretes erythropoietin (EPO) in response to hypoxia |
| Hormone metabolism | Activates Vitamin D (1,25-DHCC); metabolises/excretes hormone metabolites |
| Gluconeogenesis | Especially during prolonged fasting |
- Guyton & Hall, p. 3125-3148
2. FUNCTIONAL ANATOMY OF THE NEPHRON
Gross Structure
Each kidney has approximately 1 million nephrons. The nephron is the functional unit, consisting of a renal corpuscle (glomerulus + Bowman's capsule) and a renal tubule.
Types of Nephrons
| Type | Location | Loop of Henle | Function |
|---|---|---|---|
| Cortical nephrons (~85%) | Cortex | Short loop, stays in cortex | General filtration |
| Juxtamedullary nephrons (~15%) | Cortex-medulla junction | Long loop, dips into medulla | Urine concentration |
Nephron Segments (in order)
- Glomerulus - filtration
- Bowman's capsule - collects filtrate
- Proximal convoluted tubule (PCT) - bulk reabsorption
- Loop of Henle - descending (thin) + ascending (thin + thick)
- Distal convoluted tubule (DCT) - regulated reabsorption
- Collecting duct (CD) - final concentration/dilution
Blood Supply
-
Afferent arteriole → glomerular capillaries → efferent arteriole → peritubular capillaries (cortical nephrons) or vasa recta (juxtamedullary nephrons)
-
Unique feature: two capillary beds in series - glomerular capillaries (high pressure, for filtration) and peritubular capillaries (low pressure, for reabsorption)
-
Ganong's, p. 671-672
3. GLOMERULAR FILTRATION
What is GFR?
GFR = volume of plasma ultrafiltrate formed per minute. Normal = 125 mL/min (180 L/day). Of this, ~178.5 L is reabsorbed; only ~1.5 L/day is excreted as urine.
Filtration Barrier (Glomerular Membrane)
Three layers prevent passage of large proteins and cells:
- Fenestrated endothelium - prevents passage of RBCs and platelets
- Glomerular basement membrane (GBM) - negatively charged; repels anionic proteins (e.g., albumin)
- Podocyte foot processes with slit diaphragms - final filtration barrier
Freely filtered: water, electrolytes, glucose, urea, creatinine, small molecules
Not filtered: plasma proteins, blood cells
Starling Forces Governing GFR
GFR = Kf × (PG - PB - πG + πB)
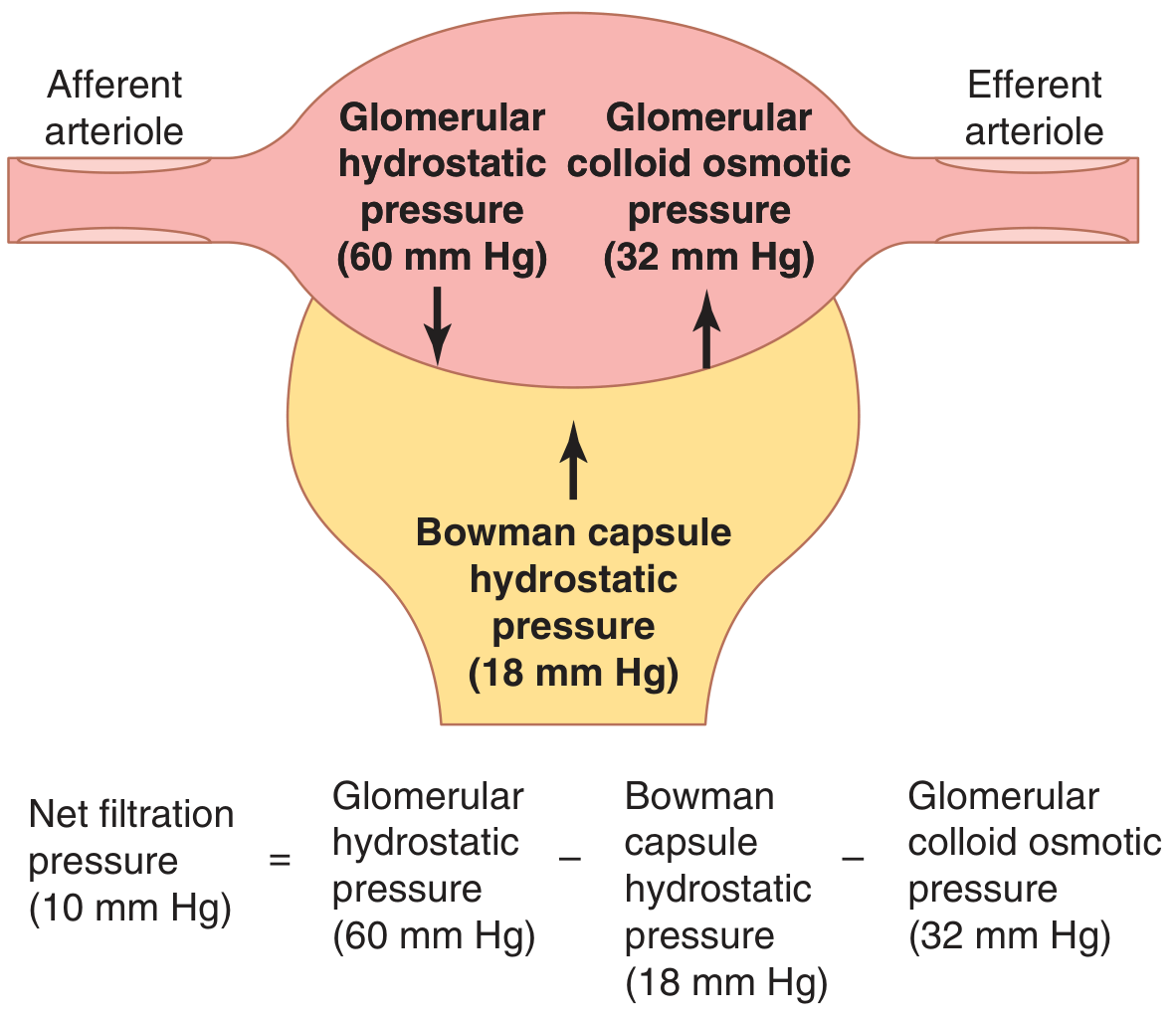
Starling forces at the glomerular capillary (Guyton & Hall, Fig. 27.5)
| Force | Value (mm Hg) | Direction |
|---|---|---|
| Glomerular hydrostatic pressure (PG) | 60 | Favors filtration |
| Bowman's capsule hydrostatic pressure (PB) | 18 | Opposes filtration |
| Glomerular colloid osmotic pressure (πG) | 32 | Opposes filtration |
| Bowman's capsule COP (πB) | ~0 | Favors filtration |
| Net filtration pressure | +10 |
- Kf (filtration coefficient) = ~12.5 mL/min/mm Hg (400x higher than other capillaries)
- Guyton & Hall, p. 3567-3596
Factors Increasing/Decreasing GFR
| Increase GFR | Decrease GFR |
|---|---|
| ↑ Afferent arteriole dilation | ↑ Afferent arteriole constriction |
| ↓ Efferent arteriole constriction (mild) | ↑ Efferent arteriole dilation |
| ↑ Blood pressure (within limits) | ↑ Bowman's capsule pressure (obstruction) |
| ↑ Kf (↑ surface area) | ↑ Plasma proteins (↑ πG) |
4. RENAL AUTOREGULATION
The kidneys maintain relatively constant GFR and renal blood flow despite changes in arterial pressure from ~70 to 210 mm Hg.
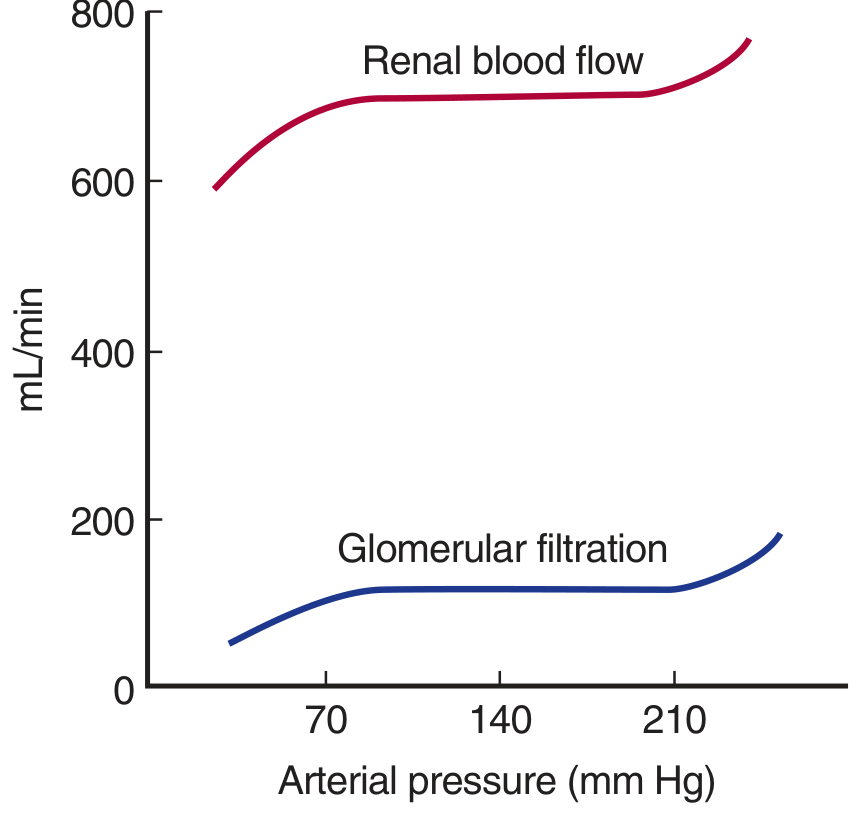
Autoregulation of renal blood flow and GFR (Ganong's, Fig. 37-4)
Mechanisms:
- Myogenic mechanism - stretch of afferent arteriole smooth muscle → vasoconstriction
- Tubuloglomerular feedback (TGF) - macula densa senses ↑ NaCl delivery → adenosine release → afferent arteriole vasoconstriction → ↓ GFR
Juxtaglomerular Apparatus (JGA)
-
Macula densa: specialized cells of thick ascending limb; NaCl sensor
-
Juxtaglomerular (JG) cells: in afferent arteriole wall; secrete renin
-
Extraglomerular mesangial cells (Lacis cells): communication between macula densa and JG cells
-
Ganong's, p. 1644-1665
5. MEASUREMENT OF GFR - RENAL CLEARANCE
Clearance formula:
C = (U × V) / P
Where: C = clearance (mL/min), U = urine concentration, V = urine flow rate (mL/min), P = plasma concentration
Ideal Marker for GFR Measurement
Must be:
- Freely filtered (not bound to protein)
- NOT reabsorbed
- NOT secreted
- Non-toxic, not metabolized
Inulin Clearance (Gold standard)
- Polymer of fructose (MW ~5,200)
- Cinulin = GFR = ~125 mL/min
- Requires IV infusion; not practical clinically
Creatinine Clearance (Clinical use)
- Endogenous product of muscle creatine metabolism
- Freely filtered, not reabsorbed, slightly secreted → slightly overestimates GFR (~10%)
- Normal: ~125 mL/min (males), ~110 mL/min (females)
- Used to estimate GFR in clinical practice
Para-aminohippuric acid (PAH) Clearance
-
Measures Effective Renal Plasma Flow (ERPF)
-
Almost completely cleared in one pass (filtered + secreted)
-
CPAH ≈ ERPF = ~625 mL/min
-
Renal blood flow (RBF) = ERPF / (1 - hematocrit) ≈ 1,200 mL/min
-
Filtration fraction (FF) = GFR/ERPF = 125/625 = ~0.2 (20%)
-
Ganong's, p. 1404-1641
6. TUBULAR REABSORPTION AND SECRETION
Overview
| Segment | Key Function |
|---|---|
| PCT | Bulk reabsorption (65-70% of Na⁺, water, HCO₃⁻, glucose, amino acids) |
| Thin descending Loop of Henle | Water reabsorption (osmotic) |
| Thick ascending Loop of Henle | Na⁺-K⁺-2Cl⁻ cotransport (impermeable to water - "diluting segment") |
| DCT | Na⁺ reabsorption (via NCC cotransporter); regulated |
| Collecting duct | Final adjustment of Na⁺, K⁺, water; ADH and aldosterone action |
Proximal Convoluted Tubule (PCT)
- Reabsorbs ~65% of filtered Na⁺, Cl⁻, water, K⁺, HCO₃⁻
- 100% glucose and amino acids reabsorbed (by secondary active transport - Na⁺-glucose cotransporter, SGLT)
- Tm (transport maximum): maximum rate of tubular reabsorption
- Glucose Tm = ~375 mg/min; renal threshold = ~180-200 mg/dL plasma glucose
- Above threshold → glucosuria
- Isoosmotic reabsorption (fluid remains isotonic)
- Na⁺/H⁺ exchanger at apical membrane; Na⁺-K⁺-ATPase at basolateral membrane
Loop of Henle
- Thin descending limb: permeable to water, NOT to solutes → fluid becomes hyperosmotic
- Thick ascending limb: Na⁺-K⁺-2Cl⁻ (NKCC2) cotransporter; impermeable to water → dilutes the tubular fluid
- Counter-current multiplier creates hyperosmotic medullary interstitium (up to 1200 mOsm/kg)
- Loop diuretics (furosemide) block NKCC2 → prevent concentration, cause diuresis
Distal Convoluted Tubule (DCT)
- NaCl cotransporter (NCC) reabsorbs Na⁺ and Cl⁻
- Thiazide diuretics block NCC
- Ca²⁺ reabsorption stimulated by PTH
Collecting Duct
-
Two cell types:
- Principal cells: Na⁺ reabsorption via ENaC (aldosterone-sensitive), K⁺ secretion
- Intercalated cells (Type A): H⁺ secretion; HCO₃⁻ reabsorption (acid excretion)
-
ADH (vasopressin): inserts aquaporin-2 (AQP2) into apical membrane → water reabsorption → concentrated urine
-
Ganong's, p. 1885-1912
7. REGULATION OF WATER EXCRETION - CONCENTRATION/DILUTION OF URINE
Countercurrent Mechanism
The medullary osmotic gradient (300-1200 mOsm/kg, cortex to papilla) is essential for producing concentrated urine.
Countercurrent Multiplier (Loop of Henle):
- Thick ascending limb actively pumps NaCl into interstitium (without water)
- Creates progressively higher osmolality in medulla
- Thin descending limb equilibrates with hyperosmotic interstitium (loses water)
Countercurrent Exchanger (Vasa Recta):
- Hairpin capillaries of juxtamedullary nephrons run parallel to Loop of Henle
- Preserve medullary osmotic gradient by equilibrating without washing it out
Role of ADH (Vasopressin)
- Released from posterior pituitary when plasma osmolality rises (>285 mOsm/kg) or when volume depletes
- Binds V2 receptor → cAMP → PKA → inserts AQP2 water channels into collecting duct apical membrane
- Water moves from tubular lumen into hyperosmotic interstitium → concentrated urine (max ~1200 mOsm/kg)
- Without ADH: dilute urine (~50-100 mOsm/kg)
| State | ADH | Urine |
|---|---|---|
| Dehydration | ↑↑ | Hyperosmotic (max ~1200 mOsm) |
| Water overload | ↓↓ | Hypo-osmotic (min ~50 mOsm) |
| Diabetes insipidus | Absent/ineffective | Large volumes, dilute urine |
- Ganong's, p. 1896-1908
8. REGULATION OF Na⁺ AND EXTRACELLULAR FLUID VOLUME
Renin-Angiotensin-Aldosterone System (RAAS)
- ↓ BP / ↓ NaCl at macula densa / ↑ sympathetics → Renin release from JG cells
- Renin cleaves angiotensinogen → Angiotensin I
- ACE (lung) converts Ang I → Angiotensin II
- Ang II effects:
- Stimulates aldosterone from adrenal cortex → Na⁺ retention, K⁺ excretion (collecting duct)
- Efferent arteriole constriction → maintains GFR at low BP
- ADH release → water retention
- Thirst stimulation
- Na⁺/H⁺ exchange in PCT
Aldosterone
- Steroid hormone from zona glomerulosa
- Acts on collecting duct principal cells
- Activates sgk (serum/glucocorticoid kinase) → ↑ ENaC (epithelial Na channels) at apical membrane
- Net effect: ↑ Na⁺ reabsorption, ↑ K⁺ secretion, ↑ H⁺ secretion
Atrial Natriuretic Peptide (ANP)
-
Released from atria when volume/pressure increases
-
Causes natriuresis (↑ Na⁺ excretion) and diuresis
-
Inhibits RAAS; dilates afferent arteriole, constricts efferent → ↑ GFR
-
Ganong's, p. 1888-1895
9. POTASSIUM REGULATION
-
Most filtered K⁺ is reabsorbed in PCT (65-70%) and thick ascending limb
-
K⁺ is secreted by principal cells of collecting duct
-
Factors ↑ K⁺ secretion: aldosterone, ↑ tubular flow, metabolic alkalosis, ↑ plasma K⁺
-
Factors ↓ K⁺ secretion: acidosis (H⁺ competes with K⁺)
-
Ganong's, p. 1909-1912
10. ACID-BASE REGULATION BY KIDNEYS
| Mechanism | Site | Details |
|---|---|---|
| HCO₃⁻ reabsorption | PCT (80-85%) | H⁺ secreted via Na⁺/H⁺ exchanger; H⁺ + HCO₃⁻ → H₂CO₃ → CO₂ + H₂O (carbonic anhydrase) |
| Titratable acid excretion | Distal tubule/collecting duct | H⁺ + HPO₄²⁻ → H₂PO₄⁻ (buffers H⁺ in urine) |
| Ammonium excretion | PCT + collecting duct | NH₃ + H⁺ → NH₄⁺; main buffer for H⁺ in acidosis |
11. MICTURITION (URINATION) REFLEX
Anatomy of the Bladder
- Detrusor muscle: smooth muscle; contracts to expel urine (40-60 mm Hg)
- Trigone: triangular area between 2 ureteral orifices and internal urethral orifice
- Internal sphincter: smooth muscle (involuntary) - tonic contraction keeps bladder closed
- External sphincter: skeletal muscle (voluntary) - conscious control of urination
Innervation
| Nerve | Spinal Level | Function |
|---|---|---|
| Pelvic nerves (parasympathetic) | S2-S4 | Detrusor contraction, urination |
| Pudendal nerve (somatic) | S2-S4 | External sphincter control |
| Hypogastric nerve (sympathetic) | L1-L2 | Relaxes detrusor, contracts internal sphincter → storage |
Micturition Reflex
- Bladder fills → stretch receptors activate
- Afferent signals via pelvic nerves → sacral micturition center (S2-S4)
- Efferent parasympathetic signals → detrusor contraction + internal sphincter relaxation
- Voluntary relaxation of external sphincter → voiding
- Higher centers (pontine micturition center, cortex) can inhibit or facilitate the reflex
Cystometrogram
-
Bladder pressure vs. volume graph
-
First urge at ~150 mL; strong desire at ~300-400 mL; max capacity ~600 mL
-
Intravesical pressure remains low (5-15 cm H₂O) until near capacity due to detrusor plasticity
-
Guyton & Hall, p. 3324-3373
12. DIURETICS (Overview for 1st Year)
| Class | Site of Action | Mechanism | Example |
|---|---|---|---|
| Osmotic | PCT, descending loop | ↑ Osmolarity → ↓ water reabsorption | Mannitol |
| Carbonic anhydrase inhibitors | PCT | Blocks CA → ↓ H⁺ secretion → ↓ HCO₃⁻ reabsorption → ↑ NaHCO₃ excretion | Acetazolamide |
| Loop diuretics | Thick ascending limb | Block NKCC2 → ↓ NaCl reabsorption, ↓ medullary gradient | Furosemide |
| Thiazides | DCT | Block NCC cotransporter | Hydrochlorothiazide |
| K⁺-sparing | Collecting duct | Block ENaC (amiloride) or block aldosterone receptor (spironolactone) | Spironolactone, Amiloride |
13. QUICK REVISION TABLE - KEY VALUES
| Parameter | Normal Value |
|---|---|
| GFR | 125 mL/min (180 L/day) |
| Urine output | ~1-1.5 L/day |
| Renal blood flow (RBF) | ~1,200 mL/min (25% of CO) |
| Renal plasma flow (RPF/ERPF) | ~625 mL/min |
| Filtration fraction (FF) | ~0.2 (20%) |
| Glucose Tm | ~375 mg/min |
| Renal threshold for glucose | ~180-200 mg/dL |
| Urine osmolality range | 50-1200 mOsm/kg |
| Creatinine clearance (male) | ~125 mL/min |
| Plasma osmolality | 285-295 mOsm/kg |
HIGH-YIELD EXAM POINTS FOR MBBS
- Inulin is gold standard for GFR; PAH measures ERPF
- Filtration fraction = GFR/RPF = 0.2
- Net filtration pressure = 60 - 18 - 32 = +10 mm Hg
- Thick ascending limb is impermeable to water (the "diluting segment") - site of loop diuretics
- ADH acts on V2 receptors → AQP2 water channels → concentrated urine
- Aldosterone → sgk → ↑ ENaC → ↑ Na⁺ reabsorption, ↑ K⁺ secretion
- PCT reabsorbs glucose (100%) by secondary active transport via SGLT cotransporters
- Glucosuria occurs when plasma glucose exceeds ~180-200 mg/dL (renal threshold)
- JGA = macula densa + JG cells + lacis cells → controls renin secretion + TGF
- Micturition reflex: sacral (S2-S4) parasympathetic → detrusor contraction; voluntary control via external sphincter (pudendal nerve)
Ganong's Review of Medical Physiology, 26th Ed. | Guyton and Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.