Cerebral blood flow and regulation, factors affecting icp perioperatively, methods to reduce icp intra operatively
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from Miller's Anesthesia to deliver a thorough, well-organized response.
Cerebral Blood Flow, ICP Regulation, and Intraoperative ICP Management
Primary source: Miller's Anesthesia, 10th edition (Chapters 10 & 53)
Part 1: Cerebral Blood Flow - Basics
The adult brain weighs ~1350 g (2% of body weight) but receives 12-15% of cardiac output. Resting oxygen consumption is ~3.5 mL O2/100 g/min; total brain O2 consumption (~50 mL/min) = 20% of whole-body utilization.
- Normal CBF: ~50 mL/100 g/min (gray matter ~80, white matter ~20)
- Normal ICP: <10-15 mmHg
- CPP = MAP - ICP (target >50-60 mmHg)
Approximately 60% of brain energy supports electrophysiologic (depolarization-repolarization) function; the rest maintains cellular homeostasis ("housekeeping").
Part 2: Regulation of Cerebral Blood Flow
CBF is regulated by three major mechanisms: chemical, myogenic (pressure/autoregulation), and neurogenic.
2.1 Chemical Regulation
PaCO2 (most potent vasomotor influence)
CBF changes 1-2 mL/100 g/min per mmHg change in PaCO2 in the physiologic range. Response is attenuated below PaCO2 <25 mmHg.
- Hypercapnia → cerebral vasodilation → ↑ CBF → ↑ ICP
- Hypocapnia → cerebral vasoconstriction → ↓ CBF → ↓ ICP
The mechanism is perivascular pH change (CO2 diffuses freely across the BBB, lowering pH around vessel walls, causing vasodilation). The effect is not sustained - over 6-8 hours, CSF bicarbonate adjusts and pH normalizes, returning CBF toward baseline.
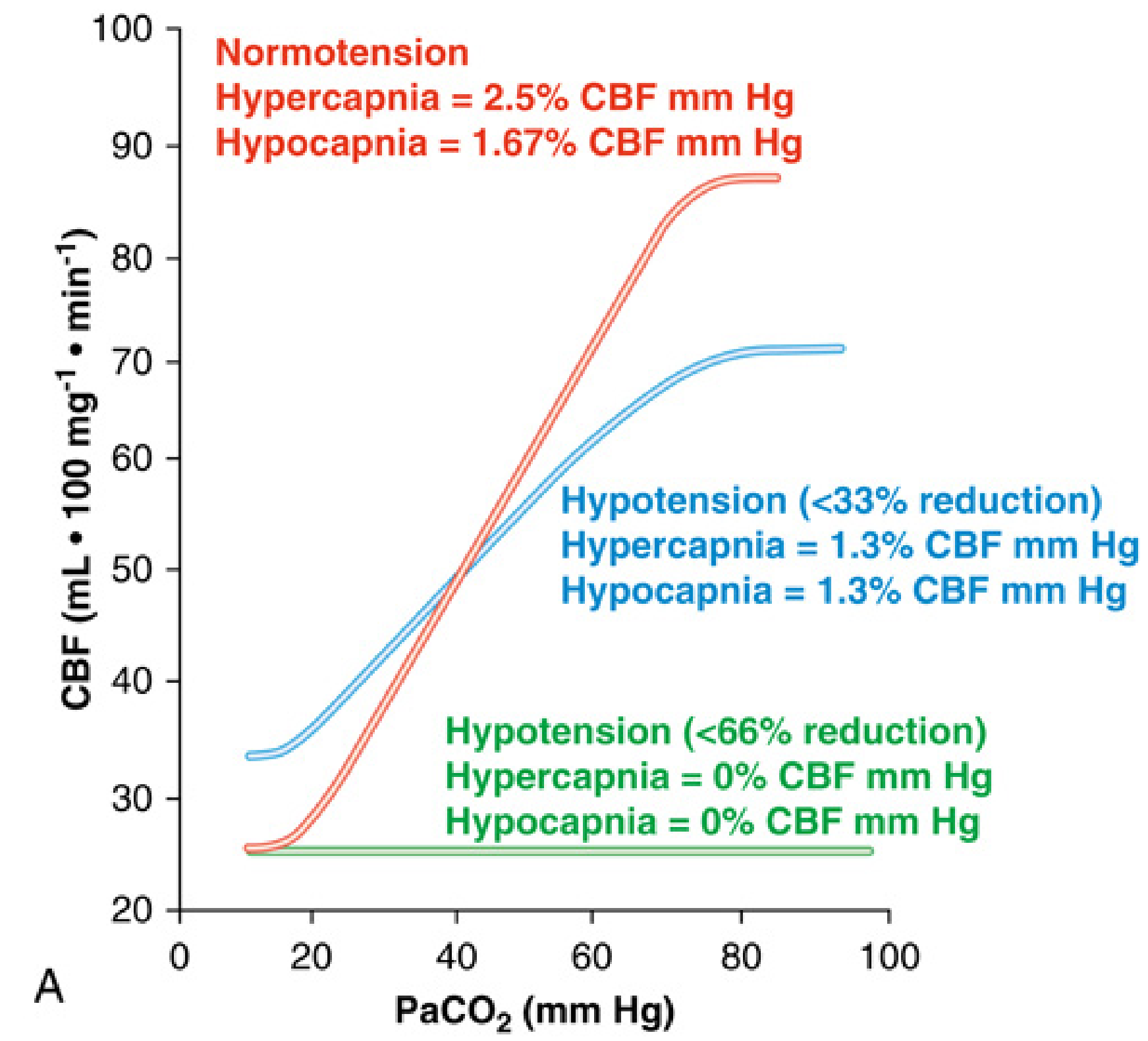
Fig: CBF vs PaCO2 under normotension, mild hypotension, and severe hypotension. Note: CO2 reactivity is abolished with severe hypotension (<66% reduction in MAP).
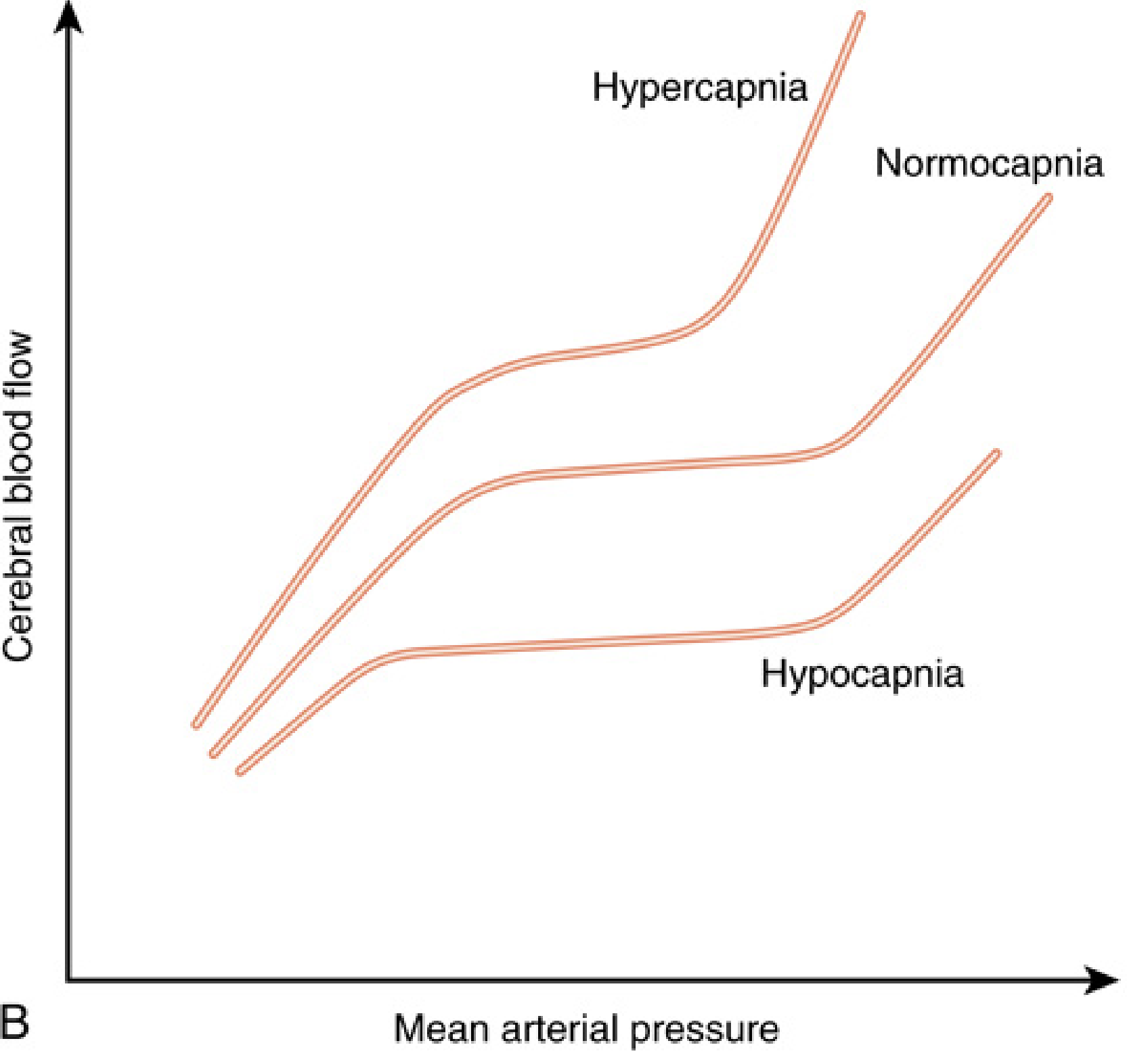
Fig: Hypercapnia shifts the autoregulation curve leftward (CBF higher at any given MAP); hypocapnia shifts it right.
PaO2
Changes from PaO2 60-300 mmHg have little influence on CBF. Below PaO2 60 mmHg, CBF rapidly increases (reflex vasodilation). Mechanisms: NO release from deoxyhemoglobin, ATP-sensitive K+ channel opening in vascular smooth muscle, rostral ventrolateral medulla oxygen sensing.
- Hypoxia + hypercapnia = synergistic vasodilation
- At 1 atm O2, CBF decreases ~18%
CMR (Flow-Metabolism Coupling)
Regional CBF and CMR are tightly coupled via the neurovascular unit (NVU): neurons + glia + pericytes + endothelial cells. Key mediators of coupling:
- Local by-products of metabolism: K+, H+, lactate, adenosine, ATP
- Glutamate → NO synthesis (potent vasodilator)
- Astrocyte activation → arachidonic acid → prostaglandins and EETs
- Retrograde endothelial hyperpolarization via K+ and Ca2+ channels propagates to proximal arterioles
Factors increasing CMR (and thus CBF): arousal, pain, seizures, hyperthermia
Factors decreasing CMR: anesthetics (barbiturates, propofol, isoflurane, etomidate), hypothermia, coma
Temperature
CMR decreases 6-7% per °C of cooling. Unlike anesthetics (which only suppress the electrophysiologic component), hypothermia reduces both the functional and the homeostatic components of CMR. EEG suppression occurs at ~18-20°C; at 18°C, CMRO2 is <10% of normothermic values.
2.2 Pressure Autoregulation (Myogenic Mechanism)
CBF is maintained relatively constant over a MAP range of approximately 50-150 mmHg by active vasoconstriction/dilation of cerebral resistance vessels.
- Below the lower limit of autoregulation (~50 mmHg): CBF becomes pressure-passive (ischemia risk)
- Above the upper limit (~150 mmHg): forced vasodilation and breakthrough hyperperfusion (edema, hemorrhage)
Modifiers of autoregulation:
- Hypercarbia and hypoxia attenuate autoregulation
- Chronic hypertension shifts both limits rightward
- Volatile anesthetics impair autoregulation in a dose-dependent fashion
- β-agonists, calcium channel blockers, nitrates, ACE inhibitors can all blunt autoregulation
Contemporary view: Autoregulation is not a static phenomenon - it is a dynamic, continuously integrated process dependent on MAP, PaCO2, PaO2, cardiac output, anesthetic agents, sympathetic tone, and the status of the BBB. The classical flat-plateau autoregulation curve is an oversimplification.
2.3 Neurogenic Regulation
The cerebral vasculature is extensively innervated; density is greatest on larger cerebral arteries.
Extrinsic innervation:
- Sympathetic (superior cervical ganglion): NE, epinephrine, dopamine → mild vasoconstriction; functionally important during hypertension to limit upper limit breakthrough
- Parasympathetic (sphenopalatine ganglion): ACh, VIP → vasodilation; contributes during hypotension
- Sensory (trigeminal): substance P, CGRP → vasodilation
Intrinsic innervation:
- Interneurons containing VIP, somatostatin, cholecystokinin modulate regional flow in response to local neural activity
Neurogenic control is of primary importance in the defense against hypertension (upper limit protection). Its vasodilatory capacity during hypotension is limited.
Part 3: Factors Affecting ICP Perioperatively
Monro-Kellie Doctrine: The cranium is a fixed-volume box containing brain (~80%), CSF (~10%), and blood (~10%). Any increase in one compartment must be offset by a decrease in another, or ICP rises.
ICP-volume relationship: Initially, compensation by CSF and venous blood translocation to extracranial spaces keeps ICP stable. Once compensatory reserve is exhausted, tiny incremental volume increases produce steep ICP rises.
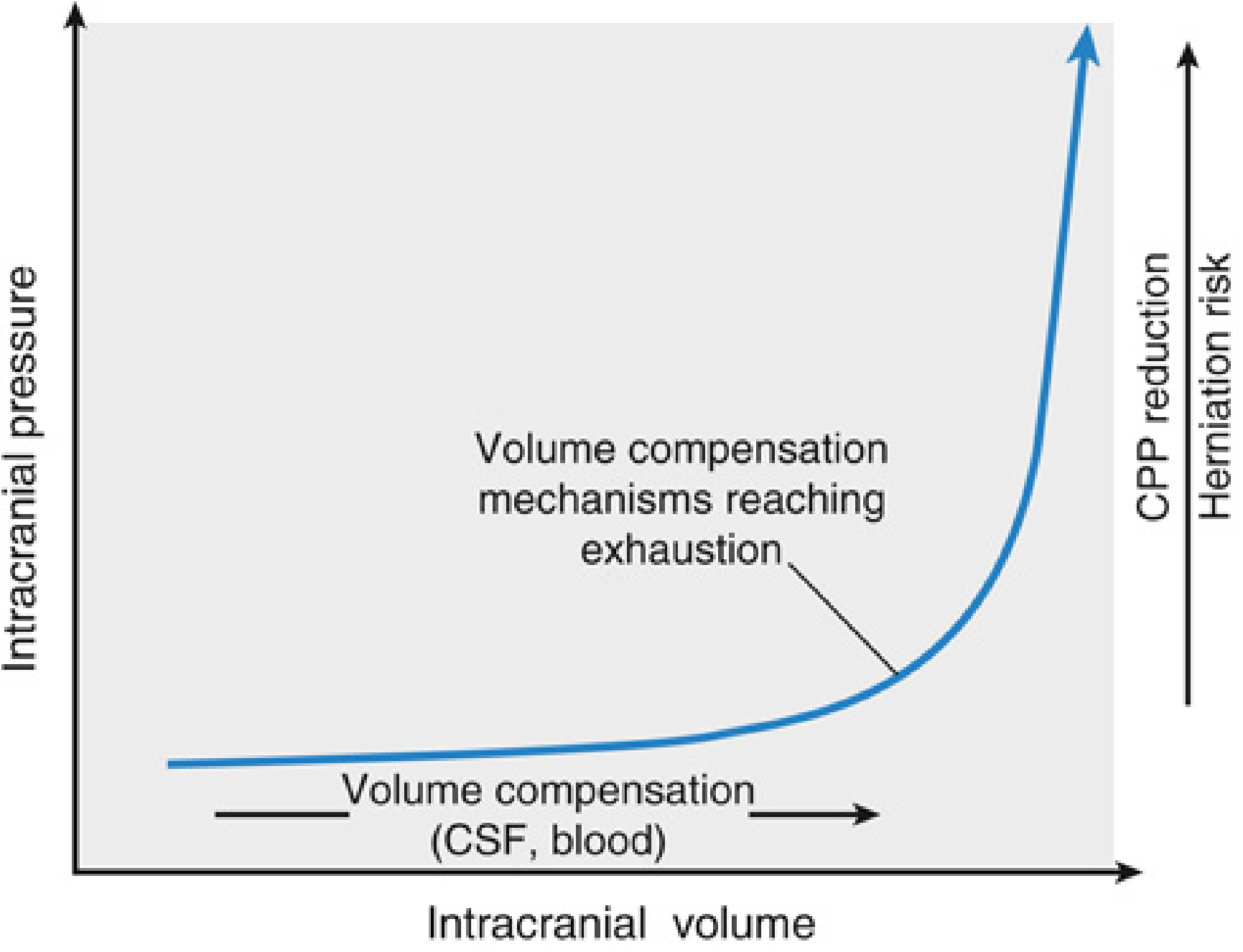
Fig 53.3: ICP-Volume relationship. The flat portion reflects intact compensatory reserve (CSF + venous blood displacement). Once exhausted, small volume increments cause exponential ICP rise, with risks of herniation or CPP reduction.
Perioperative Factors Raising ICP
| Category | Specific Factor | Mechanism |
|---|---|---|
| Ventilatory | Hypercapnia (hypoventilation) | CBF ↑ → CBV ↑ |
| Hypoxia (PaO2 <60 mmHg) | Cerebral vasodilation | |
| High airway pressure / PEEP | ↑ CVP → impaired venous drainage | |
| Bronchospasm, coughing, straining | ↑ intrathoracic pressure | |
| Positional | Extreme head rotation or flexion | Jugular vein compression |
| Head-down/Trendelenburg | Raised CVP + venous congestion | |
| Hemodynamic | Arterial hypertension (above autoregulatory range) | Pressure-passive CBF ↑ |
| Hypotension (below autoregulatory range) | Loss of autoregulation, reactive vasodilation | |
| Metabolic/Functional | Pain, arousal, inadequate anesthesia | CMR ↑ → coupled CBF ↑ |
| Seizures | Extreme CMR ↑ | |
| Hyperthermia | CMR ↑, CBF ↑ | |
| Anesthetic | Volatile agents (dose-dependent) | Cerebral vasodilation (↑CBV), impaired autoregulation |
| N2O | Increases CMR and CBF | |
| Ketamine | Increases CMR and CBF | |
| Succinylcholine | Small, transient ↑ ICP (can be blunted by pre-treatment with NDMB) | |
| Histamine-releasing NMBs (atracurium) | Cerebral vasodilation | |
| Surgical | Laser/bipolar coagulation near venous sinuses | Venous obstruction |
| Retractor pressure | Direct parenchymal compression | |
| Mass lesion (hematoma, air + N2O, clamped ventricular drain) | Volume expansion | |
| Fluid | Hypo-osmolar fluids (5% dextrose, excess free water) | Osmotic gradient drives fluid into brain |
Part 4: Intraoperative Methods to Reduce ICP / Achieve Brain Relaxation
The operative strategy targets reducing volume in any of the four intracranial subcompartments: cells, blood (CBV), CSF, extracellular fluid (edema).
4.1 Checklist for Acute "Tight Brain" - First-Line Steps (Box 53.3)
Step 1 - Optimize pressures:
- Eliminate extreme head rotation/flexion → ensure free jugular venous drainage
- Head-up 15-30° → reduce CVP and facilitate venous drainage
- Avoid excessive PEEP; check for bronchospasm, pneumothorax
- Optimize PaCO2 and PaO2
- Treat arterial hypertension if above autoregulatory range
Step 2 - Control metabolic rate:
- Ensure adequate depth of anesthesia (pain and arousal increase CMR)
- Treat hyperthermia
- Control seizures
Step 3 - Eliminate potential vasodilators:
- N2O, volatile agents, nitroprusside, calcium channel blockers
Step 4 - Rule out mass lesions:
- New hematoma, expanding pneumocephalus (if N2O in use), clamped CSF drain
4.2 Reduction of CBV - Ventilation
Controlled hyperventilation (target PaCO2 30-35 mmHg):
- Reduces CBF by 1-2 mL/100 g/min per mmHg ↓ PaCO2
- Each mmHg ↓ PaCO2 reduces CBV by ~0.04 mL/100 g
- Minimum PaCO2 of 25 mmHg (not less) - below this, ischemia risk with minimal additional ICP benefit
- Effect is not sustained (6-8 hours for adaptation)
- In head-injured patients with already-low CBF: use cautiously; prophylactic hyperventilation is inadvisable
- Indication: raised/uncertain ICP, imminent herniation, intraoperative brain bulge
4.3 CSF Drainage
- Lumbar drain or ventriculostomy (external ventricular drain, EVD) - most direct, rapid method
- "Brain needle" CSF aspiration through cortical surface intraoperatively
- Reduces CSF compartment volume directly, bypasses dependence on pharmacology
4.4 Osmotherapy
Mannitol (20% solution)
- Dose: 0.25-1.5 g/kg IV infused over 10-15 minutes
- Most common intraoperative osmotic agent
- Mechanisms:
- Immediate rheologic effect - reduces blood viscosity → reflex vasoconstriction maintains O2 delivery → ↓ CBV
- Osmotic effect (delayed 15-30 min) - creates osmotic gradient drawing water out of brain parenchyma, reducing brain bulk
- Must infuse over 10-15 minutes - rapid bolus causes extreme hyperosmolarity at cerebral vasculature, paradoxical vasodilation and brain engorgement
- Upper osmolarity limit: ~320 mOsm/L
- Adverse effects: diuresis, volume depletion, rebound edema if BBB severely disrupted
Hypertonic Saline (HTS)
- Available in 3%, 7.5%, 15%, 23.4% concentrations
- Increasing use in critical care as alternative to mannitol
- Advantages over mannitol: no diuresis, maintains intravascular volume, may benefit patients refractory to mannitol
- Equiosmolar doses achieve similar initial ICP reduction
- In TBI patients, HTS may provide better combined ICP and CPP effect
Furosemide
- Loop diuretic - can be used alone or in combination with mannitol
- Combination (furosemide + mannitol) acts synergistically - additive effect on brain dehydration
4.5 CMR Suppression - Reduction of Coupled CBV
Barbiturates (thiopental, pentobarbital):
- Cause dose-related suppression of EEG → ↓ CMR → coupled ↓ CBF and CBV
- Reduce ICP effectively; supported by ICU evidence
- Used as a "last resort" - significant hemodynamic effects
Propofol:
- Has gained popularity for CMR suppression intraoperatively
- Caution: propofol infusion syndrome (metabolic acidosis + rhabdomyolysis) with prolonged ICU infusions
- Less ICU evidence than barbiturates for ICP control
Both agents: maximum CMR reduction occurs at EEG suppression - further dose increase gives no additional CMR/CBF benefit (housekeeping component is preserved)
4.6 Anesthetic Choice
| Agent | Effect on CBF/ICP | Notes |
|---|---|---|
| Propofol | ↓ CBF, ↓ ICP | Preferred TIVA for neuro; maintains autoregulation |
| Barbiturates | ↓↓ CBF, ↓↓ ICP | Most potent CMR suppressors |
| Etomidate | ↓ CBF, ↓ ICP | Preserves autoregulation; adrenal suppression concern |
| Volatile agents | ↑ CBF (dose-dependent), ↓ CMR | At ≤1 MAC, ICP effect modest; above 1.5 MAC, significant cerebral vasodilation |
| N2O | ↑ CBF, ↑ CMR | Avoid or use with caution in intracranial HTN |
| Ketamine | ↑ CBF, ↑ ICP | Traditionally avoided; recent data suggest may be acceptable with controlled ventilation |
| Opioids | Minimal direct effect | Fentanyl/remifentanil maintain autoregulation; minimize painful stimulus response |
| Dexmedetomidine | Modest ↓ CBF | Reduces sympathetic tone; preserves autoregulation |
4.7 Patient Positioning
- Head-up 15-30° - most important positional measure; facilitates venous drainage, reduces CVP
- Neutral head position - avoid compression of jugular veins
- Avoid extreme Trendelenburg
4.8 Corticosteroids
- Dexamethasone - effective for reducing vasogenic edema (peritumoral), typically 4 mg q6h perioperatively
- No benefit for cytotoxic edema (TBI, stroke)
- Reduces BBB permeability and tumor-associated inflammatory edema
4.9 Temperature Management
- Avoid hyperthermia - each 1°C rise increases CMR ~6-7%, increasing CBF and ICP
- Mild hypothermia (34-35°C) may reduce CMR and brain bulk intraoperatively, though outcome benefit is not clearly established
- Major benefit of hypothermia during circulatory arrest: CMRO2 <10% of baseline at 18°C
4.10 Surgical Options (Last Resort)
- Lobectomy or removal of bone flap (decompressive craniectomy)
- Evacuation of hematoma or space-occupying lesion
- Permanent or temporary CSF diversion
Summary: Rapid ICP Reduction Methods (Box 53.4, Miller's)
- Further reduction of PaCO2 (target ~25-30 mmHg; no lower than 23-25 mmHg)
- CSF drainage (EVD or brain needle)
- Diuresis (mannitol, furosemide, hypertonic saline)
- CMR suppression (barbiturates, propofol)
- MAP reduction (if dysautoregulation - pressure-passive state)
- Surgical control (lobectomy, bone flap removal, hematoma evacuation)
Source: Miller's Anesthesia, 10th ed., Chapters 10 (Cerebral Physiology) and 53 (Neuroanesthesia), pp. 931-990 and 8114-8145.
This is a shared conversation. Sign in to Orris to start your own chat.