A 15 year old unmarried non pregnant girl has vomiting, non bloody, watery in nature, one glass in quantity, a/w unilateral headache,.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive clinical analysis of this case:
Clinical Assessment: 15-Year-Old Girl with Unilateral Headache + Vomiting
Most Likely Diagnosis: Migraine Without Aura
This presentation is a textbook case. The combination of unilateral headache with nausea/vomiting in a pubertal adolescent girl is the hallmark of migraine.
Why Migraine?
Epidemiology supports this strongly
"At puberty, the incidence of migraine increases sharply in both boys and girls, but preferentially so in girls." — Bradley and Daroff's Neurology in Clinical Practice
The peak increase in migraine prevalence in females occurs precisely at puberty — a 15-year-old unmarried girl is in the highest-risk demographic window.
ICHD-3 Diagnostic Criteria for Migraine Without Aura
| Criterion | This Patient |
|---|---|
| A. ≥5 attacks fulfilling B–D | To be confirmed by history |
| B. Attacks lasting 4–72 hours (untreated) | Consistent |
| C. ≥2 of: unilateral location / pulsating quality / moderate–severe intensity / worsened by activity | Unilateral headache ✓ |
| D. During headache: nausea/vomiting OR photophobia + phonophobia | Vomiting ✓ |
| E. Not better accounted for by another ICHD-3 diagnosis | Exclude secondaries |
This patient satisfies criteria C (i) and D (i) already from the presenting complaint alone.
Pathophysiology
- The headache derives from activation of trigeminal afferents of the dura
- Associated with cortical spreading depression — a wave of neuronal and glial depolarization causing transient reduction in blood flow followed by hyperemia
- Serotonin (5-HT) dysregulation underlies both the pain and GI symptoms
- Vomiting is a direct feature of the migraine attack mediated via the chemoreceptor trigger zone and vagal pathways — the non-bloody, watery nature of this vomiting is typical (not related to a primary GI pathology)
Diagnostic Approach Flowchart
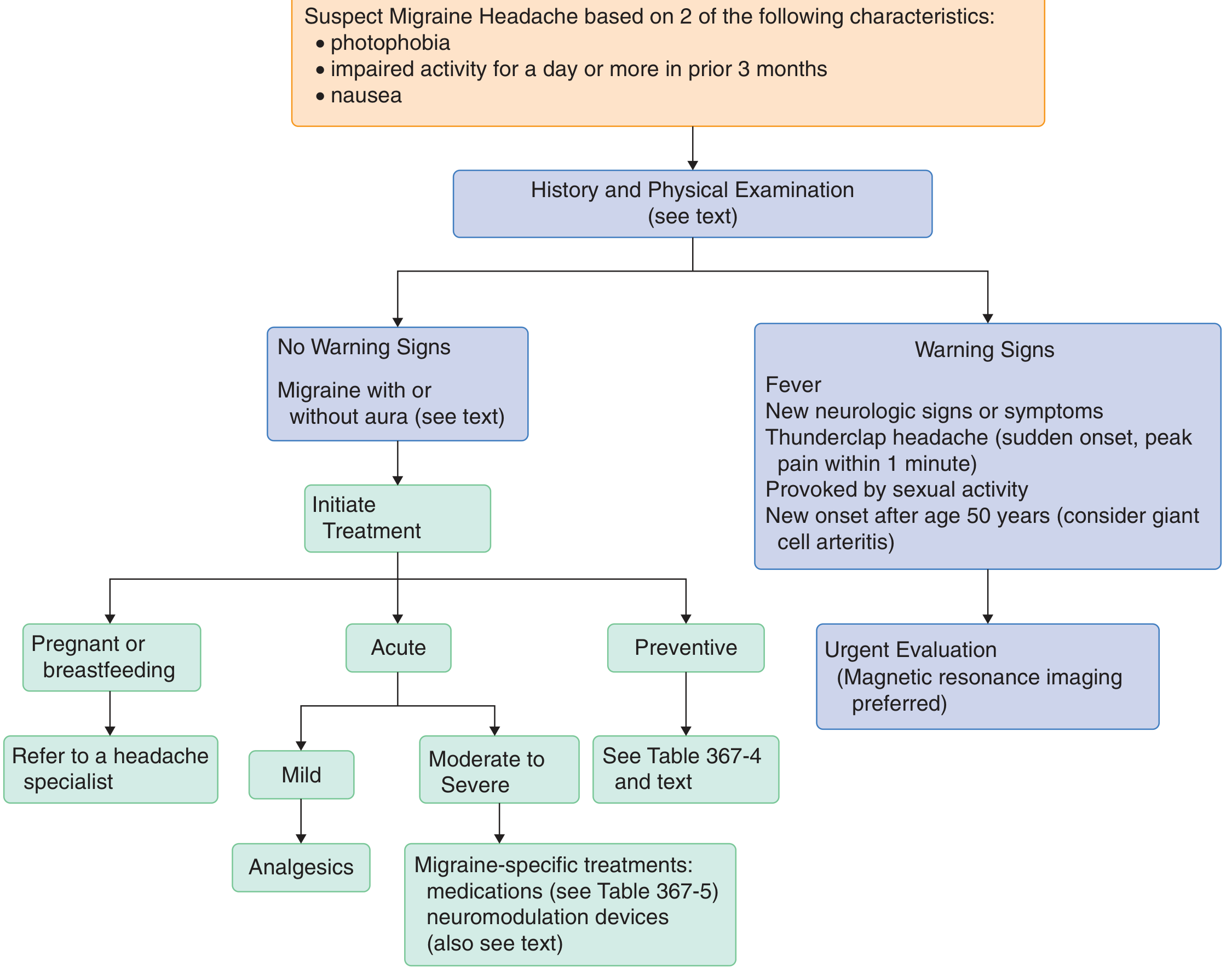
No warning signs present → Proceed to treatment (no neuroimaging needed if exam is normal)
Red Flag Warning Signs to Rule Out (SNNOOP10)
- Fever → meningitis/encephalitis
- Thunderclap headache (peak at 1 min) → subarachnoid hemorrhage
- New focal neurological signs → mass lesion/stroke
- Headache worsened by Valsalva/posture → raised ICP
- None of these are mentioned in this case
Management
Acute Treatment (Stratified by Severity)
Mild attacks:
- Paracetamol (acetaminophen) 650–1000 mg
- NSAIDs: Ibuprofen 400–600 mg (first-line in adolescents), Naproxen 500–825 mg, Diclofenac 50 mg
Moderate to Severe attacks:
- Triptans (5-HT1B/1D agonists): Sumatriptan, Rizatriptan — migraine-specific; vasoconstriction + trigeminal inhibition
- Contraindications: uncontrolled hypertension, ischemic heart disease (less relevant in a 15-year-old but should be noted)
- Antiemetics for vomiting: Metoclopramide 10 mg IV/oral, Prochlorperazine 10 mg
- Note: Ondansetron should be used with caution in children as it can paradoxically worsen headache
- DHE (dihydroergotamine) for very severe/refractory attacks
Important: Avoid opioids (risk of medication overuse headache); avoid aspirin in children under 16 (Reye's syndrome risk)
Preventive Treatment (if ≥4 attacks/month or significant disability)
- Propranolol, Amitriptyline, Topiramate, Valproate
- Lifestyle: regular sleep, meals, hydration, stress management, avoid triggers (hormonal fluctuations, skipped meals, bright lights)
Differential Diagnoses to Consider
| Diagnosis | Feature that distinguishes from this case |
|---|---|
| Tension-type headache | Bilateral, pressure/band-like, NO vomiting |
| Raised ICP (tumor/pseudotumor) | Postural, morning headache, papilledema; would need MRI |
| Viral meningitis | Fever, neck stiffness, altered consciousness |
| Cyclic vomiting syndrome | Vomiting predominant, headache secondary |
| Sinusitis | Facial pressure, purulent discharge |
Key Teaching Points
- Unilateral headache + vomiting in a pubertal girl = migraine until proven otherwise
- Diagnosis is clinical — neuroimaging only if warning signs or atypical features
- The watery non-bloody vomiting is a direct migraine symptom, not a GI cause
- Triptans are first-line for moderate–severe attacks but should be used early ("prompt treatment improves outcome")
- Medication overuse is a major risk — counsel on limiting acute treatment to ≤10–15 days/month
Sources: Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine 26th ed.; Cummings Otolaryngology; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Anti ematic for 15 year girls with brand name and dosages
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
antiemetics for 15 year old adolescent migraine vomiting brand names doses metoclopramide ondansetron domperidone
I have comprehensive textbook data. Let me now compile a complete, well-structured answer.
Antiemetics for a 15-Year-Old Girl (Migraine-Associated Vomiting)
At age 15, adult dosing applies for most antiemetics (weight typically ≥40 kg). Below are all commonly used antiemetics, stratified by drug class, with generic name, brand name(s), dose, route, and key notes.
🥇 FIRST-LINE
1. Ondansetron (5-HT₃ antagonist)
| Parameter | Detail |
|---|---|
| Brand names | Zofran, Emeset, Vomikind, Ondem |
| Dose (age ≥12) | 4–8 mg oral / IV / ODT (orally disintegrating tablet) |
| Route | PO, IV, ODT (melt-on-tongue — preferred when vomiting) |
| Frequency | Every 8–12 hours as needed |
| Max single dose | 8 mg |
| Notes | First-line in ED and outpatient. ODT is ideal when the patient is actively vomiting and can't swallow tablets. Risk of QT prolongation — check ECG if at risk; correct K⁺/Mg²⁺ first. Avoid concurrent serotonergic drugs. Caution: can paradoxically worsen headaches in some children |
2. Metoclopramide (Dopamine D₂ antagonist / prokinetic)
| Parameter | Detail |
|---|---|
| Brand names | Reglan, Perinorm, Maxolon, Metonia |
| Dose | 10 mg oral / IV / IM (0.1–0.15 mg/kg in children) |
| Route | PO, IV (over 5 min), IM |
| Frequency | Every 6–8 hours as needed |
| Notes | Dual benefit in migraine — antiemetic + mild analgesic effect via central dopamine blockade. Preferred for migraine-associated vomiting. Risk of extrapyramidal side effects (dystonia, akathisia) — pretreat with diphenhydramine (25 mg) if giving IV. Avoid >3 days continuous use (tardive dyskinesia risk) |
🥈 SECOND-LINE
3. Domperidone (Peripheral D₂ antagonist)
| Parameter | Detail |
|---|---|
| Brand names | Motilium, Domstal, Vomistop, Omidom |
| Dose | 10 mg oral (0.25 mg/kg/dose) |
| Route | PO (tablet or suspension) |
| Frequency | 3 times daily, 15–30 min before meals |
| Notes | Preferred oral antiemetic in adolescents — does not cross blood-brain barrier, so minimal EPS risk. Available OTC in many countries. Also mildly prokinetic. Risk of QT prolongation (lesser than metoclopramide) |
4. Prochlorperazine (Phenothiazine / D₂ antagonist)
| Parameter | Detail |
|---|---|
| Brand names | Compazine, Stemetil, Nauseals |
| Dose | 5–10 mg oral; 5–10 mg IM/IV; 25 mg PR (suppository) |
| Route | PO, IM, IV, rectal |
| Frequency | Every 6–8 hours |
| Notes | Effective for refractory migraine vomiting. More sedating than metoclopramide. EPS risk — co-administer diphenhydramine if giving parenterally. Avoid in children <10 kg. Third-line in ED setting |
🥉 THIRD-LINE / SITUATIONAL
5. Promethazine (Phenothiazine / H₁ + D₂ antagonist)
| Parameter | Detail |
|---|---|
| Brand names | Phenergan, Avomine, Fenazil |
| Dose (>2 years) | 0.25–1 mg/kg/dose (usually 12.5–25 mg at age 15) |
| Route | PO, IM, PR (suppository); IV NOT recommended (severe tissue necrosis risk) |
| Frequency | Every 4–6 hours |
| Notes | Highly sedating — good for acute attacks requiring rest. Black Box Warning: Avoid in children <2 years (respiratory depression). More EPS side effects than other agents |
6. Dimenhydrinate (H₁ antihistamine)
| Parameter | Detail |
|---|---|
| Brand names | Dramamine, Gravol, Dimetabs |
| Dose (≥12 years) | 50–100 mg oral |
| Route | PO, IM |
| Frequency | Every 4–6 hours |
| Notes | Mild antiemetic; useful for motion sickness–type nausea. Sedating. Not migraine-specific but widely available OTC |
Summary Preference Table for This Patient
| Situation | Preferred Drug | Brand | Dose |
|---|---|---|---|
| Mild vomiting, can swallow | Domperidone | Motilium | 10 mg TDS oral |
| Active vomiting, can't swallow tablets | Ondansetron ODT | Zofran (melt) / Vomikind MD | 4–8 mg under tongue |
| Moderate vomiting + migraine headache | Metoclopramide | Perinorm / Reglan | 10 mg IV/oral |
| Severe/refractory, hospital setting | Prochlorperazine | Stemetil | 5–10 mg IM |
| Needs sedation + antiemetic | Promethazine | Phenergan | 12.5–25 mg oral/IM |
⚠️ Key Safety Points for a 15-Year-Old Girl
- No IV promethazine — risk of tissue necrosis
- Metoclopramide — always give slowly IV (over ≥5 min); have diphenhydramine ready for EPS
- Ondansetron — check QTc if giving IV; avoid in prolonged QT
- Aspirin-containing antiemetic combinations — avoid (Reye's syndrome risk <16 years)
- Domperidone is the safest oral option with the least CNS side effects for outpatient use
Sources: Rosen's Emergency Medicine; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology 16e
Anti ematic for 15 year girls with brand name and dosages
This is the same question as before — here's the complete answer again for reference:
Antiemetics for a 15-Year-Old Girl (Migraine-Associated Vomiting)
At 15 years, adult dosing generally applies (weight typically ≥40 kg).
🥇 FIRST-LINE
1. Ondansetron — 5-HT₃ Antagonist
| Brand names | Zofran, Emeset, Vomikind, Ondem |
| Dose | 4–8 mg oral / IV / ODT (orally disintegrating tablet) |
| Frequency | Every 8–12 hours PRN |
| Max single dose | 8 mg |
| Best form when vomiting | ODT (dissolves on tongue — no swallowing needed) |
| Key caution | QT prolongation (check ECG if at risk); paradoxically can worsen headache in some children |
2. Metoclopramide — D₂ Antagonist + Prokinetic
| Brand names | Reglan, Perinorm, Maxolon, Metonia |
| Dose | 10 mg oral / IV (over 5 min) / IM |
| Pediatric dose | 0.1–0.15 mg/kg |
| Frequency | Every 6–8 hours PRN |
| Advantage in migraine | Dual benefit — antiemetic + direct analgesic effect on migraine |
| Key caution | Extrapyramidal side effects (dystonia, akathisia) — pretreat with diphenhydramine 25 mg if giving IV; avoid >3 consecutive days |
🥈 SECOND-LINE
3. Domperidone — Peripheral D₂ Antagonist
| Brand names | Motilium, Domstal, Vomistop, Omidom |
| Dose | 10 mg oral (0.25 mg/kg/dose) |
| Frequency | 3 times daily, 15–30 min before meals |
| Advantage | Does NOT cross blood-brain barrier → minimal EPS risk → safest oral option for outpatient use |
| Key caution | Mild QT prolongation risk |
4. Prochlorperazine — Phenothiazine
| Brand names | Compazine, Stemetil, Nauseals |
| Dose | 5–10 mg oral/IM/IV; 25 mg PR (suppository) |
| Frequency | Every 6–8 hours |
| Use | Refractory vomiting, hospital setting |
| Key caution | EPS risk — co-administer diphenhydramine; sedating |
5. Promethazine — H₁ + D₂ Antagonist
| Brand names | Phenergan, Avomine, Fenazil |
| Dose (age 15) | 12.5–25 mg oral / IM / PR |
| Frequency | Every 4–6 hours |
| Use | Acute attack requiring rest (highly sedating) |
| Key caution | ⚠️ NO IV route (tissue necrosis risk); avoid <2 years |
6. Dimenhydrinate — H₁ Antihistamine
| Brand names | Dramamine, Gravol, Dimetabs |
| Dose (≥12 years) | 50–100 mg oral / IM |
| Frequency | Every 4–6 hours |
| Use | Mild nausea, widely available OTC |
| Key caution | Sedating; not migraine-specific |
Quick-Reference by Clinical Situation
| Situation | Drug of Choice | Brand | Dose |
|---|---|---|---|
| Mild vomiting, can swallow | Domperidone | Motilium | 10 mg TDS oral |
| Active vomiting, can't swallow | Ondansetron ODT | Zofran Melt / Vomikind MD | 4–8 mg sublingual |
| Vomiting + migraine headache | Metoclopramide | Perinorm / Reglan | 10 mg IV/oral |
| Severe/refractory, hospital | Prochlorperazine | Stemetil | 5–10 mg IM |
| Needs sedation + antiemetic | Promethazine | Phenergan | 12.5–25 mg oral/IM |
⚠️ Safety Reminders Specific to This Patient
- No IV promethazine — risk of severe tissue necrosis
- Metoclopramide IV — infuse slowly over ≥5 min; keep diphenhydramine at hand for EPS
- Ondansetron — correct K⁺/Mg²⁺ before IV use; avoid concurrent serotonergic drugs
- No aspirin-containing combinations — Reye's syndrome risk under 16 years
- Domperidone is the preferred outpatient oral antiemetic in adolescents (fewest CNS side effects)
Sources: Rosen's Emergency Medicine; Roberts & Hedges' Clinical Procedures; Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic & Clinical Pharmacology 16e
This is a shared conversation. Sign in to Orris to start your own chat.