Pilonidal sinus iska full treatment btao with medicine name duration and doses according to mbbs medicine harrison or kd tripathi pharmacology book ke samjhao
Reading File
Finding Sources
Finding Sources
Searching the Web
pilonidal sinus treatment antibiotics surgery management guidelines 2024
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Ab main comprehensive answer likhne ke liye tayyar hoon. Saari information sources se collect ho gayi hai.
Pilonidal Sinus - Mukammal Ilaj (Harrison's + Surgery Textbooks + KD Tripathi/Katzung Pharmacology)
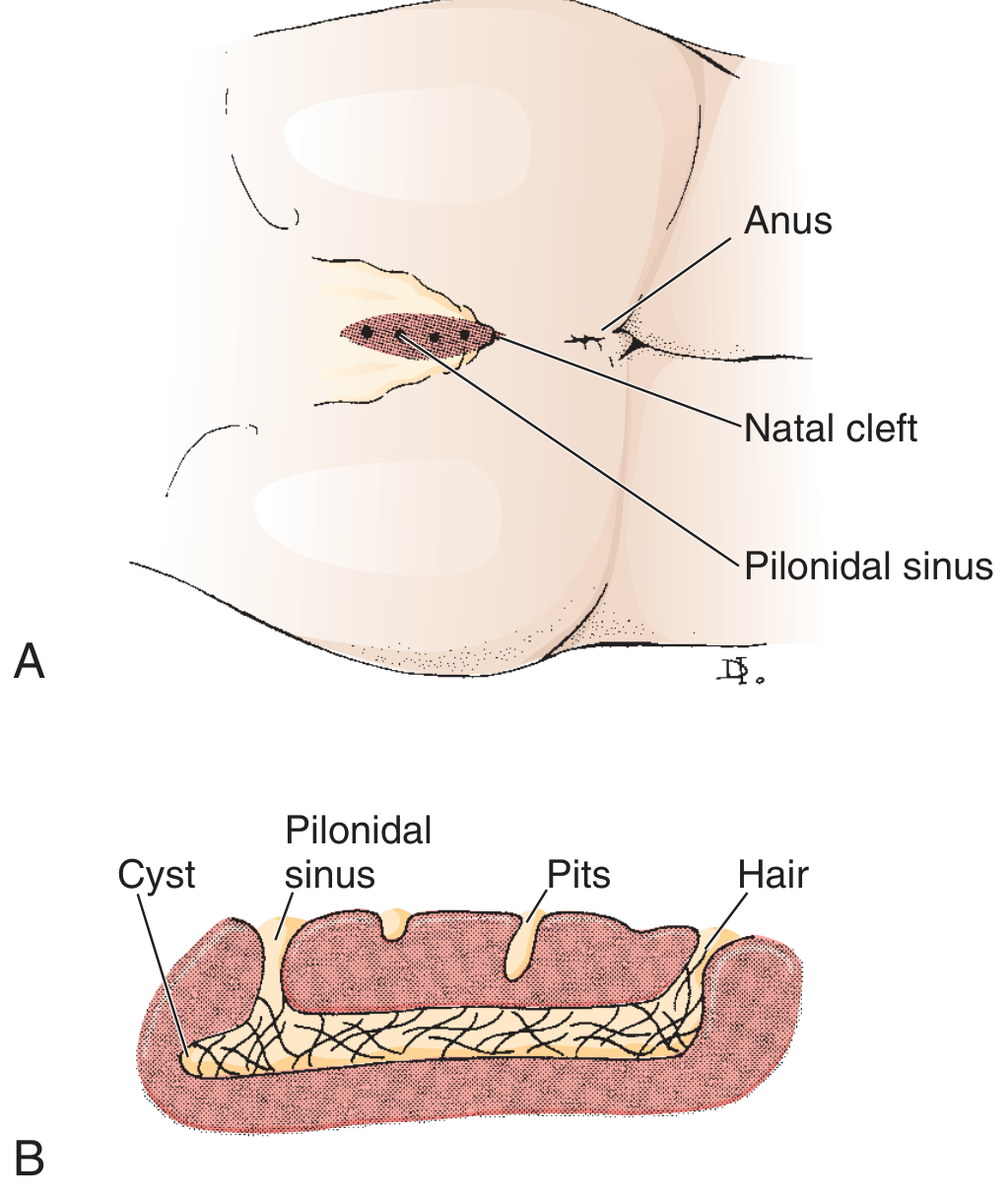
Fig: Pilonidal sinus - natal cleft mein location (A) aur cross section showing cyst, pits aur hair (B)
Pilonidal Sinus Kya Hai?
Pilonidal sinus ek acquired condition hai - "Pilus" (hair) + "Nidus" (nest). Sacrococcygeal area (gluteal cleft) mein baal subcutaneous tissue mein ghus jaate hain, foreign body granuloma banata hai, aur sinus tract form hoti hai. Anus se 5-10 cm upar midline mein hota hai.
Typical Patient: Young adult, 20-25 years, male (3:1 male:female ratio), hirsute, obese, sedentary job
Bacteria: Mixed flora - Staphylococcus aureus + Anaerobes (Bacteroides spp.) - (Sabiston Surgery, 21st Ed.)
DISEASE STAGES - Presentation ke Hisaab Se Ilaj
STAGE 1: ASYMPTOMATIC / MILD PILONIDAL SINUS
(Sirf pit hai, koi abscess nahi, minimal symptoms)
Conservative Management
- Shaving/Laser depilation: Natal cleft ke hair regularly shave karein - weekly ya fortnightly. Yahi sabse important preventive measure hai
- Hair removal from sinus openings with forceps/hemostat
- Hygiene: Area ko saaf aur dry rakhein
- No antibiotics needed at this stage
"In mild cases, treatment may involve simply shaving the hair on a regular basis to prevent it from imbedding into the intergluteal cleft." - Sleisenger & Fordtran's GI and Liver Disease, p.1562
STAGE 2: ACUTE PILONIDAL ABSCESS
(Pain, swelling, erythema, fever - acute presentation ~50% cases)
PRIMARY TREATMENT: Incision & Drainage (I&D)
- Yahi gold standard hai acute abscess ke liye
- Lateral incision - midline se bacha ke (off-midline better healing)
- Thorough curettage - sab hair aur necrotic tissue nikalo
- Wound open rakhein (packing with gauze)
- Local anesthesia se ho sakta hai (General/IV sedation bhi option)
"Primary incision and drainage should be performed in the ED for symptomatic relief." - Roberts & Hedges Emergency Procedures
ANTIBIOTICS KA ISTEMAL
Antibiotics kab dein? (IMPORTANT)
Antibiotics routine I&D ke baad ZARURI NAHI hote - sirf incase mein dein:
- Cellulitis surrounding tissue mein
- Immunocompromised patient
- Systemic signs - fever >38.5°C, tachycardia
- Surgical prophylaxis in elective excision
ANTIBIOTIC REGIMENS (Doses with Duration)
REGIMEN A: Oral - Cellulitis/Mild-Moderate Infection
(Non-MRSA, gram-positive + anaerobic coverage)
| Drug | Dose | Frequency | Duration |
|---|---|---|---|
| Amoxicillin-Clavulanate (Co-amoxiclav) | 625 mg (500/125 mg) | TDS (3x/day) | 7-10 din |
| + Metronidazole | 400-500 mg | TDS | 7-10 din |
Rationale (KD Tripathi / Katzung):
- Amoxicillin-Clavulanate: Beta-lactamase resistant, covers Staph aureus + gram-negative aerobes
- Metronidazole: Anaerobic coverage (Bacteroides spp.) - dose 500 mg TDS orally (30 mg/kg/day) - Katzung's Pharmacology, 16th Ed., p.1393
REGIMEN B: Alternative Oral Regimen
(If amoxicillin-clavulanate not available)
| Drug | Dose | Frequency | Duration |
|---|---|---|---|
| Cefalexin (Cephalexin) | 500 mg | QID (4x/day) | 7 din |
| + Metronidazole | 400 mg | TDS | 7 din |
REGIMEN C: MRSA Suspected
(Recurrent abscess, hospital-associated, no response to beta-lactams)
| Drug | Dose | Frequency | Duration |
|---|---|---|---|
| TMP-SMZ (Cotrimoxazole DS) | 960 mg (160/800 mg) | BD | 7-10 din |
| OR Doxycycline | 100 mg | BD | 7-10 din |
| OR Clindamycin | 300-450 mg | TDS | 7 din |
"Pustular/MRSA: TMP-SMZ, doxycycline, linezolid, vancomycin, daptomycin" - Katzung's Clinical Pharmacology, Empiric Skin/Soft Tissue Infection Table, p.1413
REGIMEN D: Severe/Hospitalized Patient (IV)
(Systemic sepsis, large abscess, immunocompromised)
| Drug | Dose | Frequency |
|---|---|---|
| Piperacillin-Tazobactam | 4.5 g | Q8H IV |
| OR Ampicillin-Sulbactam | 3 g | Q6H IV |
| + Metronidazole | 500 mg | Q8H IV |
STAGE 3: CHRONIC / RECURRENT PILONIDAL DISEASE
(Recurrent infections, multiple sinus tracts, incomplete healing)
Surgical Options
| Surgery | Details | Best For |
|---|---|---|
| Lay-open (unroofing) | Sinus tract khol ke khula chodna | Simple recurrent cases |
| Excision + Open healing | Complete excision, secondary intention healing | Most common, low recurrence |
| Excision + Primary closure | Off-midline closure preferred | Selected cases |
| Limberg Flap | Rhomboid rotation flap | Complex/extensive disease |
| Bascom Cleft Lift | Natal cleft flatten karna | Best long-term results |
| Z-plasty / V-Y flap | Extensive reconstruction | Very recurrent/complicated |
"Results of less extensive surgery are as good as more extensive surgery. Wounds healing by secondary closure have a lower incidence of recurrence than primary closure." - Sleisenger & Fordtran GI, p.1566
Healing Time: Excision with open wound = 40-50 din healing (8-12 weeks)
WOUND CARE (Post-Procedure)
- Cleansing: Soap+water se din mein 2-3 baar shower/irrigation
- Topical Metronidazole gel: Chronic wounds mein apply karein - granulation tissue improve karta hai
- Silver Nitrate cauterization: Excess granulation tissue ke liye
- Negative pressure dressing (VAC): Large wounds mein beneficial
- Phenol injection: Selected cases mein - ~20% recurrence rate
ADJUNCT THERAPIES
| Therapy | Purpose |
|---|---|
| Hair removal (shaving/waxing/laser) | Recurrence prevention - most important |
| Weight loss | Obesity ek major risk factor hai |
| Fibrin glue | Simple disease mein primary treatment |
| Pit-picking (Gips procedure) | Minimally invasive, less extensive disease |
PAIN MANAGEMENT
| Drug | Dose | Duration |
|---|---|---|
| Ibuprofen | 400-600 mg TDS | 3-5 din |
| Paracetamol | 500-1000 mg QID | PRN |
| Diclofenac | 50 mg TDS | Short term |
QUICK SUMMARY FLOWCHART
Pilonidal Sinus
|
├── Asymptomatic → Hair removal + hygiene (no antibiotics)
|
├── Acute Abscess → I&D (primary treatment)
| └── + Cellulitis → Antibiotics 7-10 days
| (Amox-Clav 625mg TDS + Metro 500mg TDS)
|
└── Recurrent/Chronic → Surgical Excision
├── Simple → Lay-open / Excision + open healing
└── Complex → Flap procedure (Limberg/Bascom)
SOURCES USED:
- Sabiston Textbook of Surgery, 21st Ed. - Pilonidal Disease ch. 97
- Sleisenger & Fordtran's GI and Liver Disease - ch. 129
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - ch. 37
- Pfenninger & Fowler's Procedures for Primary Care, 3rd Ed. - ch. 109
- Katzung's Basic & Clinical Pharmacology, 16th Ed. - Antibiotic empiric therapy table
- Harrison's Principles of Internal Medicine, 22nd Ed. - Drug indications table
Note: Harrison's main pilonidal sinus ka dedicated chapter nahi hai - yeh primarily surgery aur emergency medicine textbooks ka topic hai. Antibiotics ke doses KD Tripathi ke equivalent Katzung Pharmacology se confirm kiye gaye hain. Har patient mein antibiotic choice local resistance pattern aur clinical severity ke hisaab se adjust karein.
This is a shared conversation. Sign in to Orris to start your own chat.