
IMG_20260613_182941121_HDR.jpg
Diagnosis it and give mangement
Reading File
Finding Sources
Finding Sources
Searching PubMed
ascites management guidelines
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to provide a full clinical answer. Here is my complete response:
Clinical Diagnosis: Massive Ascites
The image shows a markedly distended, globular abdomen in a female patient with overlying skin changes including hyperpigmentation, lichenification, and fine scaling - consistent with massive ascites with chronic skin stretching. The umbilicus appears flattened/everted. These are classic features of longstanding, large-volume peritoneal fluid accumulation.
Differential Diagnosis
The three leading causes of ascites, in order of frequency, are:
| Cause | Frequency |
|---|---|
| Cirrhosis (hepatic portal hypertension) | ~85% |
| Peritoneal malignancy | ~7% |
| Cardiac failure | ~3% |
| Nephrotic syndrome, TB peritonitis, pancreatitis | Remainder |
In this patient (African female with bangles/context suggesting South Asia/sub-Saharan Africa), the most likely diagnoses are cirrhosis (alcoholic, viral hepatitis B/C, or NASH) or malignant ascites (ovarian, hepatic, or peritoneal carcinoma).
Workup - Key First Step: Diagnostic Paracentesis
Perform diagnostic paracentesis immediately and send fluid for:
- Cell count + differential (WBC >250 PMN/mm³ = spontaneous bacterial peritonitis, SBP)
- Albumin (to calculate SAAG - serum-ascites albumin gradient)
- Total protein
- Culture (blood culture bottles at bedside)
- Cytology (if malignancy suspected)
- Glucose, LDH
- ADA (adenosine deaminase) if TB suspected
SAAG Interpretation (Diagnostic Algorithm):
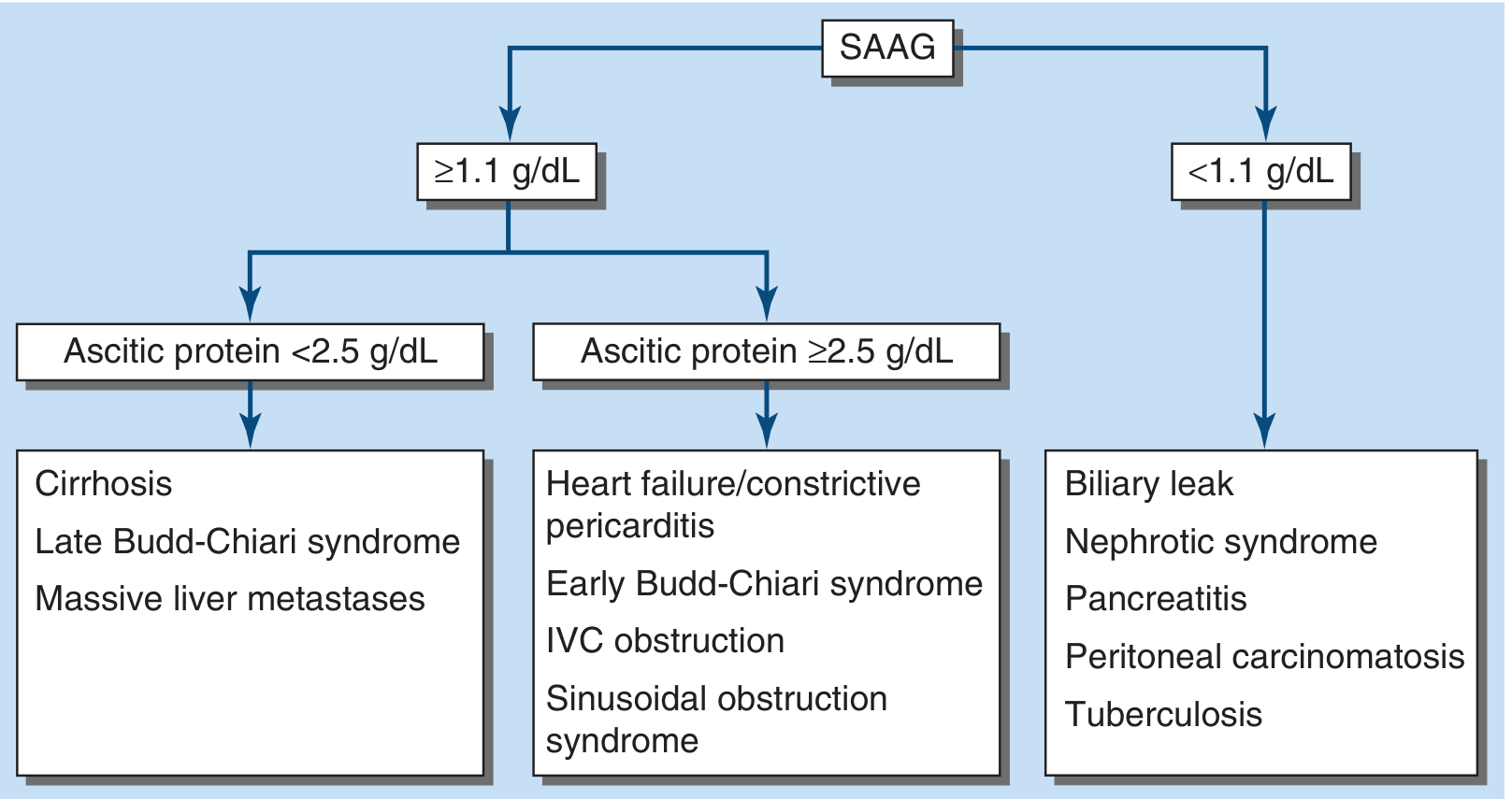
- SAAG ≥ 1.1 g/dL = portal hypertension (cirrhosis, cardiac failure, Budd-Chiari)
- SAAG < 1.1 g/dL = non-portal hypertension cause (TB, malignancy, nephrotic syndrome, pancreatitis)
(SAAG = serum albumin - ascitic fluid albumin)
Blood/Imaging Investigations
- LFTs, albumin, PT/INR, CBC (liver disease markers)
- Hepatitis B surface Ag, anti-HCV (viral hepatitis)
- Serum AFP (hepatocellular carcinoma)
- CA-125 (ovarian malignancy in women)
- Renal function panel, urine protein (nephrotic syndrome)
- Chest X-ray (pleural effusion, TB)
- Abdominal ultrasound / CT abdomen - confirm ascites, liver morphology, splenomegaly, portal vein, masses, lymphadenopathy
Management
Step 1 - Immediate (if SBP suspected or confirmed)
- IV Cefotaxime 2g q8h (or Ceftriaxone 1g daily) for 5-7 days
- IV Albumin 1.5 g/kg at diagnosis and 1 g/kg on day 3 to prevent hepatorenal syndrome
Step 2 - Medical Management of Ascites (Cirrhosis)
Sodium restriction: 2 g (88 mmol) per day - do NOT restrict more aggressively as it compromises nutrition.
Diuretics (first-line combination):
- Spironolactone 100 mg/day (aldosterone antagonist, first-line) - titrate every 3-4 days up to 400 mg/day max
- Furosemide 40 mg/day combined with spironolactone in a 40:100 ratio (furosemide:spironolactone), titrated up to 160 mg/day
- Target weight loss: 1 kg in first week, then 0.5 kg/day max (without edema) or 1 kg/day max (with peripheral edema)
Monitoring during diuretics:
- Renal function, electrolytes (watch for hyponatremia, hyperkalemia)
- If painful gynecomastia with spironolactone → switch to amiloride 5-40 mg/day
- Avoid NSAIDs, ACE inhibitors, ARBs
Long-term albumin (PILOT trial evidence):
- Adding albumin 40 g twice weekly x 2 weeks, then 40 g weekly to spironolactone + furosemide significantly reduces recurrent ascites and improves 18-month survival.
Step 3 - Refractory Ascites (10-20% of patients)
Defined as ascites not mobilized by sodium restriction + maximum diuretics, or diuretic side effects prevent max dosing.
| Option | Details |
|---|---|
| Large-Volume Paracentesis (LVP) | Remove all/most fluid; give IV albumin 6-8 g/L of fluid removed (especially >5L) to prevent post-paracentesis circulatory dysfunction |
| Midodrine (α1-agonist) | 7.5-12.5 mg TID - counters splanchnic vasodilation, improves diuretic response |
| TIPS (Transjugular Intrahepatic Portosystemic Shunt) | Superior to LVP for preventing recurrence; higher encephalopathy risk; PTFE-covered TIPS improves survival if LVP >twice/month |
| Peritoneovenous shunt | For patients not candidates for TIPS or transplant |
Note: Beta-blockers should be used cautiously - their use in refractory ascites may be associated with decreased survival.
Step 4 - Definitive Treatment
- Liver transplantation - refer early; ascites is a marker for decompensated cirrhosis (1-year survival ~50% without transplant)
- Treat underlying cause: antivirals for HBV/HCV, alcohol cessation, treat malignancy if present
Summary
| Domain | Action |
|---|---|
| Diagnosis | Diagnostic paracentesis + SAAG + cytology |
| Imaging | Abdo USS/CT |
| Labs | LFTs, viral hepatitis, AFP, CA-125, renal panel |
| Medical Rx | Sodium restriction + spironolactone + furosemide |
| Rescue | LVP + albumin if refractory |
| Escalation | TIPS or transplant referral |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine; EASL Clinical Practice Guidelines on TIPS [PMID: 40180845]; AGA Practice Update on Vasoactive Drugs and Albumin in Cirrhosis [PMID: 37978969]
⚠️ Disclaimer: This is a clinical educational response. Actual patient management must be performed by a qualified physician after direct examination and investigation.
This is a shared conversation. Sign in to Orris to start your own chat.