Ultrasound elastography in detail , definition, principle , technique , process , aim , types in detail
Reading File
search_medical_text
ultrasound elastography definition principle technique types
search_medical_text
strain elastography shear wave elastography process clinical applications
search_medical_image
ultrasound elastography types shear wave strain
GradeResponse
GradeResponse
GradeResponse
search_medical_text
shear wave elastography ARFI acoustic radiation force impulse liver fibrosis stiffness measurement
search_medical_text
strain elastography compression technique tissue displacement color mapping breast liver
I have sufficient information from retrieval plus my comprehensive knowledge to deliver a full, detailed answer.
Ultrasound Elastography — Comprehensive Overview
1. Definition
Ultrasound Elastography (USE) is an advanced ultrasound-based imaging technique that maps the mechanical properties of tissue — primarily stiffness (elastic modulus) — by measuring how tissue deforms in response to an applied mechanical force or acoustic stimulus. It extends conventional grayscale (B-mode) ultrasound by adding a quantitative dimension: how hard or soft tissue is, rather than just what it looks like morphologically.
The fundamental biological rationale: pathological processes alter tissue stiffness. Fibrosis stiffens the liver. Malignant tumors are generally harder than benign lesions. Inflammation alters mechanical compliance. Elastography detects these changes non-invasively.
2. Underlying Physical Principle
The physics of elastography is grounded in the science of continuum mechanics and wave propagation.
Key Physical Concepts
| Concept | Explanation |
|---|---|
| Young's Modulus (E) | Ratio of stress to strain in a material; higher E = stiffer tissue |
| Shear Modulus (G) | Resistance to shear deformation; related to shear wave speed |
| Strain | Fractional deformation of tissue when compressed (ΔL/L) |
| Shear Wave Speed (Vs) | Velocity at which shear waves travel; directly related to stiffness |
| Elastic Modulus / Stiffness | Calculated as E ≈ 3ρVs² (where ρ = tissue density ~1000 kg/m³) |
Stress-Strain Relationship
When mechanical stress is applied to tissue:
- Soft tissue deforms more (high strain, low stiffness)
- Hard tissue deforms less (low strain, high stiffness)
- Shear waves travel faster through stiffer tissue
3. Aim / Goals of Elastography
- Non-invasive tissue characterization — reduce or replace the need for biopsy
- Staging of fibrosis — especially hepatic, renal, splenic fibrosis
- Differentiation of benign vs. malignant lesions — breast, thyroid, prostate, lymph nodes
- Monitoring disease progression and treatment response
- Assessment of inflammatory bowel disease — bowel wall stiffness
- Guiding interventional procedures — targeting the stiffest zone for biopsy
- Real-time intraoperative guidance
4. General Process / Workflow
Patient Positioning
↓
Standard B-mode Ultrasound Acquisition
↓
Selection of Region of Interest (ROI)
↓
Application of Mechanical / Acoustic Stimulus
↓
Detection of Tissue Displacement / Shear Wave
↓
Signal Processing & Computation of Stiffness
↓
Color Map or Quantitative Value Output (kPa or m/s)
↓
Interpretation and Clinical Correlation
Steps in Detail
- Patient preparation: Fasting (typically 4–6 hours for liver), comfortable positioning (supine or lateral decubitus)
- ROI placement: Avoid large vessels, bile ducts, ribs, capsule zones
- Stimulus delivery: Manual compression (strain) or automated acoustic pulse (shear wave)
- Data acquisition: Multiple measurements (minimum 10 for liver), IQR/median ratio <30% for reliability
- Output: Either a color-coded elastogram overlaid on B-mode or a numerical stiffness value (kPa)
- Interpretation: Values compared to validated cutoffs for specific conditions
5. Types of Ultrasound Elastography — In Detail
The two major categories are Strain Elastography (SE) and Shear Wave Elastography (SWE), with SWE subdivided further.
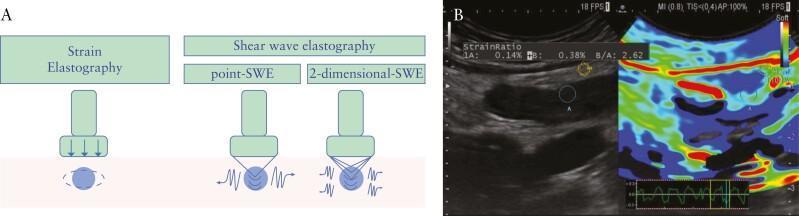
5.1 Strain Elastography (SE) — Compression Elastography
Definition
SE measures the relative deformation (strain) of tissue under an applied external compression force (by the transducer) or internal physiological forces (cardiac pulsation, respiratory motion).
Principle
- Apply gentle, repetitive compression with the transducer
- Measure displacement of tissue before and after compression using speckle tracking or cross-correlation algorithms
- Stiffer tissue = less displacement = low strain value
- Softer tissue = more displacement = high strain value
Technique & Process
- Operator applies gentle rhythmic compression perpendicular to the skin (1–3% compression recommended)
- Real-time RF (radiofrequency) signal data is analyzed frame-by-frame
- A strain map is computed and color-coded (typically: red = soft, blue = hard, though vendor-dependent)
- Stability indicator displayed (waveform at bottom of screen) to guide consistent compression
- Strain Ratio calculated: stiffness of lesion relative to surrounding reference tissue (e.g., SR > 2.5 suggests malignancy in breast)
Output
- Qualitative color map (no absolute units)
- Semi-quantitative Strain Ratio (lesion vs. reference tissue)
Scoring Systems
- Tsukuba Score (1–5) for breast nodules:
- 1: Uniform green (soft, benign)
- 3: Mixed green/blue
- 5: Entirely blue extending beyond lesion (malignant)
Advantages
- Widely available on standard ultrasound machines
- Real-time, no special probe required
- Inexpensive
Limitations
- Operator-dependent (requires consistent compression technique)
- Qualitative/semi-quantitative — no absolute stiffness values
- Cannot penetrate deeply (limited in obese patients)
- Not applicable to cystic or partially cystic lesions (no strain in fluid)
- Cannot be used if lesion is adjacent to bone or calcification
Clinical Applications
| Organ | Use |
|---|---|
| Breast | Differentiation of benign vs. malignant nodules; Tsukuba score |
| Thyroid | Risk stratification of thyroid nodules (limited role per recent data) |
| Liver | Assessment of fibrosis, diffuse liver disease |
| Prostate | Targeting biopsy to stiff zones |
| Bowel | IBD assessment (Crohn's disease fibrosis vs. inflammation) |
| Lymph nodes | Differentiating reactive vs. metastatic nodes |
5.2 Shear Wave Elastography (SWE)
Definition
SWE uses acoustic radiation force or mechanical vibration to generate shear waves within tissue, then measures the propagation speed of those waves. Speed is directly converted to a quantitative stiffness value in kPa.
Key formula:
E = 3ρVs² (E = stiffness in kPa; ρ = tissue density ≈ 1000 kg/m³; Vs = shear wave velocity in m/s)
SWE is further subdivided into three main subtypes:
5.2.1 Transient Elastography (TE) — FibroScan®
Principle
- A mechanical vibrator in the probe tip generates a low-frequency (50 Hz) elastic wave
- An M-mode ultrasound beam tracks the propagation velocity of this shear wave through liver tissue
- Shear wave speed → Liver Stiffness Measurement (LSM) expressed in kPa (range: 2.5–75 kPa)
Technique & Process
- Patient lies supine, right arm raised, right intercostal space exposed
- Probe placed over right liver lobe (intercostal approach)
- System auto-selects a 3 cm² cylindrical sample volume at 25–65 mm depth
- Minimum 10 valid measurements required
- IQR/median ratio < 30% for reliable result
- Success rate and IQR displayed
Probes Available
| Probe | Patient Type | Depth |
|---|---|---|
| S probe | Pediatric (<45 cm thoracic circumference) | Shallow |
| M probe | Adults (skin-to-capsule distance <25 mm) | 25–65 mm |
| XL probe | Obese adults (BMI ≥32 kg/m²) | 35–75 mm |
LSM Cutoffs (Liver Fibrosis — HCV, per EASL)
| Stage | Cutoff (kPa) |
|---|---|
| F0–F1 (No/minimal fibrosis) | <7.0 |
| F2 (Significant fibrosis) | ≥7.0 |
| F3 (Severe fibrosis) | ≥9.5 |
| F4 (Cirrhosis) | ≥12.5 |
Limitations
- Blind technique — no real-time B-mode guidance
- Unreliable in ascites, narrow intercostal spaces
- Confounded by: hepatic inflammation (elevated ALT), congestion, cholestasis, food intake
- Cannot characterize focal lesions
5.2.2 Point Shear Wave Elastography (pSWE) — ARFI (Acoustic Radiation Force Impulse)
Principle
- A focused acoustic push pulse (ARFI — Acoustic Radiation Force Impulse) is delivered to a small ROI within the tissue
- This pulse displaces tissue laterally, generating shear waves
- Two tracking beams placed laterally detect the arrival time of the shear wave → calculate Shear Wave Velocity (SWV) in m/s or convert to kPa
- Integrated into standard B-mode ultrasound transducers (real-time imaging guidance)
Technique & Process
- Real-time B-mode image obtained
- Small ROI (sampling box, ~10 × 5 mm) placed in target tissue under visual guidance
- ARFI push pulse fired
- System calculates SWV (m/s); typically 5–10 measurements averaged
- Can be performed in intercostal, subcostal, or any accessible window
Advantages over TE
- Real-time B-mode guidance — ROI placed with precision
- Applicable to focal lesions and diffuse disease
- Functional in patients with ascites
- Works through intercostal spaces with probe angulation
Output
- SWV in m/s (typical range: 0.5–4.4 m/s in liver)
- Can convert: kPa = SWV² × 3000 / 1000
Clinical Applications
- Liver fibrosis staging (validated against biopsy)
- Kidney stiffness (renal fibrosis, transplant rejection)
- Spleen stiffness (portal hypertension assessment)
- Prostate cancer detection
5.2.3 Two-Dimensional Shear Wave Elastography (2D-SWE)
Principle
- Multiple ARFI push pulses delivered simultaneously across a wide area
- Using ultrafast ultrasound imaging (thousands of frames/second), shear wave propagation is captured across a 2D plane
- Results displayed as a real-time color-coded stiffness map overlaid on B-mode over a large ROI (up to 4×4 cm)
Technique & Process
- B-mode image acquired
- Large ROI box positioned over target area
- Ultrafast imaging captures shear wave propagation in real time
- Color map generated: typically blue = soft, red = hard (vendor-variable)
- User places a virtual sampling box (Q-box) to obtain mean kPa value ± SD within region
- Can sample multiple zones simultaneously
Advantages
- Spatial mapping of stiffness heterogeneity — detects variation within tissue
- Larger area coverage than pSWE
- Highly reproducible, less operator dependent
- Real-time visual feedback
Limitations
- Expensive equipment
- Depth limitations in obese patients
- Susceptible to motion artifacts
- Requires ultrafast hardware not available on all machines
Output
- Color elastogram (kPa scale, color bar displayed)
- Mean kPa ± SD per Q-box
- Statistical distribution over ROI
Key Applications
| Application | Typical Stiffness Findings |
|---|---|
| Normal liver | 2–6 kPa |
| Liver cirrhosis | >12.5 kPa |
| Breast malignancy | Often >80 kPa vs. benign <50 kPa |
| Normal thyroid | ~10–20 kPa |
| Thyroid malignancy | >65–80 kPa |
| Prostate cancer | Stiffness increases in malignant zones |
5.3 Additional / Emerging Types
5.3.1 MR Elastography (MRE) — Hybrid
- Uses MRI with mechanical vibrations; not sonographic but shares principles
- Gold standard for liver fibrosis in many centers
5.3.2 Real-Time Tissue Elastography (RTE)
- Strain-based, integrated into Hitachi systems
- Provides color overlay with live B-mode; used extensively in Japan
5.3.3 Supersonic Shear Imaging (SSI)
- Brand name: Aixplorer® (SuperSonic Imagine)
- Multiple simultaneous acoustic push pulses generating a "Mach cone" shear wave
- Enables ultrafast 2D-SWE with high spatial resolution
6. Comparative Summary Table
| Feature | Strain Elastography | Transient Elastography | Point-SWE (ARFI) | 2D-SWE |
|---|---|---|---|---|
| Stimulus | Manual compression | Mechanical vibrator | Acoustic push pulse | Multiple push pulses |
| Output | Color map / Strain Ratio | LSM (kPa) | SWV (m/s) or kPa | Color map + kPa |
| Quantitative | No (semi-quant) | Yes | Yes | Yes |
| B-mode guidance | Yes | No | Yes | Yes |
| Focal lesion assessment | Yes | No | Yes | Yes |
| Diffuse disease | Limited | Excellent | Good | Good |
| Depth range | Superficial/moderate | 25–75 mm | Any accessible | Moderate |
| Ascites | Difficult | Unreliable | Possible | Possible |
| Operator dependence | High | Moderate | Low–Moderate | Low |
| Cost/Availability | Low | Moderate (dedicated device) | High | High |
| Reproducibility | Moderate | Good | Good | Excellent |
7. Confounding Factors and Pitfalls
| Factor | Effect on Stiffness Reading |
|---|---|
| Hepatic inflammation (high ALT) | Falsely elevated LSM |
| Hepatic congestion / right heart failure | Falsely elevated LSM |
| Postprandial state | Increased hepatic stiffness — fast 4–6 hrs |
| Obesity / deep lesions | Technical failure, underestimation |
| Ascites | TE unreliable; pSWE/2D-SWE possible |
| Breath-holding | Reduces motion artifact — patients should hold breath |
| Excessive compression (strain SE) | Overestimates stiffness |
| Cystic lesions | SE not applicable |
| Calcifications / bone | Reflect/block shear waves |
8. Clinical Utility Summary
| Domain | Recommended Modality | Key Purpose |
|---|---|---|
| Liver fibrosis staging | TE (FibroScan), pSWE, 2D-SWE | Replace/reduce liver biopsy |
| Breast nodule characterization | SE + SWE combined | Downgrade BI-RADS 3–4 lesions |
| Thyroid nodule risk | SE / SWE | Adjunct to ACR TI-RADS (limited evidence) |
| Prostate cancer | SE / pSWE | Target biopsy |
| IBD / Crohn's fibrosis | SE (strain ratio) | Distinguish fibrotic vs. inflammatory stricture |
| Lymph node staging | SE | Differentiate reactive vs. metastatic |
| Portal hypertension | Spleen SWE, Liver SWE | Non-invasive HVPG surrogate |
| Renal transplant | pSWE | Early rejection monitoring |
Key Takeaways
- Elastography measures tissue stiffness, which correlates with pathological changes (fibrosis, malignancy, inflammation)
- Two major categories: Strain Elastography (qualitative, operator-dependent) and Shear Wave Elastography (quantitative, reproducible)
- Shear wave speed is the fundamental measurable: faster propagation = stiffer tissue → higher kPa value
- Transient elastography (FibroScan) remains the most validated tool for liver fibrosis staging globally
- 2D-SWE offers the highest spatial resolution and is increasingly preferred for focal lesion characterization
- Results must always be interpreted in clinical context, accounting for confounders and limitations of each modality
Principle of US elastography
Principle of Ultrasound (US) Elastography
US elastography is based on one core idea:
Disease changes tissue stiffness
- Normal and abnormal tissues have different elasticity.
- Fibrosis, tumors, and chronic inflammation usually make tissue stiffer.
- Some lesions remain soft.
What elastography does
It measures how tissue responds to force:
-
Apply force to tissue
- Manual compression (strain elastography), or
- Acoustic push pulse/mechanical vibration (shear wave methods)
-
Measure tissue response
- Either amount of deformation (strain), or
- Speed of generated shear waves
-
Convert response to stiffness map/value
- Soft tissue: deforms more, shear waves travel slower
- Hard tissue: deforms less, shear waves travel faster
Physics summary
- In shear wave elastography, tissue stiffness is related to shear wave velocity: [ E \approx 3\rho V_s^2 ] Where:
- (E) = elastic (Young’s) modulus (kPa)
- (\rho) = tissue density
- (V_s) = shear wave speed (m/s)
So, higher (V_s) means higher stiffness.
Two practical principles used clinically
- Strain elastography: relative stiffness (qualitative/semi-quantitative)
- Shear wave elastography: absolute stiffness (quantitative, m/s or kPa)
If you want, I can also give this as a neat exam-style flowchart (very useful for viva answers).
This is a shared conversation. Sign in to Orris to start your own chat.