Why is there sever pain in mumps
Reading File
Finding Sources
Searching PubMed
mumps parotitis orchitis pathophysiology pain
!
HTTP 502 for https://eutils.ncbi.nlm.nih.gov/entrez/eutils/esearch.fcgi?tool=orrisai&email=dev%40orris.ai&api_key=***&db=pubmed&term=%28mumps+parotitis+orchitis+pathophysiology+pain%29+AND+%28%22Review%22%5Bpt%5D%29+NOT+%22Retracted+Publication%22%5Bpt%5D&retmode=json&retmax=3&sort=relevance&datetype=pdat&reldate=1825
We encountered an error while processing your request. Please try again or reach out to us for help.
What does unyielding nature of parotidomessetric fascia
Finding Sources
Finding Sources
Finding Sources
Searching the Web
parotidomasseteric fascia unyielding mumps pain mechanism
Reading File
Excellent - now I have all the information needed for a thorough answer.
The Unyielding Parotidomasseteric Fascia - Why It Causes Severe Pain in Mumps
What Is the Parotidomasseteric Fascia?
The parotid gland is completely enclosed within a tight fibrous capsule derived from the investing (deep cervical) fascia. This fascia splits into two layers to wrap around the gland:
| Layer | Attachment | Character |
|---|---|---|
| Superficial lamina (parotidomasseteric fascia) | Zygomatic arch | Thick and strong |
| Deep lamina | Styloid process, tympanic plate, ramus of mandible | Thinner |
The superficial layer - the parotidomasseteric fascia - is notably thick, tough, and inelastic. It does not stretch or yield when its contents swell.
Why "Unyielding" = Severe Pain in Mumps
In mumps, the paramyxovirus spreads via the bloodstream to the parotid gland, causing acute viral parotitis. The gland becomes inflamed and edematous - it wants to expand. But here is the problem:
The fascia does not give way. As the swollen gland presses outward against a non-compliant fibrous wall, intrinsic pressure inside the capsule rises sharply, compressing glandular tissue, blood vessels, and the rich nerve supply within.
This is directly analogous to compartment syndrome - swelling within a closed, inelastic space.
Specific Pain Mechanisms
- Capsular pressure on sensory nerves
- The parotid capsule is supplied by the great auricular nerve (C2, C3). Rising intracapsular pressure directly stimulates these pain fibers, causing the characteristic sharp, aching parotid pain.
- Earache (otalgia)
- The swollen glenoid (retroparotid) process of the gland, which extends medially behind the temporomandibular joint (TMJ), presses against the joint. This explains the referred ear pain patients commonly report.
- Trismus (difficulty opening the mouth)
- The inflamed, tense gland lies directly over the masseter muscle and near the TMJ. Pressure from the swollen gland makes chewing and mouth opening extremely painful - this is why patients classically refuse to eat.
- Pain on eating
- When a person eats, salivary flow is stimulated, increasing glandular secretion and volume - worsening capsular tension and pain. This is a hallmark feature of mumps parotitis.
Comparison with Other Glands
The same "unyielding capsule" principle explains mumps orchitis pain too. The testes are enclosed by the tunica albuginea - another tough, non-compliant fibrous sheath. When the virus replicates in the seminiferous tubules, testicular swelling within this rigid covering produces the severe testicular pain and tenderness reported in 15-35% of post-pubertal males.
Summary
The parotidomasseteric fascia is unyielding because it is derived from the thick investing layer of deep cervical fascia and has no capacity to stretch. When the parotid gland swells in mumps, this rigid enclosure converts inflammation into a high-pressure, closed-space injury - compressing nerves, vessels, and glandular tissue - which is the direct anatomical reason for the severe, throbbing pain, otalgia, and trismus that define mumps parotitis.
- Goldman-Cecil Medicine, Block 50 (Mumps - Pathobiology & Clinical Manifestations)
- Parotid Gland Anatomy, University of Baghdad Dental Lectures
Tonsilar artery supplies
Finding Sources
Searching the Web
tonsillar artery blood supply palatine tonsil anatomy branches
Reading File
Reading File
Here is a complete breakdown of the tonsillar artery and the blood supply of the palatine tonsil:
Tonsillar Artery - Blood Supply of the Palatine Tonsil
The Tonsillar Artery (Main Supply)
The tonsillar artery is a branch of the facial artery (itself a branch of the external carotid artery). It is the principal and most important blood supply to the palatine tonsil.
Course:
- Arises from the facial artery
- Passes upward between the medial pterygoid and styloglossus muscles
- At the superior border of styloglossus, it pierces the superior pharyngeal constrictor muscle
- Enters the pharynx and ramifies within the substance of the tonsil at its lower pole
This is clinically significant - the facial artery may lie very close to the lower pole of the tonsil, making it vulnerable during tonsillectomy.
All 5 Arteries Supplying the Tonsil
All are branches of the External Carotid Artery (ECA):
| # | Artery | Parent Vessel | Region Supplied |
|---|---|---|---|
| 1 | Tonsillar branch ⭐ (main) | Facial artery | Middle part, main supply |
| 2 | Ascending palatine branch | Facial artery | Lower pole |
| 3 | Dorsal lingual branches | Lingual artery | Lower part / tongue base |
| 4 | Ascending pharyngeal artery | External carotid directly | Upper part |
| 5 | Descending (lesser) palatine branch | Maxillary artery | Upper part |
Mnemonic - MAALT (all from ECA):
- M - Maxillary (descending palatine)
- A - Ascending pharyngeal
- A - Ascending palatine (facial)
- L - Lingual (dorsal lingual)
- T - Tonsillar (facial) ⭐
Venous Drainage
- The paratonsillar vein (external palatine vein) drains the tonsil - it runs on the lateral surface of the tonsil between the capsule and the superior constrictor
- Drains into the pharyngeal venous plexus or facial vein → Internal Jugular Vein (IJV)
The paratonsillar vein is the most common source of secondary post-tonsillectomy hemorrhage (reactionary bleeding).
Nerve Supply (for completeness)
- Glossopharyngeal nerve (CN IX) - tonsillar branches (main sensory supply)
- Lesser palatine nerve - from maxillary division of trigeminal (CN V2)
This dual nerve supply explains why tonsillitis can cause referred otalgia (ear pain via CN IX's tympanic branch - Jacobson's nerve).
Clinical Pearls
- Tonsillectomy bleeding - The facial artery near the lower pole is the feared vessel in primary hemorrhage
- Quinsy (peritonsillar abscess) - The rich blood supply and loose peritonsillar tissue allows rapid spread of infection
- All tonsillar arteries pierce the superior constrictor to reach the tonsil - this muscle is the surgical plane of dissection
- Gray's Anatomy for Students, p. 1189 (Arteries of Pharynx)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 (Vascular Supply - Tonsil)
What is palatine tonsil
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
The Palatine Tonsil
Definition and Location
The palatine tonsil is a paired mass of lymphoid tissue situated in the lateral wall of the oropharynx, lying within the tonsillar fossa - the triangular recess formed between the diverging:
- Palatoglossal arch (anterior pillar) - in front
- Palatopharyngeal arch (posterior pillar) - behind
There is one tonsil on each side of the throat.
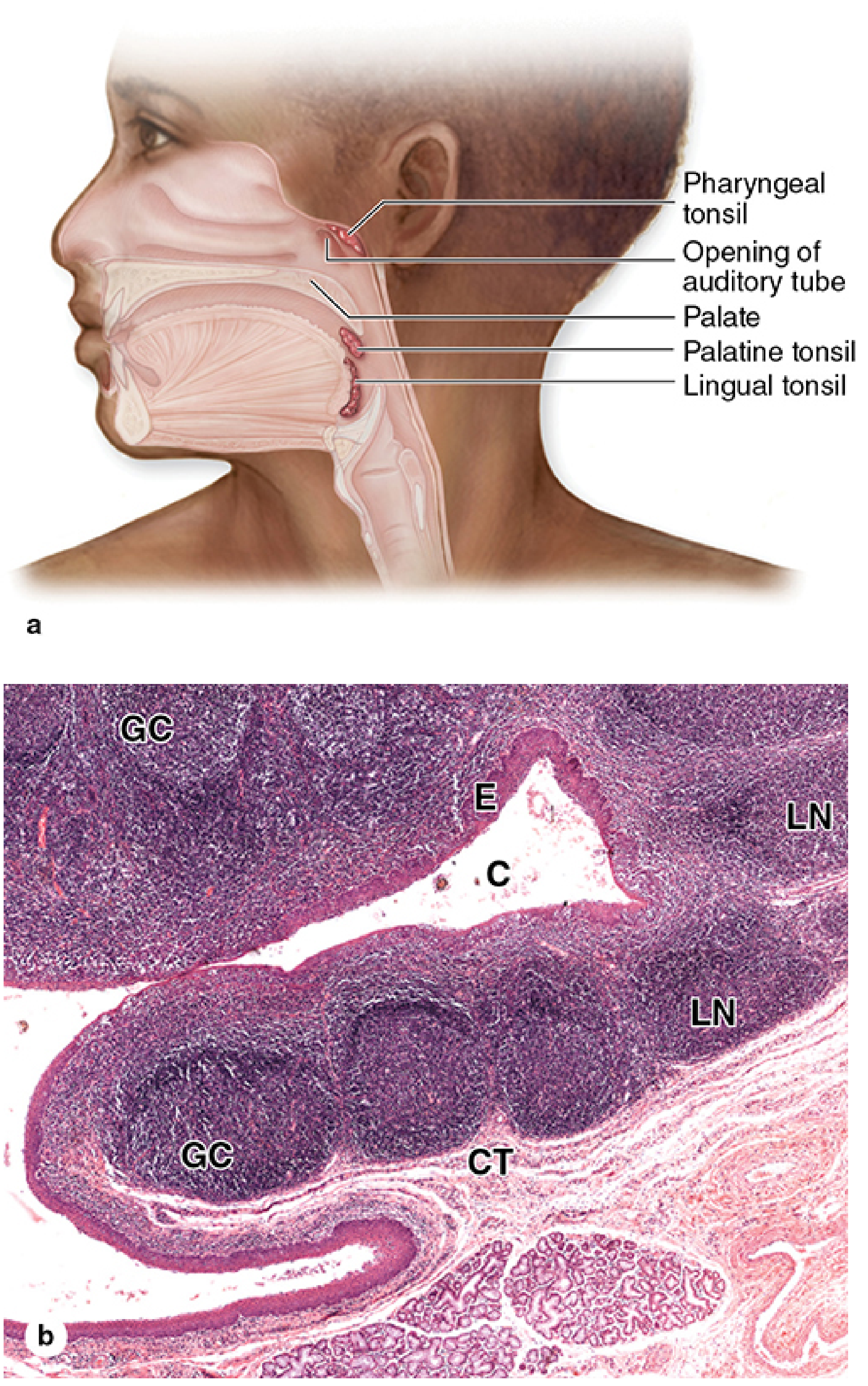
Waldeyer's Ring
The palatine tonsil forms the anteroinferior part of Waldeyer's ring - a ring of lymphoid tissue guarding the entrance to the digestive and respiratory tracts:
| Component | Location |
|---|---|
| Palatine tonsils (×2) | Lateral walls of oropharynx |
| Pharyngeal tonsil (adenoids) | Posterior wall of nasopharynx |
| Tubal tonsils (×2) | Around the opening of Eustachian tube |
| Lingual tonsil | Base of tongue |
| Smaller lymphoid collections | Intertonsillar intervals |
Size
- At puberty: approximately 10-15 mm transverse diameter, 20-25 mm vertical dimension
- After puberty: the tonsil begins to atrophy - by old age, only a small remnant of lymphoid tissue remains
Structure
Surfaces:
- Medial (free) surface - projects into the oropharynx; has a pitted appearance from 10-15 pit openings
- Lateral (deep) surface - covered by the fibrous tonsillar hemicapsule, which can be separated from the underlying superior constrictor muscle (the surgical plane in tonsillectomy)
The Tonsillar Crypts:
- The pits on the medial surface lead into 10-20 deep, branching, blind-ending crypts extending through the full thickness of the tonsil
- The crypts are lined by stratified squamous epithelium that is densely infiltrated with lymphocytes - so much so that the epithelial layer can be hard to identify histologically
- The crypts contain desquamated cells, lymphocytes, and bacteria
Histology
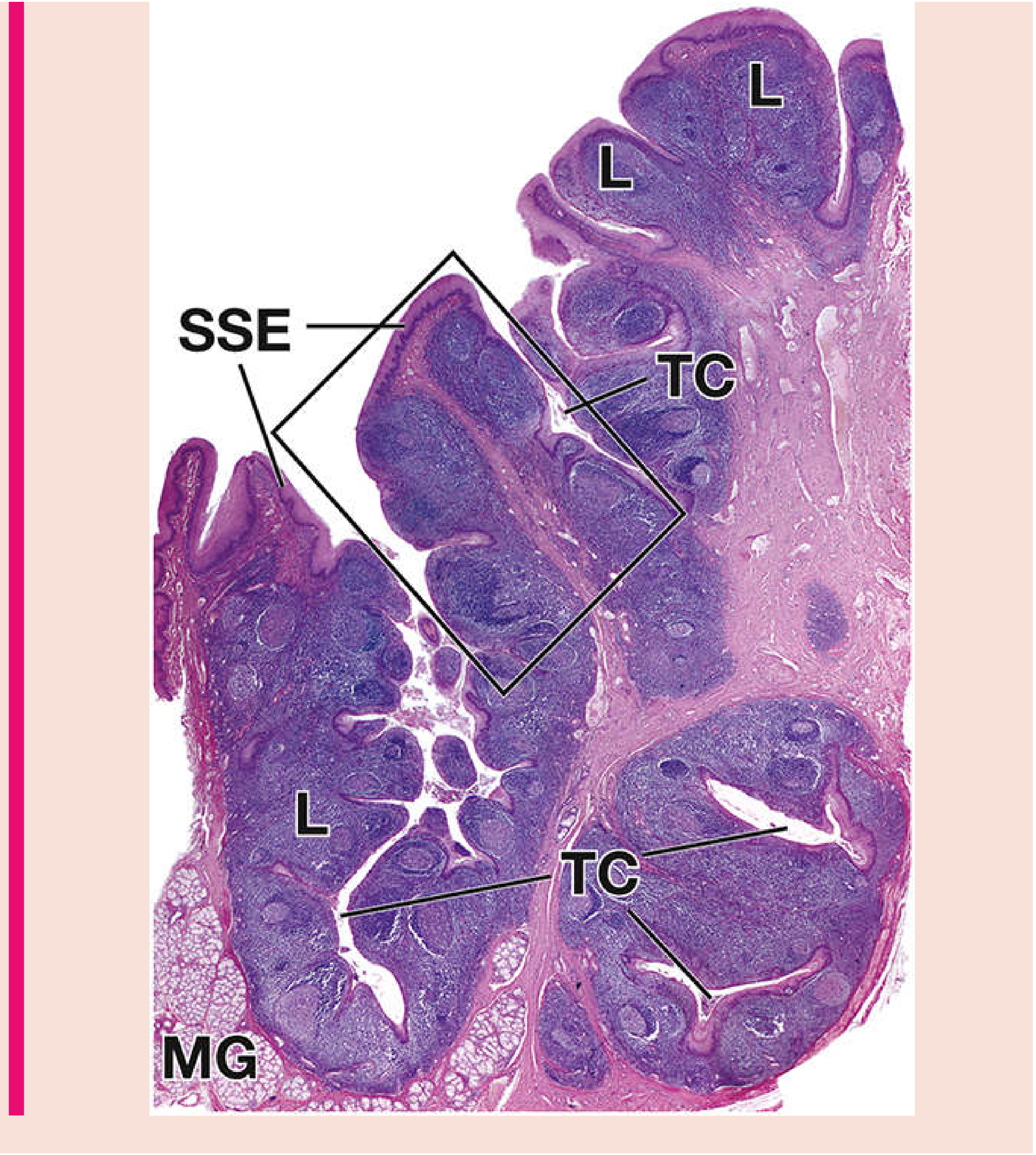
Key histological features:
| Label | Structure |
|---|---|
| SSE | Stratified squamous epithelium (surface covering) |
| TC | Tonsillar crypts (infoldings of epithelium) |
| L | Lymphoid tissue (packed lymphocytes + nodules) |
| GC | Germinal centers (within secondary lymphoid nodules) |
| MG | Mucous glands at the base |
| CT | Connective tissue capsule (deep surface) |
The lymphoid tissue is filled diffusely with lymphocytes, with many secondary lymphoid nodules especially concentrated around the crypts. These germinal centers are where B-cells undergo maturation and antibody production.
Function
The palatine tonsil is a secondary lymphoid organ. Its functions include:
- Antigen sampling - the crypts trap pathogens from swallowed food and inhaled air
- Immune activation - lymphocytes in the nodules mount B-cell and T-cell responses
- First-line defense - guards the common entry point of the respiratory and digestive tracts
- The tonsil has no afferent lymphatics - antigens enter directly via the crypt epithelium, not via lymph vessels
Clinical Importance
| Condition | Notes |
|---|---|
| Tonsillitis | Bacterial or viral infection of the tonsil; commonest in children |
| Quinsy (peritonsillar abscess) | Pus collects between the capsule and superior constrictor |
| Tonsillectomy | Dissection in the plane between hemicapsule and superior constrictor |
| Adenotonsillar hypertrophy | Enlarged tonsils can obstruct the airway causing sleep apnea |
| Tonsillar carcinoma | Squamous cell carcinoma; associated with HPV-16 |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Palatine tonsil section)
- Junqueira's Basic Histology, 17e (MALT and Tonsils)
- Histology: A Text and Atlas, Plate 14.1 (Palatine Tonsil)
This is a shared conversation. Sign in to Orris to start your own chat.