anemia case medicine pre sentation
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is your complete medicine case presentation on Anemia for MBBS students, drawn directly from Harrison's, Robbins & Kumar, and Goldman-Cecil Medicine.
🩸 ANEMIA - Full Clinical Case Presentation
Medicine | MBBS Level
PART 1 - OVERVIEW & DEFINITION
Anemia is defined as blood counts below normal for a given population. In practical terms:
- Males: Hb < 13.5 g/dL
- Females: Hb < 12.0 g/dL
- Pregnant women: Hb < 11.0 g/dL
PART 2 - CLASSIFICATION
A. By Red Cell Size (MCV-Based - Wintrobe's Classification)
| Type | MCV | Causes |
|---|---|---|
| Microcytic | < 80 fL | Iron deficiency, Thalassemia, Anemia of chronic disease, Sideroblastic anemia |
| Normocytic | 80-100 fL | Aplastic anemia, Hemolytic anemia, Acute blood loss, CKD, Endocrinopathies |
| Macrocytic | > 100 fL | Vit B12/Folate deficiency (oval macrocytes), Liver disease, Alcohol, Hypothyroidism (round macrocytes) |
B. By Mechanism (Pathophysiologic Classification)
(Robbins, Cotran & Kumar - Pathologic Basis of Disease)
| Mechanism | Examples |
|---|---|
| Blood loss | Acute trauma, GI bleed, menorrhagia |
| Increased destruction (Hemolysis) | G6PD deficiency, sickle cell disease, autoimmune hemolytic anemia, malaria, PNH |
| Decreased production | Iron deficiency, B12/folate deficiency, aplastic anemia, CKD, myelophthisic anemia |
C. By Reticulocyte Count (Key Clinical Tool)
- Elevated reticulocytes → Hemolysis OR blood loss (marrow is responding)
- Low reticulocytes → Decreased production (marrow failure)
PART 3 - CLINICAL FEATURES (Common to All Anemias)
Symptoms:
- Fatigue, easy fatigability
- Dyspnea on exertion
- Palpitations
- Headache, dizziness
- Reduced exercise tolerance
Signs:
- Pallor (conjunctiva, palms, nail beds)
- Tachycardia
- Flow murmur (ejection systolic, best heard at pulmonary area)
- In severe cases: cardiac failure, angina
CASE 1 - IRON DEFICIENCY ANEMIA
Clinical Vignette
A 26-year-old woman presents with 3 months of progressive fatigue, breathlessness on climbing stairs, and pica (craving for ice and chalk). She has heavy menstrual periods (soaking >5 pads/day). On exam: pallor of conjunctiva and palms, angular cheilitis, smooth tongue (atrophic glossitis). No splenomegaly.
Investigation Results
| Test | Result | Interpretation |
|---|---|---|
| Hb | 7.2 g/dL | Low |
| MCV | 65 fL | Microcytic |
| MCH | 18 pg | Hypochromic |
| Serum Iron | 30 µg/dL | Low |
| TIBC | 480 µg/dL | High (↑ transferrin) |
| Transferrin saturation | 6% | Low (normal >15%) |
| Serum Ferritin | 4 µg/L | Low (normal >12 µg/L) |
| Reticulocytes | Low-normal | Decreased production |
Peripheral Blood Smear

Pathophysiology (Robbins)
- Cause: Chronic blood loss (menorrhagia) → depletes storage iron (ferritin) → depletes transport iron → hemoglobin synthesis fails
- Normal diet: 10-20 mg/day; absorb 1-2 mg; women need 7-20 mg/day
- Heme iron (from meat) absorbed 20% vs non-heme iron only 1-2%
- Hepcidin falls in iron deficiency → attempts to maximize absorption
- Bone marrow: erythroid hyperplasia with absent iron stores (Prussian blue stain negative)
Treatment
- Oral ferrous sulfate: 150-200 mg elemental iron/day in divided doses (fasting or with Vit C)
- Reticulocytosis begins in 5-7 days
- Full correction takes 4-6 weeks; continue for 3 months to replenish stores
- Treat the cause (manage menorrhagia)
Examination Questions
Q1. What is the single most useful test to diagnose iron deficiency?
Serum ferritin - it directly reflects iron stores. Values < 12 µg/L are diagnostic.
Q2. Why is TIBC elevated in IDA?
The liver produces more transferrin when iron is deficient to capture any available iron. More "empty" transferrin = elevated TIBC.
Q3. Name four causes of microcytic anemia.
Iron deficiency, Thalassemia, Anemia of chronic disease/inflammation, Sideroblastic anemia (mnemonic: TAILS - Thalassemia, Anemia of chronic disease, Iron deficiency, Lead poisoning, Sideroblastic)
Q4. What is Plummer-Vinson syndrome?
Triad of: microcytic hypochromic anemia + atrophic glossitis + esophageal webs. Associated with long-standing severe iron deficiency. Risk factor for postcricoid carcinoma.
CASE 2 - MEGALOBLASTIC ANEMIA (Vitamin B12 Deficiency)
Clinical Vignette
A 55-year-old vegetarian man presents with fatigue, sore tongue, and tingling/numbness in both feet and hands (glove-and-stocking pattern). He had a gastrectomy 10 years ago. On exam: pallor, mild jaundice (lemon-yellow tinge), smooth beefy red tongue, loss of vibration sense and proprioception in lower limbs bilaterally.
Investigation Results
| Test | Result |
|---|---|
| Hb | 8.4 g/dL |
| MCV | 115 fL (macrocytic) |
| Serum B12 | 85 pg/mL (low; normal 200-900) |
| Serum Folate | Normal |
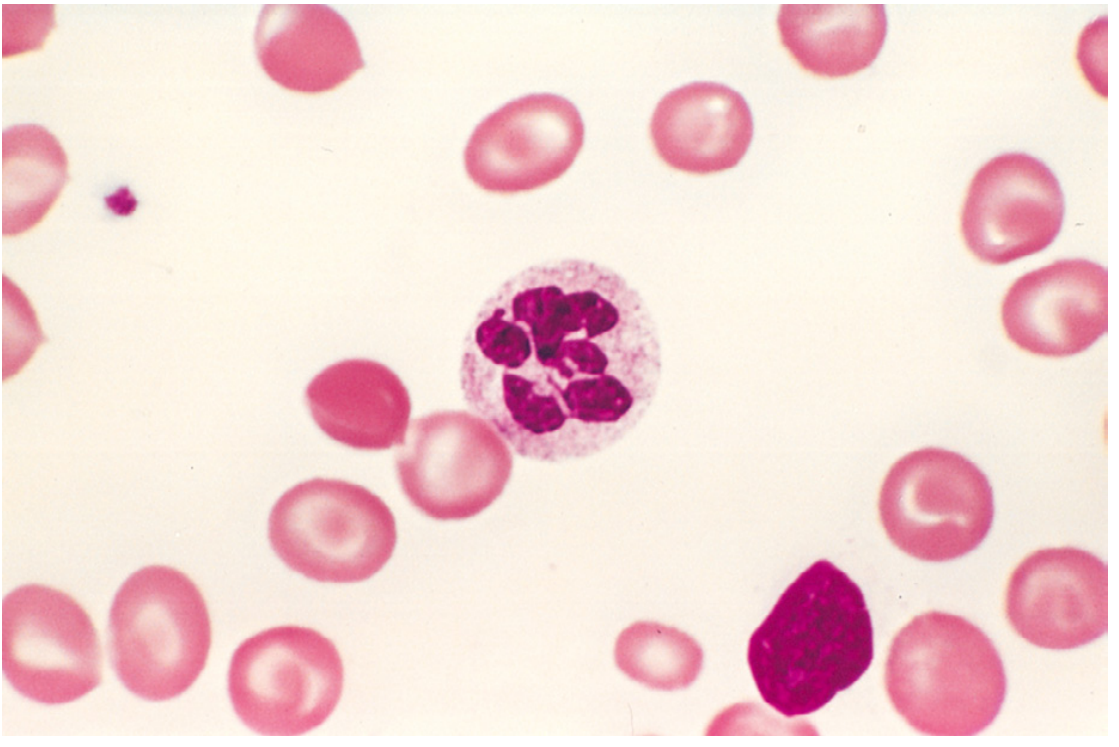
| Peripheral smear | Macro-ovalocytes, hypersegmented neutrophils (>5 lobes) |
| LDH | Elevated |
| Indirect bilirubin | Mildly elevated |
| Anti-intrinsic factor antibodies | Positive |
| Schilling test | Abnormal (corrected by intrinsic factor) |
Morphology (Robbins)
- Peripheral blood: macro-ovalocytes (large oval RBCs without central pallor), hypersegmented neutrophils (5+ lobes - pathognomonic)
- Bone marrow: hypercellular with megaloblasts (nuclear-cytoplasmic asynchrony - cytoplasm matures but nucleus remains immature)
- Giant metamyelocytes and band forms
Pathophysiology
- B12 required for: thymidine synthesis (DNA) + conversion of methylmalonyl CoA → succinyl CoA (myelin)
- Intrinsic factor secreted by gastric parietal cells - required for B12 absorption in terminal ileum
- Gastrectomy → loss of parietal cells → no IF → no B12 absorption (Pernicious anemia if autoimmune)
- DNA synthesis impaired → ineffective erythropoiesis → pancytopenia + intramedullary hemolysis (elevated LDH and indirect bilirubin)
- Subacute combined degeneration of spinal cord: B12 deficiency causes demyelination of posterior columns (vibration/proprioception) + lateral corticospinal tracts (UMN signs)
Treatment
- IM Cyanocobalamin/Hydroxocobalamin: 1000 µg daily × 7 days → weekly × 4 → monthly (lifelong)
- Oral B12 1000 µg/day (for dietary deficiency)
- Important: Must rule out B12 deficiency before giving folate alone (folate can correct anemia but WILL NOT prevent/may worsen neurological damage)
Examination Questions
Q1. What is the classic peripheral smear finding in megaloblastic anemia?
Hypersegmented neutrophils (≥5 lobes in >5% of neutrophils, or any neutrophil with ≥6 lobes) AND macro-ovalocytes.
Q2. B12 vs Folate deficiency - how do you differentiate?
Neurological features (subacute combined degeneration) occur only in B12 deficiency. Check serum B12, folate, and methylmalonic acid (elevated in B12 deficiency only).
Q3. What is nuclear-cytoplasmic asynchrony?
In megaloblasts, DNA synthesis is impaired so the nucleus remains large and immature while the cytoplasm continues to mature normally (accumulates hemoglobin). The nucleus appears "young" for the age of the cell.
Q4. Why does pernicious anemia cause jaundice?
Ineffective erythropoiesis leads to intramedullary hemolysis (destruction of megaloblasts in the bone marrow before they enter circulation), releasing bilirubin → elevated indirect bilirubin and LDH.
CASE 3 - HEMOLYTIC ANEMIA
Clinical Vignette
A 19-year-old male student develops sudden onset of dark urine, jaundice, and pallor 2 days after taking primaquine for malaria prophylaxis. His urine appears dark brown ("Coca-Cola colored"). No splenomegaly. His maternal uncle had a similar episode.
Investigation Results
| Test | Result |
|---|---|
| Hb | 6.1 g/dL |
| MCV | 90 fL (normocytic) |
| Reticulocytes | 12% (markedly elevated) |
| Peripheral smear | "Bite cells" (eccentrocytes), Heinz bodies (supravital stain) |
| Indirect bilirubin | Elevated |
| LDH | Elevated |
| Serum Haptoglobin | Low/absent |
| Urinalysis | Hemoglobinuria |
| G6PD assay | Deficient |
| Coombs test | Negative |
Pathophysiology (Robbins)
Extravascular vs Intravascular Hemolysis:
| Feature | Extravascular | Intravascular |
|---|---|---|
| Site | Spleen (macrophages) | Blood vessels |
| Splenomegaly | Yes | No/mild |
| Hemoglobinuria | No | Yes |
| Hemoglobinemia | No | Yes |
| Haptoglobin | Low | Very low/absent |
| Jaundice | Yes | Yes |
| Causes | Spherocytosis, Warm AIHA, sickle cell | G6PD deficiency (severe), PNH, TTP/HUS, mechanical valves |
G6PD Deficiency mechanism:
- X-linked recessive (more common in males)
- G6PD needed to regenerate glutathione (protects RBCs from oxidative damage)
- Oxidant stress (primaquine, dapsone, fava beans, infections) → hemoglobin oxidation → Heinz bodies → RBC destruction
Treatment
- Withdraw precipitating drug
- Transfusion if severe
- Folic acid supplementation
- Avoid triggers (oxidant drugs, fava beans)
Examination Questions
Q1. What distinguishes intravascular from extravascular hemolysis?
Intravascular: hemoglobinuria, hemoglobinemia, very low haptoglobin. Extravascular: splenomegaly, jaundice (no free hemoglobin in urine).
Q2. Name the hallmark labs for all hemolytic anemias.
Elevated reticulocytes, elevated indirect bilirubin, elevated LDH, low haptoglobin, +/- peripheral smear evidence of hemolysis.
Q3. What is a Coombs test and when is it positive?
Direct Coombs (DAT) detects antibodies/complement on RBC surface - positive in autoimmune hemolytic anemia (AIHA), hemolytic transfusion reactions, drug-induced hemolysis.
Q4. Classify hemolytic anemia into intrinsic vs extrinsic causes.
Intrinsic (intracorpuscular): G6PD deficiency, pyruvate kinase deficiency, hereditary spherocytosis, sickle cell disease, thalassemia, PNH. Extrinsic (extracorpuscular): AIHA, malaria, microangiopathic HA (TTP, HUS, DIC), mechanical valves.
CASE 4 - APLASTIC ANEMIA
Clinical Vignette
A 22-year-old male presents with 6 weeks of progressive fatigue, spontaneous bruising over his limbs, recurrent oral ulcers, and a 5-day history of high fever not responding to antibiotics. He took carbamazepine for 3 months. On exam: pallor, scattered petechiae and ecchymoses, no splenomegaly, no lymphadenopathy.
Investigation Results
| Test | Result |
|---|---|
| Hb | 5.8 g/dL |
| WBC | 1.2 × 10⁹/L (neutrophils < 500/µL) |
| Platelets | 8 × 10⁹/L |
| Reticulocytes | <0.1% (severely reduced) |
| MCV | Normal |
| Peripheral smear | Pancytopenia, no abnormal cells |
| Bone marrow biopsy | Hypocellular marrow with > 90% fat cells - diagnostic |
| Flow cytometry | No PNH clone |
Pathophysiology (Robbins & Kumar)
- Multipotent myeloid stem cells are suppressed → bone marrow failure → pancytopenia
- Immune-mediated (most common): Activated T cells produce cytokines → suppress hematopoietic progenitors. Evidence: 60-70% respond to immunosuppression
- Intrinsic stem cell defect: Telomerase defects in 5-10%; shortened telomeres → premature stem cell senescence
- Causes: Idiopathic (most common), drugs (carbamazepine, chloramphenicol, NSAIDs, gold), viruses (hepatitis, EBV, CMV, parvovirus B19), radiation, chemicals (benzene)
- No splenomegaly - if spleen is enlarged, consider another diagnosis
Severity Classification (Camitta Criteria)
| Grade | Criteria |
|---|---|
| Severe | Bone marrow cellularity <25% + 2 of: neutrophils <500/µL, platelets <20,000/µL, reticulocytes <20,000/µL |
| Very severe | Same + neutrophils <200/µL |
| Moderate | Does not meet severe criteria |
Treatment
- Age < 40, HLA-matched sibling: Allogeneic stem cell transplantation (curative)
- No matched donor / age > 40: Antithymocyte globulin (ATG) + Cyclosporin + Eltrombopag (immunosuppression)
- Supportive: packed RBC transfusion, platelet transfusion, antibiotics
- Minimize transfusions in transplant candidates (allosensitization → graft failure)
Examination Questions
Q1. What is the gold standard investigation for aplastic anemia?
Bone marrow biopsy - shows hypocellular marrow with >90% fat cells and absent/markedly reduced hematopoietic elements.
Q2. What triad of symptoms suggests aplastic anemia?
Anaemia (pallor, fatigue) + thrombocytopenia (petechiae, bruising, bleeding) + neutropenia (recurrent infections, fever). This is pancytopenia.
Q3. Differentiate aplastic anemia from acute leukemia presenting with pancytopenia.
Both cause pancytopenia. Leukemia: hepatosplenomegaly, lymphadenopathy, circulating blasts on smear, hypercellular marrow with blasts. Aplastic anemia: no organomegaly, no blasts, hypocellular fatty marrow.
Q4. Why should transfusions be minimized in aplastic anemia patients eligible for transplant?
Transfusions sensitize the patient to HLA antigens (allosensitization), greatly increasing the risk of graft rejection after stem cell transplantation.
PART 4 - COMPARISON TABLE: THE BIG 4 ANEMIAS
| Feature | IDA | Megaloblastic | Hemolytic | Aplastic |
|---|---|---|---|---|
| MCV | ↓ Micro | ↑ Macro | Normal | Normal |
| Hb | ↓ | ↓ | ↓ | ↓ |
| WBC | Normal | ↓ (in severe) | Normal | ↓↓ |
| Platelets | Normal | ↓ (in severe) | Normal (or ↓ in TTP) | ↓↓ |
| Reticulocytes | ↓ | ↓ | ↑↑ | ↓↓ |
| LDH | Normal | ↑↑ | ↑↑ | Normal |
| Bilirubin (indirect) | Normal | ↑ | ↑ | Normal |
| Haptoglobin | Normal | Normal/↓ | ↓↓ | Normal |
| Ferritin | ↓↓ | Normal | Normal/↑ | Normal |
| Serum B12 | Normal | ↓ | Normal | Normal |
| Bone marrow | Erythroid hyperplasia, no Fe stores | Megaloblasts, hypercellular | Erythroid hyperplasia | Hypocellular, fatty |
| Smear clue | Hypochromic, microcytic, pencil cells | Macro-ovalocytes, hyperseg. neutrophils | Spherocytes/bite cells/sickle cells | Pancytopenia, no abnormal morphology |
PART 5 - HIGH-YIELD MNEMONICS
Microcytic anemia (TAILS):
Thalassemia, Anemia of chronic disease, Iron deficiency, Lead poisoning, Sideroblastic anemia
Causes of aplastic anemia (DRIFTS):
Drugs, Radiation, Infections (viral), Fanconi anemia, Toxins (benzene), Spontaneous (idiopathic)
Hemolysis labs (5 H's):
High reticulocytes, High LDH, High indirect bilirubin, Haptoglobin low, Hemoglobinuria (intravascular)
PART 6 - EXAM SPOTTERS
| Finding | Diagnosis |
|---|---|
| Hypersegmented neutrophils | Megaloblastic anemia |
| Pencil cells + hypochromic microcytes | IDA |
| Bite cells + Heinz bodies | G6PD deficiency |
| Positive direct Coombs | Autoimmune hemolytic anemia |
| Hypocellular marrow + pancytopenia + no spleen | Aplastic anemia |
| Koilonychia + pica + angular cheilitis | IDA |
| Subacute combined degeneration | B12 deficiency |
| Lemon-yellow jaundice + macrocytic anemia | Megaloblastic anemia |
| Target cells + microcytosis | Thalassemia |
| Schistocytes (fragments) | Microangiopathic HA (TTP/HUS/DIC) |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine
case p refoma
Asking for Preferences
Here are all 4 complete clinical case proformas for Anemia, formatted as they would appear in a bedside/ward case write-up.
CLINICAL CASE PROFORMA
Department of Medicine | MBBS Undergraduate Teaching
PROFORMA 1 - IRON DEFICIENCY ANEMIA
Date: ___________
Posting: Medicine
Bed No.: ___________
Case No.: ___________
PATIENT IDENTIFICATION
| Name | Mrs. Sunita Devi |
| Age / Sex | 26 years / Female |
| Occupation | Homemaker |
| Address | Rural, UP |
| Religion | Hindu |
| Informant | Self (reliable) |
CHIEF COMPLAINTS
- Fatigue and weakness - 3 months
- Breathlessness on exertion (climbing stairs) - 2 months
- Craving for ice and chalk (pica) - 1 month
- Excessive menstrual bleeding - 6 months
HISTORY OF PRESENT ILLNESS
Patient was apparently well 6 months ago. She then began to notice heavy menstrual periods, soaking more than 5 pads per day. Over the next 3 months she developed gradually worsening fatigue, inability to perform household work, and breathlessness on climbing 1 flight of stairs. She has no breathlessness at rest. Over the past month she developed a craving for ice (pagophagia) and chalk. She also noticed hairfall, soreness of the tongue, and painful cracks at the corners of her mouth.
No chest pain, orthopnoea, PND, palpitations at rest, edema, hematemesis, melena, or hematuria.
PAST HISTORY
- Similar illness: No prior episodes
- Medical: No known DM, HTN, thyroid disease
- Surgical: No prior operations
- Drug history: No NSAIDs, antacids, tetracyclines
- Allergy: Nil known
OBSTETRIC & MENSTRUAL HISTORY
- LMP: ___________
- Cycle: Irregular, heavy (menorrhagia), 8-10 days duration
- Married × 4 years; G2P2L2; last delivery 18 months ago (normal vaginal delivery)
- No current pregnancy
DIETARY HISTORY
- Predominantly vegetarian; rarely eats meat
- Low fruit and vegetable intake
- Drinks 3-4 cups of tea daily (tannins reduce iron absorption)
FAMILY HISTORY
No similar illness in family. No history of thalassemia or hemolytic disorders.
PERSONAL HISTORY
- Diet: Vegetarian, inadequate
- Sleep: Reduced (fatigue)
- Bowel/Bladder: Normal
- Appetite: Decreased
- Addiction: Nil
GENERAL PHYSICAL EXAMINATION
| Finding | Result |
|---|---|
| Built & Nourishment | Thin, poorly nourished |
| Pallor | Present (+++): conjunctivae, palms, nail beds |
| Icterus | Absent |
| Cyanosis | Absent |
| Clubbing | Absent |
| Lymphadenopathy | Absent |
| Edema | Trace pedal edema |
| Koilonychia | Present (spoon-shaped nails) |
| Angular cheilitis | Present |
| Atrophic glossitis | Present (smooth, shiny tongue) |
| Alopecia | Present |
| Pulse | 104/min, regular, low volume |
| BP | 100/70 mmHg |
| RR | 18/min |
| Temperature | Afebrile |
| SpO2 | 98% on room air |
SYSTEMIC EXAMINATION
Cardiovascular:
- Apex beat: 5th ICS, MCL (shifted - hyperdynamic)
- S1, S2 heard; ejection systolic flow murmur at pulmonary area (grade 2/6)
- No diastolic murmur
Respiratory: Clear; no added sounds
Abdomen:
- Soft, non-tender
- No hepatomegaly; No splenomegaly
- No ascites
CNS: No neurological deficits
INVESTIGATIONS
Hemogram:
| Value | Normal | |
|---|---|---|
| Hb | 7.2 g/dL | 12-16 |
| TLC | 7,200/µL | 4000-11000 |
| PLC | 4.2 lakhs/µL | Normal |
| MCV | 65 fL | 80-100 |
| MCH | 18 pg | 27-33 |
| MCHC | 25 g/dL | 32-36 |
| RDW | 18% (elevated) | <14.5% |
| Reticulocyte count | 0.8% | Normal |
Iron Studies:
| Test | Value | Normal |
|---|---|---|
| Serum Iron | 30 µg/dL | 60-170 |
| TIBC | 480 µg/dL | 250-370 |
| Transferrin saturation | 6% | 20-50% |
| Serum Ferritin | 4 µg/L | 12-150 |
Peripheral blood smear:
- Hypochromic, microcytic RBCs
- Large zone of central pallor (>1/3 cell diameter)
- Pencil cells (elongated elliptocytes)
- Anisocytosis and poikilocytosis
- No abnormal WBCs or platelets
Other investigations:
- Stool for occult blood: Negative
- USG Pelvis: Bulky uterus (fibroid)
- Serum folate/B12: Normal
- RBS: Normal
DIAGNOSIS
Provisional: Iron Deficiency Anemia (moderate severity), secondary to menorrhagia (uterine fibroid)
Differential Diagnoses:
- Thalassemia trait (but normal Hb electrophoresis + positive family history expected)
- Anemia of chronic disease (but TIBC would be low, not high)
- Sideroblastic anemia (rare; ring sideroblasts on marrow)
Final Diagnosis: Iron Deficiency Anemia (microcytic hypochromic, moderate) secondary to menorrhagia
TREATMENT
| Tab Ferrous Sulfate | 200 mg TDS with Vitamin C, before meals × 3 months |
| Tab Folic acid | 5 mg OD × 4 months |
| Diet counselling | Increase iron-rich foods; avoid tea with meals |
| Refer Gynaecology | Management of fibroid/menorrhagia |
| Monitoring | Reticulocyte count at day 7; repeat Hb at 4 weeks |
PROGNOSIS
Good with treatment of underlying cause and adequate iron supplementation.
PROFORMA 2 - MEGALOBLASTIC ANEMIA (B12 DEFICIENCY / PERNICIOUS ANEMIA)
Date: ___________
Bed No.: ___________
PATIENT IDENTIFICATION
| Name | Mr. Ramesh Kumar |
| Age / Sex | 55 years / Male |
| Occupation | Farmer |
| Diet | Strict vegetarian (vegan) for 20 years |
CHIEF COMPLAINTS
- Fatigue, weakness - 4 months
- Tingling and numbness in both hands and feet - 2 months
- Difficulty walking, unsteadiness - 6 weeks
- Sore, burning tongue - 1 month
- Mild yellowish discoloration of skin - 1 month
HISTORY OF PRESENT ILLNESS
Mr. Ramesh is a 55-year-old male, strict vegetarian, who underwent subtotal gastrectomy for peptic ulcer disease 10 years ago. He presents with 4 months of progressive fatigue. Over the last 2 months he developed tingling and numbness in a glove-and-stocking distribution. He has difficulty walking in the dark and has fallen twice. Tongue pain makes eating difficult. His wife noticed a lemon-yellow tinge to his skin. No blood in stools, no significant weight loss, no diarrhea.
PAST HISTORY
- Subtotal gastrectomy 10 years ago (peptic ulcer)
- No DM, HTN, thyroid disease
- No long-term medications
- No alcohol or smoking
GENERAL PHYSICAL EXAMINATION
| Finding | Result |
|---|---|
| Built & Nourishment | Average |
| Pallor | Present (+++) |
| Icterus | Present (mild, lemon-yellow tinge) |
| Cyanosis | Absent |
| Clubbing | Absent |
| Lymphadenopathy | Absent |
| Edema | Absent |
| Glossitis | Present (beefy red, smooth tongue) |
| Pulse | 96/min, regular |
| BP | 118/76 mmHg |
| Temperature | Afebrile |
SYSTEMIC EXAMINATION
Cardiovascular: Flow murmur at pulmonary area; No organically significant murmur
Abdomen: Soft; no hepatomegaly; no splenomegaly
CNS - KEY FINDINGS:
| Neurological Test | Finding |
|---|---|
| Vibration sense (128 Hz tuning fork) | Absent at great toe and ankle bilaterally |
| Proprioception (position sense) | Absent at toes bilaterally |
| Romberg's test | Positive (falls with eyes closed) |
| Heel-shin test | Impaired |
| Power | Normal |
| Tone | Slightly increased (bilateral lower limbs) |
| Knee jerks | Brisk (+++) |
| Plantar response | Extensor (bilateral Babinski positive) |
| Sensory examination | Glove-and-stocking hypoesthesia |
Impression: Subacute combined degeneration of spinal cord (posterior column + lateral corticospinal tract involvement)
INVESTIGATIONS
Hemogram:
| Value | Normal | |
|---|---|---|
| Hb | 8.4 g/dL | Low |
| TLC | 3,200/µL | Low |
| PLC | 85,000/µL | Low |
| MCV | 115 fL | High (macrocytic) |
| MCH | 38 pg | High |
| Reticulocytes | 0.5% | Low |
Special Tests:
| Test | Value | Normal |
|---|---|---|
| Serum Vit B12 | 85 pg/mL | 200-900 |
| Serum Folate | 8 ng/mL | Normal |
| Serum Iron | Normal | |
| Serum Ferritin | Normal | |
| LDH | 1200 U/L | <250 (elevated) |
| Indirect bilirubin | 2.1 mg/dL | Elevated |
| Direct bilirubin | 0.3 mg/dL | Normal |
| Anti-intrinsic factor Ab | Positive | Diagnostic of pernicious anemia |
| Anti-parietal cell Ab | Positive | |
| Methylmalonic acid | Elevated | Specific for B12 deficiency |
Peripheral Blood Smear:
- Macro-ovalocytes (large oval RBCs without central pallor)
- Hypersegmented neutrophils (>5 lobes; some with 6-7 lobes)
- Anisocytosis, poikilocytosis
- Thrombocytopenia (large platelets)
Bone Marrow (if done):
- Hypercellular
- Megaloblasts (nuclear-cytoplasmic asynchrony)
- Giant metamyelocytes and band forms
MRI Spine: T2 hyperintensity in posterior and lateral columns (cervicothoracic region)
DIAGNOSIS
Provisional: Megaloblastic anemia with subacute combined degeneration of spinal cord - secondary to Vitamin B12 deficiency
Cause: Pernicious anemia (anti-IF antibodies positive) + post-gastrectomy (loss of parietal cells) + strict vegetarian diet
Differential Diagnoses:
- Folate deficiency (no neurological features; folate normal here)
- Myelodysplastic syndrome (but normal morphology of blasts expected; rule out with marrow)
- Hypothyroid macrocytosis (check TFTs)
TREATMENT
| Drug | Dose | Route | Duration |
|---|---|---|---|
| Hydroxocobalamin | 1000 µg daily | IM | × 7 days |
| Then 1000 µg weekly | IM | × 4 weeks | |
| Then 1000 µg monthly | IM | Lifelong | |
| Folic acid | 5 mg OD | Oral | × 4 months |
| Physiotherapy | For gait rehabilitation |
Important: Never give folate alone without correcting B12 - folate corrects the anemia but WORSENS the neurological damage.
PROGNOSIS
- Hematological response begins within 1 week
- Neurological recovery: variable; depends on duration (may not fully reverse if > 6 months)
- Lifelong B12 replacement required
PROFORMA 3 - HEMOLYTIC ANEMIA (G6PD DEFICIENCY)
Date: ___________
Bed No.: ___________
PATIENT IDENTIFICATION
| Name | Mr. Arjun Singh |
| Age / Sex | 19 years / Male |
| Occupation | Student |
| Family history | Maternal uncle had similar episode |
CHIEF COMPLAINTS
- Dark brown urine (hemoglobinuria) - 2 days
- Yellowish discoloration of eyes - 2 days
- Fatigue and pallor - 2 days
- Drug intake: Primaquine started 3 days ago
HISTORY OF PRESENT ILLNESS
A 19-year-old male student was started on primaquine 3 days ago for malaria prophylaxis before a trip. Two days later he developed sudden dark brown ("Coca-Cola/tea-colored") urine, yellow discoloration of eyes, and severe fatigue. No prior similar episode personally, but his maternal uncle had a similar episode years ago after taking a sulfa drug. No fever, no abdominal pain, no recent infections. No hematuria (distinct from hemoglobinuria - no RBCs in urine).
PAST HISTORY
- No prior anemia or transfusion
- No DM, thyroid disease
- No chronic medications
- Family history: Maternal uncle - similar episode with sulfa drug
GENERAL PHYSICAL EXAMINATION
| Finding | Result |
|---|---|
| Pallor | Present (+++) |
| Icterus | Present (+++) |
| Cyanosis | Absent |
| Clubbing | Absent |
| Lymphadenopathy | Absent |
| Edema | Absent |
| Pulse | 110/min, regular |
| BP | 106/72 mmHg |
| Temperature | 37.2°C (afebrile) |
SYSTEMIC EXAMINATION
Abdomen:
- Liver: Not palpable
- Spleen: Not palpable (intravascular hemolysis - spleen not involved)
- No ascites
CVS: Tachycardia; flow murmur; no significant findings
CNS: Normal
INVESTIGATIONS
Hemogram:
| Value | |
|---|---|
| Hb | 6.1 g/dL |
| TLC | 11,000/µL (mild leukocytosis - stress response) |
| PLC | 1.8 lakhs/µL (normal) |
| MCV | 90 fL (normocytic) |
| Reticulocyte count | 12% (markedly elevated) |
Hemolysis Panel:
| Test | Value | Interpretation |
|---|---|---|
| LDH | 2400 U/L | Elevated (cell lysis) |
| Indirect bilirubin | 4.8 mg/dL | Elevated (Hb breakdown) |
| Direct bilirubin | 0.4 mg/dL | Normal |
| Serum Haptoglobin | Absent | Diagnostic of hemolysis |
| Plasma Hb | Elevated | Intravascular hemolysis |
| Direct Coombs (DAT) | Negative | Rules out AIHA |
Urinalysis:
- Color: Dark brown
- Hemoglobin: Positive (hemoglobinuria)
- RBCs: Absent (distinguishes from hematuria)
- Hemosiderin: Present
Peripheral Blood Smear:
- "Bite cells" (eccentrocytes) - RBCs with Hb pushed to one side
- Blister cells
- Polychromasia (reticulocytes)
- Heinz bodies visible on supravital stain (brilliant cresyl blue)
- No spherocytes; No sickle cells
Confirmatory Test:
- G6PD quantitative assay: Severely deficient (< 10% of normal)
- Note: Test should be repeated 6-8 weeks after acute episode (reticulocytes have normal G6PD activity - may give falsely normal result in acute phase)
Hemoglobin electrophoresis: Normal (rules out hemoglobinopathy)
DIAGNOSIS
Provisional: Acute intravascular hemolytic anemia secondary to G6PD deficiency, precipitated by primaquine
Differential Diagnoses:
- Autoimmune hemolytic anemia (Coombs negative here - excluded)
- Paroxysmal nocturnal hemoglobinuria - PNH (flow cytometry for CD55/CD59 - negative here)
- Sickle cell crisis (no sickle cells on smear; Hb electrophoresis normal)
- Glucose-6-phosphate isomerase deficiency (very rare)
PATHOPHYSIOLOGY (Brief)
G6PD (X-linked recessive) → Deficiency → Oxidative stress from primaquine → Glutathione depleted → Hb oxidized → Heinz body formation → RBC membrane damage → Intravascular hemolysis → Hemoglobinemia/uria
TREATMENT
| Action | Details |
|---|---|
| Stop primaquine immediately | Primary intervention |
| IV fluids | Hydration to protect kidneys from Hb precipitation |
| Blood transfusion | If Hb < 7 or symptomatic (given 1 unit pRBC) |
| Folic acid | 5 mg OD (to support erythropoiesis) |
| Monitor renal function | Hemoglobin in tubules → acute tubular necrosis risk |
| Patient education | Avoid: primaquine, dapsone, nitrofurantoin, sulfonamides, fava beans, high-dose Vit C, mothballs (naphthalene) |
| Screen family | X-linked recessive → screen brothers and maternal relatives |
PROGNOSIS
- Acute episode is self-limiting (once offending drug withdrawn)
- Hb recovers in 3-4 weeks
- Future episodes preventable by avoiding oxidant triggers
- No chronic hemolysis in the Mediterranean/African G6PD variants (WHO Class II/III)
PROFORMA 4 - APLASTIC ANEMIA
Date: ___________
Bed No.: ___________
PATIENT IDENTIFICATION
| Name | Mr. Vikram Sharma |
| Age / Sex | 22 years / Male |
| Occupation | College student |
| Drug history | Carbamazepine × 3 months (for seizures) |
CHIEF COMPLAINTS
- Progressive fatigue, pallor - 6 weeks
- Spontaneous bruising over limbs - 4 weeks
- Recurrent mouth ulcers - 3 weeks
- High-grade fever, not responding to antibiotics - 5 days
- Gum bleeding on brushing - 2 weeks
HISTORY OF PRESENT ILLNESS
A 22-year-old male was diagnosed with epilepsy 4 months ago and started on carbamazepine 200 mg TDS. Six weeks ago he noticed progressive fatigue and pallor. Four weeks later he developed spontaneous bruising on arms and legs without any trauma, followed by recurrent painful oral ulcers. He has had high fever (101-103°F) for the last 5 days not responding to oral antibiotics. He noticed bleeding from gums on brushing. No hematemesis, melena, hematuria. No weight loss. No sick contacts. No recent travel.
PAST HISTORY
- Epilepsy (idiopathic, generalized tonic-clonic)
- No prior blood disorders or transfusions
- No DM, HTN, infections (hepatitis, HIV negative on testing)
- No exposure to radiation or industrial chemicals
FAMILY HISTORY
- No similar illness in family
- No consanguinity
- No known hematological disorders
GENERAL PHYSICAL EXAMINATION
| Finding | Result |
|---|---|
| Pallor | Present (+++) - conjunctivae, tongue, palms |
| Icterus | Absent |
| Cyanosis | Absent |
| Clubbing | Absent |
| Lymphadenopathy | Absent |
| Petechiae | Present over both arms and legs |
| Ecchymoses | Present (multiple, spontaneous) |
| Oral mucosa | Hemorrhagic bullae, ulcers |
| Pulse | 102/min, regular |
| BP | 110/74 mmHg |
| Temperature | 38.9°C (febrile) |
| SpO2 | 97% room air |
SYSTEMIC EXAMINATION
Abdomen:
- Liver: Not palpable
- Spleen: Not palpable ← CRITICAL FINDING
- No ascites, no lymphadenopathy in abdomen
CVS: Tachycardia; flow murmur grade 2/6; no other findings
Respiratory: Bilateral basal crepitations (neutropenic infection)
CNS: Alert, oriented; no focal deficits; fundus: retinal hemorrhages noted
INVESTIGATIONS
Hemogram (Pancytopenia):
| Value | Normal | |
|---|---|---|
| Hb | 5.8 g/dL | Low |
| TLC | 1,200/µL | Low |
| Neutrophils | 280/µL | Severely low (<500) |
| Platelets | 8,000/µL | Severely low |
| MCV | 92 fL | Normal |
| Reticulocytes | 0.05% | Severely reduced |
| Absolute reticulocyte count | 1,200/µL | Severely low |
Peripheral Blood Smear:
- Pancytopenia
- Red cells: Normochromic, normocytic
- No blast cells (rules out leukemia)
- No abnormal lymphocytes
- No dysplastic changes
Bone Marrow - DIAGNOSTIC:
- Biopsy: Hypocellular marrow with >90% fat cells
- Almost complete absence of hematopoietic elements
- No blasts, no fibrosis, no granulomas
- Confirms aplastic anemia
Other Investigations:
| Test | Result |
|---|---|
| LFT, RFT | Normal |
| HIV, Hepatitis B, C serology | Negative |
| ANA, dsDNA | Negative |
| Vitamin B12, Folate | Normal |
| Flow cytometry (PNH screen) | Negative for CD55/CD59 deficiency |
| HRCT Chest | Bilateral lower zone consolidation (fungal/bacterial) |
| Blood Culture | Staphylococcus epidermidis (neutropenic sepsis) |
| HLA typing | Pending (for transplant matching) |
| Cytogenetics (marrow) | 46 XY, normal karyotype |
| Telomerase gene mutations | Pending |
SEVERITY CLASSIFICATION (Camitta Criteria)
| Criterion | Finding | Threshold |
|---|---|---|
| Bone marrow cellularity | <10% | <25% |
| Neutrophils | 280/µL | <500/µL ✓ |
| Platelets | 8,000/µL | <20,000/µL ✓ |
| Reticulocytes | 1,200/µL | <20,000/µL ✓ |
Grade: VERY SEVERE APLASTIC ANEMIA (neutrophils <200/µL, all 3 criteria met)
DIAGNOSIS
Provisional: Pancytopenia secondary to aplastic anemia - drug-induced (carbamazepine)
Differential Diagnoses:
- Acute leukemia (pancytopenia + blasts - ruled out: no blasts, hypocellular marrow)
- Myelodysplastic syndrome (dysplasia on smear - ruled out: no dysplasia, normal karyotype)
- Hypersplenism (no splenomegaly here)
- Megaloblastic anemia with pancytopenia (MCV normal, B12/folate normal)
- PNH (flow cytometry negative)
Final Diagnosis: Very severe aplastic anemia, drug-induced (carbamazepine), complicated by neutropenic sepsis
TREATMENT
Immediate (Emergency):
| Action | Details |
|---|---|
| Stop carbamazepine | Immediately; switch seizure medication |
| Broad-spectrum IV antibiotics | Piperacillin-tazobactam + antifungal (fluconazole/voriconazole) |
| Packed RBC transfusion | 2 units irradiated, leukodepleted (Hb <7) |
| Platelet transfusion | 1 random donor pooled (plt <10,000 + bleeding) |
| Isolation | Reverse barrier nursing; neutropenic precautions |
| G-CSF | 5 µg/kg/day SC (to stimulate neutrophil recovery) |
| Cyclosporine | Started pending BMT decision |
Definitive Treatment (Decision Tree):
Very Severe Aplastic Anemia
|
Age 22 years
|
HLA typing
(sibling first)
|
----------------
| |
Matched sibling No matched sibling
present? available?
| |
Allogeneic BMT ATG + Cyclosporin
(curative, 70-80% + Eltrombopag
overall survival) (immunosuppression)
Definitive: Patient has a sibling - HLA matching in progress. Plan: Allogeneic hematopoietic stem cell transplantation (HSCT)
Pre-transplant:
- Minimize transfusions (allosensitization risk)
- Use irradiated, leukodepleted blood products only
- Myeloablative conditioning: Cyclophosphamide + ATG
PROGNOSIS
| Factor | Prognosis |
|---|---|
| Age < 40 + matched sibling + HSCT | 70-80% cure |
| Immunosuppression (no transplant) | 60-70% respond; relapse possible |
| Untreated severe aplastic anemia | >70% mortality at 1 year |
| Our patient | Favorable (young, matched sibling likely) |
FOLLOW-UP PLAN
- Daily CBC till stabilization
- Repeat bone marrow biopsy at 3 months (post-treatment)
- Monitor for PNH clone development (10% of aplastic anemia evolve to PNH)
- Long-term watch for MDS/AML transformation (especially post-immunosuppression)
COMPARISON SUMMARY (All 4 Cases)
| Feature | IDA | Megaloblastic | Hemolytic (G6PD) | Aplastic |
|---|---|---|---|---|
| Key Symptom | Pica, koilonychia | Neurological signs | Dark urine | Pancytopenia triad |
| MCV | Low | High | Normal | Normal |
| Reticulocytes | Low | Low | High | Very low |
| Spleen | Absent | Absent | Absent | Absent |
| Jaundice | No | Lemon-yellow | Yes | No |
| Smear | Hypochromic, pencil cells | Macro-ovalocytes, hyperseg. PMN | Bite cells, Heinz bodies | Pancytopenia, normal morphology |
| Bone Marrow | Erythroid hyperplasia | Megaloblasts | Erythroid hyperplasia | Hypocellular (fat cells) |
| Key Test | Serum Ferritin | Serum B12 + anti-IF Ab | G6PD assay | Bone marrow biopsy |
| Treatment | Oral iron + treat cause | IM B12 lifelong | Stop drug + supportive | HSCT or ATG+CSA |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine
detail presenting illness formale i
You want a detailed History of Present Illness (HPI) for Case 1 - Iron Deficiency Anemia (female patient - Mrs. Sunita Devi). Here it is, written in the full narrative format used in bedside case presentations and ward write-ups.
HISTORY OF PRESENT ILLNESS
Case 1 - Iron Deficiency Anemia | Mrs. Sunita Devi, 26F
Mrs. Sunita Devi, a 26-year-old homemaker from rural Uttar Pradesh, presented to the Medicine OPD on __________ with complaints of progressive fatigue, exertional breathlessness, pica, and heavy menstrual bleeding.
ONSET AND PROGRESSION OF MAIN COMPLAINTS
1. Fatigue and Weakness (3 months)
The patient was apparently well until 3 months ago, when she first noticed a gradual onset of fatigue and generalized weakness. Initially mild, she attributed it to her household workload and did not seek medical attention. Over the subsequent weeks, the fatigue progressively worsened, to the point where she is now unable to complete routine household tasks such as cooking and sweeping without needing to rest. She reports feeling exhausted even after a full night's sleep. There is no associated fever, weight loss, or night sweats.
2. Breathlessness on Exertion (2 months)
Approximately 2 months ago, she began noticing breathlessness while climbing stairs. At onset, it occurred only after climbing 2 flights of stairs; over the past 3-4 weeks it has progressed to occur on climbing even 1 flight of stairs or walking briskly for more than 100 meters. She denies breathlessness at rest, orthopnoea, paroxysmal nocturnal dyspnoea, or ankle swelling (minimal bilateral pedal edema present on examination). She has no cough, wheezing, hemoptysis, or chest pain. There is no history of prior cardiac or respiratory illness.
The breathlessness is gradual in onset, progressive, exertional, non-positional, and partially relieved by rest.
3. Pica - Craving for Ice and Chalk (1 month)
For the past 1 month, the patient has developed an unusual craving and compulsive urge to eat ice (pagophagia) and chalk. She consumes 8-10 ice cubes daily and has chewed chalk pieces on multiple occasions. She finds the texture and taste satisfying. She denies eating soil (geophagia), raw rice, or other non-food items. She acknowledges this as abnormal behavior but feels unable to control the craving. This symptom has been associated with embarrassment and she disclosed it only on direct questioning.
4. Heavy Menstrual Bleeding - Menorrhagia (6 months)
The patient gives a clear history of heavy menstrual bleeding for the past 6 months. Prior to this, her menstrual cycles were regular, with a cycle length of 28-30 days and a duration of 4-5 days, soaking 2-3 pads per day.
Over the past 6 months:
- Duration of bleeding has increased to 8-10 days per cycle
- She soaks more than 5 fully saturated pads per day during peak flow (days 2-4)
- She has passed clots on multiple occasions (clots larger than a 10-rupee coin)
- She experiences dysmenorrhoea (cramping lower abdominal pain during periods), which is new for her
- She has had inter-menstrual spotting on 2-3 occasions
- She has not consulted a gynecologist despite the severity
She denies post-coital bleeding, vaginal discharge, or pelvic pain outside of menses. She has had 2 prior normal vaginal deliveries (last delivery 18 months ago), with no excessive bleeding at delivery.
The menorrhagia is the identified cause of iron depletion in this patient.
5. Associated Symptoms (1-2 months)
The following additional symptoms developed gradually over the past 1-2 months, consistent with tissue iron depletion:
- Hairfall: Excessive hair loss on combing and washing, forming clumps. Not patchy. Present for 6 weeks.
- Soreness and burning of tongue (glossitis): Present for 4 weeks. The tongue feels raw and burning, especially while eating spicy food. She avoids spicy foods due to this.
- Cracks at corners of mouth (angular cheilitis): Painful fissures at both corners of the mouth for 3 weeks. Worsen during cold weather.
- Brittle, spoon-shaped nails (koilonychia): Noticed for 2 months. Her nails break easily and she noticed they appear "hollowed out."
- Palpitations: Intermittent awareness of heartbeats, especially at rest and at night, for 3 weeks. No associated chest pain, syncope, or dizziness.
- Dizziness and mild headache: Intermittent frontal headache and lightheadedness on standing up quickly (postural dizziness). Present for 2 months.
RELEVANT NEGATIVE HISTORY (Pertinent Negatives)
The following symptoms were specifically asked about and are absent, which helps in narrowing the differential diagnosis:
| System | Symptom Asked | Response |
|---|---|---|
| GIT | Hematemesis, melena, hematochezia | Absent |
| GIT | Dysphagia (to rule out Plummer-Vinson) | Absent (no difficulty swallowing) |
| GIT | Diarrhea, steatorrhea (malabsorption) | Absent |
| Urinary | Hematuria, hemoglobinuria | Absent |
| Constitutional | Fever, night sweats, significant weight loss | Absent |
| Neurological | Tingling, numbness, unsteadiness | Absent (rules against B12 deficiency) |
| Hematological | Jaundice, dark urine | Absent (rules against hemolysis) |
| Hematological | Easy bruising, petechiae, prolonged bleeding | Absent (rules against thrombocytopenia) |
| Respiratory | Orthopnoea, PND, cough | Absent |
| Infection | Prior TB, recurrent infections | Absent |
TREATMENT HISTORY
The patient took "iron tonic" from a local pharmacy approximately 2 months ago (unspecified syrup, taken irregularly for 3 weeks) with no perceived improvement. She stopped taking it due to constipation and dark stools (a normal side effect, but she was not counselled). She has taken no other medications for the current illness. She has not received any blood transfusions.
DIETARY HISTORY (Integrated in HPI)
On detailed dietary inquiry:
- Strict vegetarian (no meat, fish, or eggs)
- Predominantly wheat/rice-based diet with lentils (dal) and leafy vegetables 2-3 times per week
- Drinks 4-5 cups of tea per day, including with meals (tea contains tannins that inhibit iron absorption by up to 60%)
- Rarely consumes citrus fruits or Vitamin C-rich foods (which would enhance iron absorption)
- This dietary pattern means she consumes predominantly non-heme iron (1-2% absorption) with dietary inhibitors, providing far less than the 7-20 mg/day required for a premenopausal woman
COURSE OF ILLNESS
The illness has been gradual in onset and steadily progressive over the past 6 months. There has been no acute exacerbation, no spontaneous improvement, and no prior hospitalization. The patient's functional capacity has steadily declined - she is now only able to perform light household activity and requires rest periods throughout the day.
SUMMARY OF HPI
Mrs. Sunita Devi, 26F, vegetarian homemaker, presents with a 6-month history of progressive iron depletion due to menorrhagia (likely secondary to uterine fibroid on USG), superimposed on an inadequate dietary iron intake. This has resulted in a 3-month history of symptomatic moderate anemia (fatigue, exertional dyspnoea, palpitations, dizziness), progressive tissue iron depletion (koilonychia, angular cheilitis, glossitis, alopecia), and pica (pagophagia - craving for ice). There are no features of hemolysis, bleeding diathesis, malabsorption, neurological involvement, or alternate cause of anemia.
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E
for m ale
Here is the detailed History of Present Illness for a male patient with Iron Deficiency Anemia - the cause here is gastrointestinal blood loss (the most important cause in adult males), which is a clinically critical and exam-relevant scenario.
HISTORY OF PRESENT ILLNESS
Iron Deficiency Anemia | Male Patient
Mr. Rajesh Verma, 52 years / Male | Farmer | Rural Madhya Pradesh
Mrs. Rajesh Verma, a 52-year-old male farmer from rural Madhya Pradesh, presented to the Medicine OPD on __________ with complaints of progressive fatigue, exertional breathlessness, and black tarry stools.
CHIEF COMPLAINTS (Recap)
- Progressive fatigue and weakness - 5 months
- Breathlessness on exertion - 3 months
- Black, tarry stools (melena) - intermittent, 5 months
- Loss of appetite and 4 kg weight loss - 3 months
- Burning epigastric pain - 6 months
ONSET AND PROGRESSION
1. Epigastric Pain (6 months) - The Underlying Cause
The patient was apparently well until 6 months ago, when he first noticed a burning, gnawing pain in the epigastric region. The pain is:
- Onset: Gradual, insidious
- Character: Burning, gnawing
- Location: Epigastrium, occasionally radiating to the back
- Timing: Occurs 1-2 hours after meals and also wakes him from sleep at night (early morning hours)
- Relieving factors: Partially relieved by eating food and by antacids (which he has been self-medicating with for 4 months)
- Aggravating factors: Worsened by spicy food, alcohol (he consumes alcohol approximately 4-5 days per week, local liquor)
- Severity: Moderate; does not prevent him from working
He did not consult a doctor and managed with over-the-counter antacids (Tab ranitidine, self-purchased). He has not undergone any endoscopy or imaging.
2. Melena - Black Tarry Stools (5 months)
Approximately 5 months ago, the patient noticed that his stools had become black, tarry, foul-smelling, and sticky in consistency. He initially attributed this to the antacids he was taking. The melena has been intermittent - present for 4-5 consecutive days, then absent for 2-3 weeks, then recurring.
On direct questioning:
- The stool is jet black, tarry, and has a distinctly foul odor (consistent with altered blood - rules out simple dark stool from iron/bismuth)
- He has passed no fresh red blood per rectum (no hematochezia)
- No hematemesis (vomiting of blood)
- No history of frank rectal bleeding, mucus, or altered bowel habit (no alternating constipation-diarrhea)
- He estimates passing tarry stools approximately 8-10 times over the past 5 months
Clinical significance: In an adult male, GI blood loss causing iron deficiency must be evaluated for a structural lesion (peptic ulcer, gastric carcinoma, colorectal cancer) until proven otherwise. This is a red flag requiring urgent endoscopy.
3. Fatigue and Weakness (5 months)
Around the same time as the onset of melena, the patient began noticing progressive fatigue and generalized weakness. Initially mild, he could continue his farm work with moderate effort. Over the past 2 months, the fatigue has become severe and limiting - he is unable to work in the field for more than 1-2 hours and requires frequent rest. He reports feeling exhausted after minimal effort. He has no fever, chills, or night sweats.
4. Breathlessness on Exertion (3 months)
3 months ago, he developed breathlessness on walking on level ground for more than 200 meters or climbing a flight of stairs. The breathlessness is:
- Gradual in onset, progressive
- Exertional only - no breathlessness at rest
- No orthopnoea, no paroxysmal nocturnal dyspnoea
- No ankle swelling (no cardiac failure)
- No prior history of cardiac or pulmonary disease
- No smoking history
The exertional dyspnoea in this context is consistent with the reduced oxygen-carrying capacity of the blood due to progressive anemia from chronic GI blood loss.
5. Loss of Appetite and Weight Loss (3 months)
Over the past 3 months, the patient reports a significant decrease in appetite - he is eating approximately half his normal quantity. He has had an unintentional weight loss of approximately 4 kg over 3 months (confirmed on records from a prior visit to a primary health centre). He attributes it to poor appetite.
Clinical significance: Significant weight loss (>5% body weight in 3 months) combined with epigastric pain, melena, and iron deficiency anemia in a middle-aged male raises the concern for gastric malignancy until proven otherwise. This is a mandatory red flag.
6. Additional Symptoms of Iron Deficiency (Tissue Depletion)
The following symptoms developed over the past 2-3 months, reflecting progressive iron depletion beyond just the hemoglobin compartment:
- Pica: The patient admits to craving and chewing raw rice and mud (geophagia) for the past 2 months. He discloses this reluctantly on direct questioning.
- Hairfall: Increased hair loss on combing, noted for 6 weeks
- Brittle nails: Nails break easily; wife noticed they appear concave (koilonychia) for 4-6 weeks
- Soreness of tongue: Tongue feels raw and smooth; mild burning with spicy foods for 4 weeks (atrophic glossitis)
- Angular cheilitis: Painful cracks at corners of mouth for 3 weeks
- Dizziness on standing: Postural dizziness (lightheadedness) when rising from squatting or lying position, for 4-6 weeks
- Palpitations: Intermittent awareness of fast heartbeat, particularly at rest at night, for 3 weeks. No syncope, no chest pain.
ALCOHOL HISTORY (Relevant to Cause)
The patient consumes local alcohol (desi sharab) approximately 4-5 days per week, approximately 4-6 standard drinks per session, for the past 15 years. This is relevant for the following reasons:
- Chronic alcohol use causes gastric mucosal erosions and peptic ulceration, contributing to GI blood loss
- Alcohol interferes with folate absorption (may contribute to combined deficiency)
- Alcohol can cause round macrocytosis independent of anemia, potentially masking the microcytosis of IDA on MCV
RELEVANT NEGATIVE HISTORY (Pertinent Negatives)
| System | Symptom Asked | Response |
|---|---|---|
| GIT | Hematemesis | Absent (no vomiting of blood) |
| GIT | Fresh rectal bleeding (hematochezia) | Absent |
| GIT | Dysphagia (difficulty swallowing) | Absent (rules against esophageal carcinoma) |
| GIT | Jaundice, pale stools, dark urine | Absent (rules against hepatic cause) |
| GIT | Altered bowel habit, mucus in stools | Absent (lowers suspicion for colorectal CA - but must still exclude) |
| Urinary | Hematuria, hemoglobinuria | Absent |
| Constitutional | Fever, drenching night sweats | Absent (rules against lymphoma/TB) |
| Neurological | Tingling, numbness, unsteadiness | Absent (rules against B12 deficiency) |
| Hematological | Jaundice, dark urine | Absent (rules against hemolysis) |
| Hematological | Easy bruising, petechiae | Absent (rules against thrombocytopenia) |
| Occupational | Exposure to chemicals, heavy metals, benzene | Absent (rules against aplastic/toxic) |
| Parasites | Prior hookworm treatment, walking barefoot | Yes - walks barefoot on farm soil (hookworm possible contributor) |
Note on hookworm: This patient works barefoot on farm soil. Hookworm (Ancylostoma duodenale) infestation causes chronic intestinal blood loss and is an important cause of iron deficiency anemia in rural agricultural laborers in India. Stool examination for ova and parasites is essential.
TREATMENT HISTORY
- Self-medicating with antacids (Tab ranitidine, OTC) for 4 months - no prescription
- No prior iron supplementation
- No prior endoscopy or investigation for GI symptoms
- No prior blood transfusions
- No herbal/traditional medicines
DIETARY HISTORY (Integrated)
- Non-vegetarian but meat consumed only 1-2 times per week (limited income)
- Main diet: wheat rotis, dal, seasonal vegetables
- Eats very few fruits; no citrus
- Drinks 4-5 cups of tea daily including with meals (tannins inhibit non-heme iron absorption)
- Chronic alcohol use as above
- Despite being non-vegetarian, his dietary iron intake is insufficient to compensate for ongoing GI blood loss
OCCUPATIONAL HISTORY
Works as a farmer; barefoot contact with soil daily for 30+ years (hookworm risk). No known exposure to industrial chemicals, pesticides beyond routine agricultural use, or radiation.
COURSE OF ILLNESS
The illness has been insidious and progressive over 5-6 months, with no acute episodes and no spontaneous improvement. The patient delayed seeking medical attention, attributing symptoms to "weakness from hard work" and "stomach acidity." The progressive weight loss and worsening anemia over the past 3 months prompted the family to bring him to the hospital.
SUMMARY OF HPI
Mr. Rajesh Verma, 52M, a farmer with chronic alcoholism, presents with a 5-month history of iron deficiency anemia secondary to chronic gastrointestinal blood loss, manifesting as progressive fatigue, exertional dyspnoea, and features of tissue iron depletion (koilonychia, angular cheilitis, atrophic glossitis, pica). The likely source of blood loss is a peptic ulcer/gastric lesion given the 6-month history of burning epigastric pain relieved by food and antacids, intermittent melena, significant weight loss (4 kg/3 months), and risk factors of chronic alcohol use. Gastric malignancy must be actively excluded by urgent upper GI endoscopy. Hookworm infestation as an additional contributing cause requires exclusion by stool examination. There are no features of hemolysis, neurological involvement, or alternate hematological diagnosis.
KEY CLINICAL TEACHING POINTS FOR THIS CASE
| Point | Teaching |
|---|---|
| IDA in adult males | Always assume GI blood loss until proven otherwise - never dismiss it as dietary |
| Melena vs. dark stool | Melena = jet black, tarry, foul-smelling (altered blood from upper GI); dark stool = iron/bismuth (no smell) |
| Weight loss + IDA + epigastric pain | Red flag triad - urgent endoscopy mandatory to exclude gastric malignancy |
| Hookworm | Important cause of IDA in rural, agricultural populations; stool exam essential |
| Alcohol + IDA | Alcohol causes gastric erosions + impairs folate - may present with mixed picture |
| TIBC in IDA | Elevated (liver makes more transferrin when iron is low) - opposite of anemia of chronic disease |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goldman-Cecil Medicine
General questions askedin presenting illness with out above case
Here is a complete set of general questions asked during History of Present Illness (HPI) for any Anemia case - independent of the specific type. These are the standard questions every MBBS student must ask systematically at the bedside.
GENERAL QUESTIONS ASKED IN HISTORY OF PRESENT ILLNESS
Anemia - Any Case | MBBS Bedside Clerking Guide
WHY WE ASK A STRUCTURED HPI IN ANEMIA
Anemia is a symptom, not a diagnosis. The HPI helps you answer three questions:
- How severe is the anemia? (symptoms of oxygen deprivation)
- What type is it? (clues from associated symptoms)
- What is the cause? (bleeding, destruction, decreased production)
SECTION 1 - QUESTIONS ABOUT THE ANEMIA SYMPTOMS THEMSELVES
These questions establish the severity and duration of the anemia.
A. Fatigue / Weakness
| Question | Why It Is Asked |
|---|---|
| When did the weakness start? | Establishes duration - acute vs chronic onset |
| Did it come suddenly or gradually? | Sudden = acute blood loss or acute hemolysis; gradual = chronic anemia |
| Is it getting worse, better, or the same? | Progressive worsening suggests ongoing cause |
| Does it affect your daily work/activities? | Functional grading of severity |
| Do you feel tired even after a full night's sleep? | Characteristic of anemia - rest does not relieve it |
B. Breathlessness
| Question | Why It Is Asked |
|---|---|
| Do you get breathless on walking or climbing stairs? | Exertional dyspnoea - graded by distance/flights |
| How much activity causes breathlessness? | Grades severity (can walk 500m? 100m? On flat ground?) |
| Do you get breathless at rest? | Rest dyspnoea = severe anemia or cardiac failure |
| Do you wake up at night breathless? (PND) | Suggests cardiac failure - not pure anemia |
| Do you need extra pillows to sleep? (Orthopnoea) | Suggests cardiac failure |
| Is the breathlessness getting worse over time? | Progressive = ongoing blood loss or worsening production failure |
C. Palpitations
| Question | Why It Is Asked |
|---|---|
| Do you feel your heart beating fast or pounding? | Tachycardia is compensatory in anemia |
| Does it occur at rest or only on activity? | At rest = more severe anemia |
| Is it associated with chest pain or dizziness? | Rules out arrhythmia or cardiac cause |
| Did you ever faint or feel you would faint? | Syncope = severe anemia or cardiac cause |
D. Dizziness / Headache
| Question | Why It Is Asked |
|---|---|
| Do you feel dizzy or lightheaded? | Cerebral hypoxia from anemia |
| Does it happen on standing up suddenly? (Postural dizziness) | Suggests postural hypotension from blood loss |
| Do you have frequent headaches? | Cerebral hypoxia symptom |
| Do you have difficulty concentrating or memory problems? | Iron deficiency affects CNS even before frank anemia |
| Do you feel cold all the time? | Reduced peripheral perfusion in anemia |
SECTION 2 - QUESTIONS TO FIND THE CAUSE OF ANEMIA
A. Questions for Blood Loss
| Question | Why It Is Asked |
|---|---|
| Have you noticed any blood in your stools? | Upper GI bleed (melena) or lower GI bleed (fresh blood) |
| Are your stools black and tarry? (Melena) | Upper GI source - peptic ulcer, gastric cancer |
| Have you vomited blood? (Hematemesis) | Upper GI bleed - urgent |
| Do you have burning or pain in the stomach/abdomen? | Peptic ulcer disease causing GI blood loss |
| Have you noticed blood in your urine? (Hematuria) | Renal/bladder source of blood loss |
| Do you cough up blood? (Hemoptysis) | Pulmonary source |
| (For females) Are your periods heavy? How many pads per day? | Menorrhagia - most common cause of IDA in women |
| (For females) Duration of each period? Any clots? | Quantifies menstrual blood loss |
| Do you have any known bleeding from anywhere? | Nose bleeds, gum bleeding, prolonged wound bleeding |
| Have you had any recent surgery or trauma? | Acute blood loss |
B. Questions for Hemolysis (Destruction)
| Question | Why It Is Asked |
|---|---|
| Have you noticed yellowing of eyes or skin? (Jaundice) | Bilirubin from RBC breakdown - hemolysis |
| Is your urine dark brown or red? (Hemoglobinuria) | Intravascular hemolysis - G6PD, PNH, mechanical |
| Did the urine turn dark after eating fava beans? | G6PD deficiency - favism |
| Did you take any new medication recently? | Drug-induced hemolysis (primaquine, dapsone, sulfa drugs) |
| Do you have a family history of jaundice or anemia? | Hereditary hemolytic anemias (spherocytosis, G6PD, sickle cell) |
| Do you have pain in your abdomen or back during these episodes? | Sickle cell crisis, severe hemolysis |
| Have you received a blood transfusion recently? | Transfusion reaction |
| Do you have frequent infections? | Immunodeficiency - may trigger hemolysis (e.g. in G6PD) |
| Any history of malaria? | Malaria destroys RBCs |
| Have you been told you have gallstones? (Young person) | Pigment stones from chronic hemolysis |
C. Questions for Decreased Production
| Question | Why It Is Asked |
|---|---|
| Do you eat meat, fish, eggs? | Dietary B12 source - absent in vegans |
| Are you a strict vegetarian or vegan? | B12/iron deficiency risk |
| Do you eat adequate fruits and vegetables? | Folate source |
| Have you had any stomach surgery? (Gastrectomy) | Removes parietal cells → no intrinsic factor → no B12 absorption |
| Do you have any bowel disease, diarrhea, or malabsorption? | Crohn's, celiac disease → B12/folate/iron malabsorption |
| Do you take any medications? (List all) | Methotrexate, phenytoin, OCP → folate deficiency; Chloramphenicol → aplastic anemia |
| Do you drink alcohol? How much, how often? | Alcohol → folate deficiency + macrocytosis + gastric erosions |
| Have you had any chronic illness? | CKD → low EPO; Hypothyroidism → macrocytosis; Cancer → anemia of chronic disease |
| Do you have any kidney disease? | Erythropoietin deficiency → normocytic anemia |
| Have you had frequent infections (TB, HIV)? | Anemia of chronic inflammation; marrow suppression |
| Any history of cancer or chemotherapy/radiation? | Marrow suppression → aplastic / decreased production |
| Any exposure to chemicals? (Benzene, pesticides) | Aplastic anemia risk |
| Do you have bone pain? | Marrow infiltration, multiple myeloma |
SECTION 3 - SPECIFIC SYMPTOM QUESTIONS BY ANEMIA TYPE
For Iron Deficiency - Ask These Specifically
| Question | Why |
|---|---|
| Do you crave unusual non-food items? (Pica) | Pagophagia (ice), geophagia (mud/clay), amylophagia (starch) |
| Have you noticed spoon-shaped nails? (Koilonychia) | Tissue iron depletion |
| Do you have cracks at corners of mouth? (Angular cheilitis) | Iron deficiency |
| Is your tongue smooth and sore? (Glossitis) | Atrophic glossitis - iron/B12 deficiency |
| Do you have excessive hairfall? | Tissue iron depletion |
| Do you drink a lot of tea? | Tannins inhibit iron absorption |
| Do you walk barefoot on soil? (Rural) | Hookworm risk |
For Megaloblastic Anemia (B12/Folate) - Ask These Specifically
| Question | Why |
|---|---|
| Do you have tingling or numbness in hands/feet? | Subacute combined degeneration - B12 only |
| Do you have difficulty walking, especially in dark? | Posterior column loss (proprioception) - B12 |
| Have you fallen recently? | Ataxia from posterior column disease |
| Do you feel unsteady? | Romberg positive - posterior column |
| Any memory problems or confusion? | B12 deficiency can cause dementia |
| Any psychiatric symptoms? (Depression, irritability) | "Megaloblastic madness" - B12 |
| Do you eat meat/dairy? Are you vegan? | B12 dietary source |
| Did you have stomach surgery? | Loss of parietal cells → no intrinsic factor |
| Do you drink alcohol? | Folate deficiency + macrocytosis |
| Are you pregnant? | Increased folate requirement |
| Do you take antiepileptics? (Phenytoin, carbamazepine) | Folate antagonism |
| Do you take methotrexate or any chemotherapy? | Folate antagonism |
For Hemolytic Anemia - Ask These Specifically
| Question | Why |
|---|---|
| Is there a family history of jaundice/anemia/splenomegaly? | Hereditary hemolytic anemia |
| Did you ever need a splenectomy? | Previous hemolytic disorder |
| Did you receive any new drug recently? | Drug-induced hemolysis |
| Do episodes occur with illness/infection? | G6PD trigger, sickle crisis |
| Do you have bone/joint pain during episodes? | Sickle cell crisis |
| Do you have pain in the chest during episodes? | Acute chest syndrome - sickle cell |
| Do you have recurrent abdominal pain with dark urine? | PNH |
| Any morning dark urine (first urine of the day)? | PNH (complement activation overnight) |
For Aplastic Anemia - Ask These Specifically
| Question | Why |
|---|---|
| Do you bruise easily without injury? | Thrombocytopenia - aplastic anemia |
| Do you have petechiae (pinpoint red spots)? | Thrombocytopenia |
| Do you bleed from gums or nose easily? | Thrombocytopenia |
| Do you have recurrent or prolonged infections? | Neutropenia - marrow failure |
| Have you had any recent viral illness? (Hepatitis, EBV) | Viral-triggered aplastic anemia |
| Any exposure to chemicals, solvents, benzene? | Aplastic anemia cause |
| Any drug intake? (Carbamazepine, chloramphenicol, gold) | Drug-induced aplastic anemia |
| Any radiation exposure? | Aplastic anemia cause |
| Any family members with blood disorders? | Fanconi anemia (inherited) |
SECTION 4 - GENERAL QUESTIONS ASKED IN EVERY ANEMIA HPI
These are asked in every case regardless of suspected type:
| Category | Questions |
|---|---|
| Onset | When exactly did symptoms start? Was there a triggering event? |
| Progression | Are symptoms getting better, worse, or the same? |
| Severity | How much does it affect daily life and work? |
| Prior episodes | Have you had anemia before? Any blood transfusions? |
| Treatment taken | Any iron tablets, B12 injections, or tonic taken? Did it help? |
| Dietary history | Vegetarian/vegan? Tea/coffee intake? Alcohol? |
| Drug history | Complete drug list - many drugs cause all types of anemia |
| Surgical history | Gastrectomy, bowel resection, splenectomy |
| Chronic illness | CKD, hypothyroidism, liver disease, rheumatoid arthritis, TB, HIV, malignancy |
| Family history | Any family members with anemia, jaundice, splenomegaly, blood disorder |
| Occupational | Exposure to chemicals, radiation, heavy metals; barefoot soil contact |
| Pregnancy (females) | Current pregnancy, number of pregnancies, recent delivery |
| Menstrual (females) | Cycle regularity, duration, pad count, clots, intermenstrual bleeding |
SECTION 5 - PERTINENT NEGATIVES TO ALWAYS ASK AND DOCUMENT
These must be specifically asked AND their absence documented in the write-up:
| Symptom | Significance of Its Absence |
|---|---|
| No jaundice / dark urine | Against hemolysis |
| No tingling / numbness | Against B12 deficiency |
| No melena / hematemesis | Against upper GI blood loss |
| No petechiae / bruising | Against aplastic / thrombocytopenia |
| No fever / night sweats / weight loss | Against malignancy / infection / lymphoma |
| No bone pain | Against multiple myeloma / marrow infiltration |
| No dysphagia | Against Plummer-Vinson / esophageal carcinoma |
| No change in bowel habit | Against colorectal carcinoma |
| No frothy / bulky stools | Against malabsorption / celiac disease |
QUICK SUMMARY TABLE
| Goal | Key Questions |
|---|---|
| Severity of anemia | Fatigue grade, breathlessness (rest vs exertion), palpitations, syncope |
| Duration and onset | Sudden vs gradual, triggering event |
| Blood loss? | Melena, hematemesis, hematuria, menorrhagia, trauma |
| Hemolysis? | Jaundice, dark urine, family history, drug intake, malaria |
| Production failure? | Diet (vegan), surgery (gastrectomy), drugs, chronic illness, CKD, radiation |
| IDA clues | Pica, koilonychia, glossitis, tea intake, hookworm exposure |
| B12/folate clues | Neurology (tingling, unsteady), vegan diet, gastric surgery, alcohol |
| Aplastic clues | Bruising, petechiae, infections, drugs, chemicals |
| Treatment tried | Iron/B12 tablets, transfusions, response |
These questions form the framework for history-taking in any anemia case at the bedside, OPD, or examination.
causes - acute I chro
You want causes of anemia divided into Acute and Chronic. Here is the complete, exam-ready breakdown:
CAUSES OF ANEMIA
Acute vs Chronic Classification
MBBS Medicine | Complete Reference
PART 1 - ACUTE CAUSES OF ANEMIA
(Anemia that develops over hours to days)
A. ACUTE BLOOD LOSS (Hemorrhagic Anemia)
| Source | Specific Causes |
|---|---|
| Gastrointestinal | Bleeding peptic ulcer, esophageal varices (rupture), Mallory-Weiss tear, acute gastritis/erosions, Dieulafoy lesion, angiodysplasia |
| Trauma | Road traffic accident, penetrating injury, fracture (femur fracture = 1-2L loss; pelvic fracture = 2-4L loss) |
| Surgical | Post-operative hemorrhage, intraoperative blood loss |
| Obstetric | Postpartum hemorrhage, placenta praevia, abruptio placentae, ruptured ectopic pregnancy |
| Respiratory | Massive hemoptysis (TB, bronchiectasis, lung carcinoma) |
| Urological | Gross hematuria (renal carcinoma, bladder carcinoma, trauma) |
| Vascular | Ruptured aortic aneurysm, arterial injury |
| Iatrogenic | Excessive phlebotomy (ICU patients), surgical drainage |
| Internal | Hemothorax, hemoperitoneum, retroperitoneal hematoma |
Key Features of Acute Blood Loss Anemia:
- Normocytic, normochromic initially
- Reticulocytosis appears after 5-7 days
- Hb may be normal in first few hours (hemodilution not yet complete)
- Tachycardia, hypotension, cold peripheries (shock features)
B. ACUTE HEMOLYSIS
| Category | Causes |
|---|---|
| Drug-induced (oxidant) | Primaquine, dapsone, nitrofurantoin, rasburicase, high-dose Vit C, sulfonamides |
| Infections | Malaria (Plasmodium falciparum - most severe), Clostridium perfringens septicemia, Bartonella, babesiosis |
| Transfusion reaction | ABO incompatibility (most dangerous - intravascular hemolysis within minutes) |
| Microangiopathic | TTP (Thrombotic Thrombocytopenic Purpura), HUS (Hemolytic Uremic Syndrome), DIC (Disseminated Intravascular Coagulation) |
| Mechanical | Defective prosthetic heart valves, cardiopulmonary bypass, IABP |
| Snake venom | Viper bite → phospholipases destroy RBC membrane |
| Burns | Severe thermal injury → direct RBC membrane destruction |
| G6PD deficiency (acute trigger) | Fava beans, oxidant drugs, infection → acute hemolytic episode |
| Autoimmune (acute) | Cold agglutinin disease (Mycoplasma, EBV), paroxysmal cold hemoglobinuria |
| PNH (crisis) | Paroxysmal Nocturnal Hemoglobinuria - complement-mediated, often overnight |
| Hypersplenism (acute) | Splenic sequestration crisis (sickle cell in children) |
Key Features of Acute Hemolysis:
- Sudden pallor + jaundice + dark urine (hemoglobinuria)
- Normocytic (or slightly macrocytic due to reticulocytosis)
- Reticulocytes elevated within 24-48 hours
- LDH very high, haptoglobin absent, indirect bilirubin elevated
- May cause acute kidney injury (hemoglobin precipitates in tubules)
C. ACUTE BONE MARROW SUPPRESSION
| Cause | Examples |
|---|---|
| Parvovirus B19 | Aplastic crisis in patients with pre-existing hemolytic anemia (sickle cell, hereditary spherocytosis) - reticulocytes drop to zero |
| Chemotherapy | Cytotoxic drugs (cyclophosphamide, methotrexate) → acute marrow suppression |
| Radiation | Total body irradiation → marrow failure |
| Sepsis | Severe infections suppress erythropoiesis acutely |
PART 2 - CHRONIC CAUSES OF ANEMIA
(Anemia that develops over weeks to months)
A. CHRONIC BLOOD LOSS → IRON DEFICIENCY
| Source | Specific Causes |
|---|---|
| Gastrointestinal (MOST COMMON in males and postmenopausal females) | Peptic ulcer disease (chronic), colorectal carcinoma, gastric carcinoma, angiodysplasia, inflammatory bowel disease (Crohn's, UC), hookworm infestation, hemorrhoids, esophageal varices (slow bleed), hiatus hernia (Cameron lesions) |
| Gynecological (MOST COMMON in premenopausal females) | Menorrhagia (uterine fibroids, endometriosis, PCOS, hormonal causes, IUD), multiple/frequent pregnancies |
| Urological | Chronic microscopic hematuria (IgA nephropathy, renal carcinoma, bladder carcinoma) |
| Pulmonary | Idiopathic pulmonary hemosiderosis, Goodpasture syndrome (iron trapped in lung macrophages) |
| Iatrogenic | Frequent blood donations, repeated phlebotomy in ICU patients, hemodialysis (blood loss in circuit) |
Result: Microcytic, hypochromic anemia. Serum ferritin low, TIBC high, transferrin saturation <15%.
B. NUTRITIONAL DEFICIENCY ANEMIAS (Chronic)
| Deficiency | Causes | Type of Anemia |
|---|---|---|
| Iron deficiency | Inadequate diet (vegans, infants, poverty), malabsorption (celiac, Crohn's, post-gastrectomy), increased demand (pregnancy, growth) | Microcytic, hypochromic |
| Vitamin B12 deficiency | Pernicious anemia (anti-IF antibodies), veganism, gastrectomy, ileal resection/Crohn's, fish tapeworm, bacterial overgrowth | Macrocytic, megaloblastic |
| Folate deficiency | Alcoholism, poor diet, pregnancy (increased demand), malabsorption, drugs (methotrexate, phenytoin, trimethoprim, OCP) | Macrocytic, megaloblastic |
| Protein deficiency | Kwashiorkor, severe malnutrition | Normocytic |
| Copper deficiency | Rare; TPN without copper, excess zinc intake | Normocytic/microcytic |
| Vitamin C deficiency | Scurvy - bleeding + impaired iron absorption | Contributes to IDA |
C. CHRONIC HEMOLYTIC ANEMIAS
i. Intrinsic (Intracorpuscular) Defects
| Category | Diseases |
|---|---|
| RBC Membrane defects | Hereditary spherocytosis (AD, spectrin/ankyrin defect), Hereditary elliptocytosis, Hereditary stomatocytosis |
| RBC Enzyme defects | G6PD deficiency (X-linked; chronic hemolysis in severe variants), Pyruvate kinase deficiency (AR; chronic non-spherocytic hemolytic anemia) |
| Hemoglobin defects | Sickle cell disease (HbSS - chronic hemolysis + vaso-occlusive crises), HbC disease, HbE disease, Unstable hemoglobins |
| Globin synthesis defects | Beta-thalassemia major (severe chronic hemolysis + ineffective erythropoiesis), Alpha-thalassemia (HbH disease) |
| Acquired (intracorpuscular) | Paroxysmal Nocturnal Hemoglobinuria - PNH (chronic intravascular hemolysis) |
ii. Extrinsic (Extracorpuscular) Defects
| Category | Diseases |
|---|---|
| Autoimmune | Warm AIHA (IgG, DAT positive; SLE, CLL, drugs), Cold agglutinin disease (IgM, Mycoplasma, EBV, lymphoma), Drug-induced AIHA (methyldopa, penicillin) |
| Microangiopathic (chronic) | Chronic TTP, giant hemangioma (Kasabach-Merritt), malignant hypertension, chronic DIC |
| Mechanical (chronic) | Prosthetic heart valves (especially mechanical), march hemoglobinuria |
| Infections | Chronic malaria, bartonellosis |
| Hypersplenism | Portal hypertension, storage diseases (Gaucher's, Niemann-Pick), lymphoma |
| Liver disease | Acanthocytes (spur cells) in severe hepatocellular disease |
D. CHRONIC DECREASED PRODUCTION ANEMIAS
i. Anemia of Chronic Disease / Inflammation (ACD)
Most common anemia in hospitalized patients. Caused by:
| Disease Category | Examples |
|---|---|
| Chronic infections | Tuberculosis, HIV, chronic osteomyelitis, bacterial endocarditis, lung abscess |
| Chronic inflammatory diseases | Rheumatoid arthritis, SLE, IBD, vasculitis, sarcoidosis |
| Malignancies | Any solid tumor or hematological malignancy |
Mechanism: IL-6 → hepcidin ↑ → blocks iron release from macrophages → iron-restricted erythropoiesis
Lab pattern: Normocytic (or mildly microcytic), low serum iron, low TIBC, normal/high ferritin
ii. Renal Anemia (Anemia of CKD)
| Cause | Mechanism |
|---|---|
| Chronic Kidney Disease (any cause) | Reduced EPO production by peritubular cells |
| Additional factors in CKD | Uremic toxins shorten RBC life, blood loss from dialysis, poor nutrition |
Pattern: Normocytic, normochromic; EPO levels low for degree of anemia
Treatment: Erythropoiesis-stimulating agents (ESAs) - darbepoetin, epoetin alfa
iii. Endocrine Anemias
| Endocrine Cause | Mechanism | Type |
|---|---|---|
| Hypothyroidism | Reduced EPO production + reduced erythropoiesis | Normocytic (or macrocytic - round macrocytes) |
| Hypopituitarism | Reduced androgens + thyroid hormone | Normocytic |
| Addison's disease | Reduced androgens + cortisol | Normocytic |
| Hypogonadism (males) | Androgens stimulate EPO production; deficiency → mild anemia | Normocytic |
| Hyperparathyroidism | PTH toxic to erythroid progenitors | Normocytic |
| Diabetes mellitus | CKD + autonomic neuropathy affecting EPO production | Normocytic |
iv. Bone Marrow Failure / Aplastic Anemia
| Cause | Examples |
|---|---|
| Idiopathic (most common) | Immune-mediated T-cell suppression of stem cells |
| Drugs | Chloramphenicol (dose-independent, rare but fatal), carbamazepine, phenytoin, sulfonamides, gold salts, NSAIDs, benzene |
| Viral | Hepatitis (non-A, non-B, non-C seronegative hepatitis), EBV, CMV, HIV, parvovirus B19 |
| Radiation | Total body irradiation |
| Chemicals | Benzene, insecticides, solvents |
| Inherited | Fanconi anemia (AR; chromosomal fragility + congenital anomalies), Dyskeratosis congenita (telomerase mutation) |
| Autoimmune | SLE, thymoma-associated pure red cell aplasia |
v. Bone Marrow Infiltration (Myelophthisic Anemia)
| Infiltrating Process | Cause |
|---|---|
| Metastatic carcinoma | Breast, prostate, lung, thyroid, kidney (most common) |
| Hematological malignancy | Leukemia (CML, CLL, ALL, AML), lymphoma (NHL, Hodgkin's), multiple myeloma, myelofibrosis |
| Granulomatous disease | Tuberculosis, sarcoidosis |
| Storage diseases | Gaucher's disease, Niemann-Pick disease |
| Osteopetrosis | Marble bone disease - sclerotic bone leaves no room for marrow |
Smear: Leukoerythroblastic picture (immature WBCs + nucleated RBCs) + teardrop cells (dacrocytes)
vi. Pure Red Cell Aplasia (PRCA)
| Type | Causes |
|---|---|
| Congenital | Diamond-Blackfan anemia (ribosomal protein mutation) |
| Acquired - acute | Parvovirus B19 (aplastic crisis in hemolytic anemia) |
| Acquired - chronic | Thymoma (15-20% have PRCA), CLL, drugs (EPO antibodies), SLE |
vii. Dyserythropoietic / Ineffective Erythropoiesis
| Condition | Mechanism |
|---|---|
| Beta-thalassemia major | RBCs produced but destroyed in marrow before release |
| Myelodysplastic syndrome (MDS) | Clonal stem cell disorder; cells made but dysfunctional and destroyed in marrow |
| Megaloblastic anemia | Intramedullary destruction of megaloblasts |
| Sideroblastic anemia | Iron loaded but not used; ring sideroblasts on Prussian blue stain |
SUMMARY TABLE - ACUTE vs CHRONIC
| Feature | ACUTE Anemia | CHRONIC Anemia |
|---|---|---|
| Onset | Hours to days | Weeks to months |
| Main mechanisms | Acute blood loss, acute hemolysis | Nutritional deficiency, chronic blood loss, chronic hemolysis, decreased production |
| Hb drop | Sudden, severe | Gradual, compensated |
| Symptoms | Shock (hypotension, tachycardia, cold sweat) | Fatigue, dyspnoea on exertion, pallor |
| Reticulocytes | Rise after 5-7 days (blood loss) or 1-2 days (hemolysis) | Low (production failure) or high (chronic hemolysis) |
| MCV | Normocytic initially | Micro/macro/normo depending on cause |
| Compensation | Tachycardia, vasoconstriction, 2,3-DPG shift | Increased 2,3-DPG, increased cardiac output, increased EPO |
| Key examples | Ruptured ectopic, acute GI bleed, transfusion reaction, severe malaria | IDA (menorrhagia, peptic ulcer), megaloblastic, aplastic, CKD anemia |
| Emergency treatment | Blood transfusion, fluid resuscitation, stop bleeding | Treat underlying cause; iron/B12/EPO supplementation |
MNEMONIC - CAUSES OF CHRONIC ANEMIA
"BIND MARR"
- B - B12 / Folate deficiency (megaloblastic)
- I - Iron deficiency (chronic blood loss / dietary)
- N - Nutritional (protein, copper)
- D - Disease (anemia of chronic disease / inflammation)
- M - Marrow failure (aplastic anemia)
- A - Anemia of CKD (EPO deficiency)
- R - RBC destruction (chronic hemolysis - hereditary spherocytosis, sickle cell, thalassemia)
- R - Replacement of marrow (myelophthisic anemia - metastasis, leukemia)
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goldman-Cecil Medicine
Examination
Here is the complete, structured Physical Examination for Anemia - exactly as performed and written up at the bedside for MBBS students.
PHYSICAL EXAMINATION IN ANEMIA
Complete Bedside Guide | MBBS Medicine
APPROACH TO EXAMINATION
Examination in anemia has two goals:
- Confirm the presence and severity of anemia
- Find clues to the TYPE and CAUSE of anemia
Always follow the sequence:
General Physical Examination → Vital Signs → Systemic Examination
PART 1 - GENERAL PHYSICAL EXAMINATION
1. BUILT AND NOURISHMENT
| Observation | Significance |
|---|---|
| Thin, poorly nourished | Nutritional anemia (IDA, megaloblastic), malignancy |
| Normal built | Does not exclude anemia |
| Overweight/obese | Menorrhagia from PCOS → IDA in females |
| Stunted growth (child) | Chronic anemia from thalassemia, sickle cell |
2. PALLOR ← MOST IMPORTANT SIGN
Where to look (sites of pallor):
| Site | How to Examine | Significance |
|---|---|---|
| Conjunctivae | Pull down lower eyelid - look at palpebral conjunctiva | Most reliable site; pale/white = anemia |
| Palms | Compare patient's palm to your own | Creases lose pink color in moderate anemia |
| Nail beds | Press nail and release - look at nail bed color | Pale on release = anemia |
| Tongue | Ask patient to open mouth and lift tongue | Pallor of tongue mucosa |
| Buccal mucosa | Inner cheek lining | Pale mucosa |
Grading of Pallor:
| Grade | Appearance |
|---|---|
| + (Mild) | Slight pallor, only conjunctiva involved |
| ++ (Moderate) | Conjunctiva + palms + tongue |
| +++ (Severe) | All sites involved; very marked pallor |
| ++++ (Very severe) | Extreme pallor, patient may have high-output cardiac failure signs |
Exam Tip: Conjunctival pallor is the most reliable sign. Palmar pallor has poor sensitivity. Always grade and document.
3. ICTERUS (JAUNDICE)
| Finding | How to Examine | Significance in Anemia |
|---|---|---|
| Scleral icterus | Look at sclera in good natural light | Elevated indirect bilirubin → hemolysis or megaloblastic anemia |
| Lemon-yellow tinge | Combination of pallor + mild jaundice | Classic of megaloblastic anemia |
| Deep jaundice | Sclera deeply yellow | Severe acute hemolysis (G6PD crisis, transfusion reaction, malaria) |
| No jaundice | IDA, aplastic anemia, CKD anemia |
4. CYANOSIS
- Absent in pure anemia (anemia = low Hb, not desaturated Hb)
- If present → suggests concomitant respiratory/cardiac disease
- Important: Severe anemia can MASK cyanosis (not enough Hb to appear blue even if desaturated)
5. CLUBBING
| Finding | Significance |
|---|---|
| Absent | Most anemias |
| Present | Chronic cyanotic heart disease with polycythemia (opposite of anemia); Infective endocarditis; Crohn's disease (cause of IDA) |
6. LYMPHADENOPATHY
| Finding | Significance |
|---|---|
| Absent | IDA, megaloblastic, aplastic anemia (important - aplastic has NO organomegaly) |
| Present (cervical, axillary, inguinal) | Lymphoma (anemia from marrow infiltration), CLL, infectious mononucleosis (EBV), TB |
| Generalized lymphadenopathy | Lymphoma, leukemia, HIV |
7. EDEMA
| Finding | Significance |
|---|---|
| Pedal edema (bilateral) | High-output cardiac failure from severe chronic anemia |
| Pedal edema + ascites | CLD with portal hypertension → hypersplenism → anemia |
| Peri-orbital edema | Severe hypoalbuminemia (nutritional anemia), nephrotic syndrome |
| No edema | Most mild-moderate anemias |
8. SPECIFIC SIGNS OF IRON DEFICIENCY (Tissue Depletion Signs)
These are found on general physical examination and are highly specific for IDA:
| Sign | Appearance | Where to Look |
|---|---|---|
| Koilonychia | Spoon-shaped (concave) nails | Fingers - especially index and middle finger |
| Angular cheilitis | Painful fissures at corners of mouth | Corners of mouth |
| Atrophic glossitis | Smooth, shiny, red, depapillated tongue | Tongue - compare to normal (should have papillae) |
| Alopecia | Diffuse, non-patchy hair loss | Scalp |
| Brittle nails | Nails break easily, longitudinal ridging | Fingernails |
| Pallor | Pale conjunctivae, palms, nail beds | As above |
| Pica | Craving for ice/clay/chalk (elicited in history) | - |
9. SPECIFIC SIGNS OF MEGALOBLASTIC ANEMIA
| Sign | Appearance |
|---|---|
| Lemon-yellow jaundice | Mild icterus + pallor = lemon-yellow complexion |
| Beefy red, smooth tongue | Glossitis - tongue appears raw, smooth, hyperemic |
| Angular cheilitis | Also seen (B12 + folate both cause this) |
| Vitiligo | Associated with pernicious anemia (autoimmune) |
| Premature greying | Associated with pernicious anemia |
10. SPECIFIC SIGNS OF HEMOLYTIC ANEMIA
| Sign | Appearance | Significance |
|---|---|---|
| Jaundice | Usually moderate, fluctuating | Bilirubin from hemoglobin breakdown |
| Splenomegaly | Palpable spleen (see systemic exam) | Work hypertrophy from RBC destruction |
| Leg ulcers | Medial malleolus | Sickle cell disease, hereditary spherocytosis |
| Frontal bossing | Prominent forehead | Extramedullary hematopoiesis (thalassemia, severe sickle cell) |
| Maxillary overgrowth | "Chipmunk facies" | Thalassemia major (marrow expansion) |
| Tower skull / Hair-on-end skull | Seen on X-ray | Thalassemia major |
| Gall bladder tenderness | RUQ tenderness | Pigment gallstones from chronic hemolysis |
| Skin/mucosal pallor + jaundice together | Classic hemolytic picture |
11. SPECIFIC SIGNS OF APLASTIC ANEMIA
| Sign | Significance |
|---|---|
| Petechiae | Pinpoint red/purple spots on skin - thrombocytopenia |
| Ecchymoses | Large spontaneous bruises - thrombocytopenia |
| Hemorrhagic bullae in mouth | Blood blisters on buccal mucosa - thrombocytopenia |
| Gum bleeding | Spontaneous - thrombocytopenia |
| Pallor | Anemia |
| Fever | Neutropenic infection |
| No splenomegaly | Distinguishes aplastic anemia from leukemia/lymphoma |
| No lymphadenopathy | Distinguishes from lymphoma |
| Café-au-lait spots + short stature + thumb anomalies | Fanconi anemia (inherited aplastic) |
PART 2 - VITAL SIGNS
PULSE
| Finding | Significance |
|---|---|
| Tachycardia | Compensatory - most important vital sign finding in anemia |
| Rate > 100/min | Moderate-severe anemia |
| Low volume pulse | Acute blood loss (reduced stroke volume) |
| High volume, bounding | Chronic severe anemia (high cardiac output state) |
| Collapsing pulse character | Severe high-output state |
| Irregular pulse | Associated cardiac disease (rule out) |
BLOOD PRESSURE
| Finding | Significance |
|---|---|
| Normal BP | Most chronic anemias (compensated) |
| Postural hypotension (>20 mmHg drop systolic on standing) | Acute blood loss, volume depletion |
| Hypotension (lying down) | Severe acute hemorrhage → hypovolemic shock |
| Wide pulse pressure | High-output state in severe chronic anemia |
RESPIRATORY RATE
| Finding | Significance |
|---|---|
| Normal (12-18/min) | Mild-moderate anemia (compensated) |
| Tachypnoea (>18/min) | Severe anemia, pulmonary edema from cardiac failure |
TEMPERATURE
| Finding | Significance |
|---|---|
| Afebrile | IDA, megaloblastic, hemolytic (non-infectious) |
| Febrile | Aplastic anemia (neutropenic sepsis), malaria (hemolytic), lymphoma, hemolytic crisis with infection |
SpO2
- Usually normal in anemia (oxygen saturation measures % saturation, not total O2 content)
- May be low if concomitant respiratory/cardiac disease
- Important teaching point: SpO2 can be falsely NORMAL in severe anemia - patient is hypoxic in terms of O2 delivery but SpO2 reads 98-99%
PART 3 - SYSTEMIC EXAMINATION
A. CARDIOVASCULAR EXAMINATION
Inspection
- Visible apex beat in severe anemia (hyperdynamic circulation)
Palpation
| Finding | Significance |
|---|---|
| Apex beat displaced laterally | Cardiomegaly from longstanding severe anemia |
| Hyperdynamic (forceful, thrusting) apex | High-output state from severe chronic anemia |
| Normal apex position | Mild-moderate anemia |
Auscultation
| Sound | Significance |
|---|---|
| Ejection systolic flow murmur (Grade 2/6, pulmonary area, no radiation) | Hallmark of severe anemia - due to turbulent flow from high cardiac output + low blood viscosity |
| S3 gallop | Cardiac failure complicating severe anemia |
| Organic diastolic murmur | Suggests another cardiac lesion (not from anemia) |
| Loud P2 | Pulmonary hypertension (sickle cell, thalassemia - chronic lung disease) |
Key Teaching: The flow murmur of anemia is systolic, short, soft (≤2/6), and disappears when anemia is treated. It has no diastolic component and no radiation. If diastolic murmur present → organic valvular disease.
B. RESPIRATORY EXAMINATION
| Finding | Significance |
|---|---|
| Usually normal | Most anemias |
| Bilateral basal crepitations | Pulmonary edema from high-output cardiac failure (severe anemia) |
| Dullness at base + reduced breath sounds | Pleural effusion (malignancy causing myelophthisic anemia) |
| Consolidation signs | Neutropenic pneumonia (aplastic anemia) |
C. ABDOMINAL EXAMINATION
SPLEEN - Most Important Abdominal Finding in Anemia
How to Examine the Spleen:
- Patient supine, knees flexed
- Start palpation from right iliac fossa (not left) - palpate diagonally toward left hypochondrium
- Ask patient to take deep breath - feel for splenic notch moving toward you
- If not palpable supine → examine in right lateral decubitus position (brings spleen forward)
- Percussion (Traube's space): Normally resonant (gastric air bubble). Dullness = splenomegaly
- Confirm with percussion: Dull in Traube's space
Spleen Size Classification:
| Grade | Extent of Splenomegaly |
|---|---|
| Grade 1 | Just palpable below costal margin (on deep inspiration) |
| Grade 2 | Up to 4 cm below costal margin |
| Grade 3 | 4-8 cm below costal margin |
| Grade 4 (Massive splenomegaly) | Reaches or crosses umbilicus |
| Grade 5 | Below umbilicus, toward right iliac fossa |
Splenomegaly in Anemia:
| Size | Cause |
|---|---|
| Absent | IDA, megaloblastic anemia, aplastic anemia, CKD anemia |
| Mild-moderate | Autoimmune hemolytic anemia, hereditary spherocytosis, SLE, CLL, infectious mononucleosis |
| Moderate | Thalassemia trait, sickle cell disease (early - later autosplenectomy), warm AIHA |
| Massive (Grade 4-5) | Beta-thalassemia major, CML, myelofibrosis, kala-azar (visceral leishmaniasis), malaria (hyperreactive malarial splenomegaly), Gaucher's disease |
Key Rule: Aplastic anemia does NOT cause splenomegaly. If spleen is palpable, reconsider the diagnosis.
LIVER
| Finding | Significance |
|---|---|
| Normal liver | IDA, megaloblastic, aplastic (usually) |
| Hepatomegaly | CLD with hypersplenism, myelofibrosis, leukemia/lymphoma with liver infiltration, sickle cell (liver sequestration), thalassemia (extramedullary hematopoiesis + iron overload) |
| Hepatosplenomegaly | Leukemia, lymphoma, myelofibrosis, thalassemia major, kala-azar, malaria |
| Tender hepatomegaly | Acute hepatitis (aplastic anemia trigger), right heart failure, malaria |
| Hard, irregular hepatomegaly | Metastatic carcinoma (myelophthisic anemia) |
Remember: Hepatosplenomegaly with anemia in a young patient → think thalassemia or leukemia. In an older patient → think myelofibrosis, lymphoma, or carcinoma.
OTHER ABDOMINAL FINDINGS
| Finding | Significance |
|---|---|
| Ascites | CLD with portal hypertension → hypersplenism; Lymphoma with peritoneal disease |
| RUQ tenderness | Pigment gallstones (chronic hemolysis), hepatitis |
| Epigastric tenderness | Peptic ulcer (cause of GI bleed → IDA) |
| Abdominal mass | Renal carcinoma (hematuria → IDA), colorectal carcinoma (IDA), lymphadenopathy (lymphoma) |
| Midline scar (gastrectomy) | Post-gastrectomy → B12 deficiency / IDA |
D. NEUROLOGICAL EXAMINATION
Neurological examination is mandatory in ALL anemia patients to detect B12 deficiency.
Posterior Column (Dorsal Column) Signs - B12 Deficiency
| Test | Method | Abnormal Finding |
|---|---|---|
| Vibration sense | 128 Hz tuning fork on great toe, medial malleolus, tibial tuberosity, ASIS | Absent at toe = early; absent at knee = advanced |
| Proprioception (Joint position sense) | Move great toe up or down with eyes closed - patient identifies direction | Absent at toes → ankles → knees (progressive) |
| Romberg's test | Stand with feet together, eyes closed | Positive = sways/falls with eyes closed (posterior column loss) |
| Tandem gait | Walk heel-to-toe in a straight line | Ataxic gait (positive) |
| Two-point discrimination | Apply two points on fingertip | Impaired |
Lateral Corticospinal Tract Signs - B12 Deficiency
| Test | Finding |
|---|---|
| Power | Normal or slightly reduced |
| Tone | Increased (spasticity) in lower limbs |
| Deep tendon reflexes | Brisk/exaggerated knee and ankle jerks |
| Plantar response | Extensor (Babinski positive) bilaterally |
Combined Posterior + Lateral Column = Subacute Combined Degeneration of Spinal Cord (SACD)
Pattern: Loss of vibration + proprioception (posterior column) + UMN signs (lateral column) = pathognomonic of B12 deficiency
Additional Neurological Findings in Anemia
| Finding | Cause |
|---|---|
| Fundus: retinal hemorrhages (flame-shaped) | Severe anemia (Hb < 5), thrombocytopenia (aplastic anemia) |
| Papilloedema | Severe anemia (rare), associated raised ICP |
| Peripheral neuropathy (glove-stocking) | B12 deficiency (sensory > motor) |
| Cognitive impairment, dementia | B12 deficiency ("megaloblastic madness") |
| Stroke / focal deficits | Sickle cell disease (cerebral vasoocclusion) |
| Headache | Cerebral hypoxia from severe anemia |
E. MUSCULOSKELETAL / BONE EXAMINATION
| Finding | Significance |
|---|---|
| Frontal bossing | Extramedullary hematopoiesis (thalassemia, severe sickle cell) |
| Maxillary overgrowth ("chipmunk facies") | Thalassemia major |
| Bone tenderness (sternal, spinal, rib tenderness) | Multiple myeloma (myelophthisic anemia), leukemia |
| Leg ulcers (medial malleolus) | Sickle cell disease, hereditary spherocytosis |
| Dactylitis (swollen fingers in infant) | Sickle cell disease (hand-foot syndrome) |
| Short stature + thumb abnormalities | Fanconi anemia |
| Café-au-lait spots | Fanconi anemia |
| Joint swelling | Rheumatoid arthritis (cause of ACD); hemarthrosis in hemophilia |
PART 4 - EXAMINATION FINDINGS BY ANEMIA TYPE (Quick Reference)
| Sign | IDA | Megaloblastic | Hemolytic | Aplastic |
|---|---|---|---|---|
| Pallor | +++ | +++ | +++ | +++ |
| Jaundice | Absent | Lemon-yellow | Present | Absent |
| Koilonychia | Present | Absent | Absent | Absent |
| Angular cheilitis | Present | Present | Absent | Absent |
| Glossitis | Present | Present (beefy red) | Absent | Absent |
| Petechiae/Ecchymoses | Absent | Absent (severe = mild) | Absent | Present |
| Splenomegaly | Absent | Absent | Present | Absent |
| Hepatomegaly | Absent | Absent | Variable | Absent |
| Flow murmur | Present (if severe) | Present (if severe) | Present | Present (if severe) |
| Neurological signs | Absent | SACD signs (B12) | Absent (except sickle) | Absent |
| Lymphadenopathy | Absent | Absent | Absent | Absent |
| Frontal bossing | Absent | Absent | Thalassemia/sickle | Absent |
| Leg ulcers | Absent | Absent | Sickle cell | Absent |
PART 5 - EXAMINATION SUMMARY TEMPLATE
(For writing in case notes)
GENERAL PHYSICAL EXAMINATION:
Built and nourishment: ___________
Pallor: Present/Absent (Grade: +/++/+++)
- Conjunctivae: ___________
- Palms: ___________
- Nail beds: ___________
- Tongue: ___________
Icterus: Present/Absent
Cyanosis: Present/Absent
Clubbing: Present/Absent
Lymphadenopathy: Present/Absent
Edema: Present/Absent
Koilonychia: Present/Absent
Angular cheilitis: Present/Absent
Atrophic glossitis: Present/Absent
Petechiae/Ecchymoses: Present/Absent
VITAL SIGNS:
Pulse: ___/min, regular/irregular, volume: normal/low/high
BP: ___/___ mmHg (Postural drop: Yes/No)
RR: ___/min
Temperature: ___°C
SpO2: ___%
CARDIOVASCULAR:
Apex beat: _____ ICS, _____ (position)
Heart sounds: S1 S2 heard / Flow murmur: Yes/No
Murmur details: ___________
ABDOMEN:
Liver: Palpable/Not palpable (___ cm below costal margin)
Spleen: Palpable/Not palpable (Grade ___, ___ cm below costal margin)
Notch: Present/Absent
Traube's space: Resonant/Dull
Ascites: Present/Absent
CNS:
Vibration sense: Present/Absent at ___________
Proprioception: Present/Absent at ___________
Romberg's test: Positive/Negative
Deep tendon reflexes: Normal/Brisk/Absent
Plantar response: Flexor/Extensor
Fundus: Normal/Retinal hemorrhages
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goldman-Cecil Medicine
Treatment for different Type of anemia
Here is the complete, detailed treatment for all types of anemia - exam-ready with doses, durations, and clinical decision-making.
TREATMENT OF ANEMIA
By Type | Complete MBBS Medicine Reference
GENERAL PRINCIPLES BEFORE STARTING TREATMENT
| Principle | Detail |
|---|---|
| Treat the cause, not just the anemia | Iron tablets alone without finding the bleeding source is incomplete treatment |
| Identify the type first | Wrong treatment can be harmful (folate alone in B12 deficiency worsens neurology) |
| Transfuse when indicated | Hb < 7 g/dL in symptomatic patients; Hb < 8 in cardiac disease |
| Never give blood empirically | Identify the cause first unless patient is hemodynamically unstable |
| Monitor response | Reticulocyte count at 7-10 days; Hb at 4 weeks |
TYPE 1 - IRON DEFICIENCY ANEMIA (IDA)
STEP 1 - TREAT THE CAUSE
| Cause | Specific Treatment |
|---|---|
| Menorrhagia | Gynaecology referral; hormonal therapy, myomectomy, hysterectomy |
| Peptic ulcer | PPI (omeprazole 40 mg OD) + H. pylori eradication if positive |
| Colorectal/gastric carcinoma | Surgical + oncology referral (urgent) |
| Hookworm | Albendazole 400 mg single dose OR Mebendazole 100 mg BD × 3 days |
| Dietary deficiency | Dietary counselling - increase heme iron, reduce tannins |
| Celiac disease | Strict gluten-free diet |
STEP 2 - IRON SUPPLEMENTATION
Oral Iron (First Line)
| Drug | Dose | Timing | Duration |
|---|---|---|---|
| Ferrous sulfate | 200 mg TDS (65 mg elemental iron/tablet) | Empty stomach / 30 min before meals | 3-6 months |
| Ferrous gluconate | 300 mg TDS (36 mg elemental iron/tablet) | Empty stomach | 3-6 months |
| Ferrous fumarate | 200 mg BD-TDS (65 mg elemental iron/tablet) | Empty stomach | 3-6 months |
Target: 150-200 mg elemental iron per day
To enhance absorption:
- Take with Vitamin C (100-200 mg) - increases absorption 2-3 fold
- Avoid taking with tea, milk, antacids, calcium supplements, tetracyclines
Common side effects:
- Constipation (most common)
- Dark/black stools (reassure patient - normal)
- Nausea, epigastric discomfort
- Management: Take after food (reduces GI side effects but also reduces absorption slightly)
Monitoring Oral Iron Response
| Timepoint | Expected Response |
|---|---|
| Day 5-7 | Reticulocytosis (first sign of response) |
| Week 2-3 | Hb starts rising (0.8-1 g/dL per week) |
| Week 4-6 | Hb normalizes |
| Month 3-6 | Continue to replenish stores (ferritin normalizes) |
| Stop when | Ferritin > 50 µg/L (stores replenished) |
Parenteral Iron (IV/IM) - When to Use
Indications for parenteral iron:
| Indication |
|---|
| Non-compliance or intolerance to oral iron |
| Malabsorption (celiac disease, inflammatory bowel disease, post-gastrectomy) |
| Ongoing blood loss exceeding oral replacement capacity |
| Pre-operative optimization (surgery in 2-6 weeks) |
| CKD patients on hemodialysis (on EPO therapy) |
| Severe IDA needing rapid correction |
| Preparation | Route | Dose | Notes |
|---|---|---|---|
| Iron sucrose (Venofer) | IV infusion | 200 mg in 100 mL NS over 15-30 min, repeat doses | Safest IV preparation |
| Ferric carboxymaltose (Ferinject) | IV infusion | Up to 1000 mg in single dose (15 min) | High dose, convenient |
| Iron isomaltoside (Monofer) | IV infusion | Up to 20 mg/kg in single dose | Largest single dose possible |
| Iron dextran | IM (Z-track) / IV | Calculated by formula | Risk of anaphylaxis - test dose required |
Total iron deficit formula (Ganzoni formula):
Total iron (mg) = Body weight (kg) × (Target Hb - Actual Hb) g/dL × 2.4 + 500 (for stores)
Complication of IV iron:
- Anaphylaxis (rare but life-threatening - keep resuscitation ready)
- Hypotension, flushing (infusion reaction)
- Phlebitis at injection site
STEP 3 - BLOOD TRANSFUSION
Indications in IDA:
| Indication | Action |
|---|---|
| Hb < 7 g/dL with symptoms (dyspnoea at rest, angina, syncope) | Transfuse packed RBCs |
| Hb < 8 g/dL with cardiac disease or elderly | Transfuse |
| Pre-operative (Hb < 8, surgery in <24 hours) | Transfuse |
| Hemodynamically unstable from acute blood loss | Emergency transfusion |
| Asymptomatic chronic IDA with Hb > 7 | Do NOT transfuse - treat with iron |
Each unit of packed RBCs raises Hb by approximately 1 g/dL
STEP 4 - ADJUVANTS
| Drug | Dose | Indication |
|---|---|---|
| Folic acid | 5 mg OD | Often co-prescribed (mixed deficiency common, especially in pregnancy) |
| Vitamin C | 100 mg with each iron dose | Enhances iron absorption |
| Erythropoietin (EPO) | 40,000 IU SC weekly | Only in CKD or cancer chemotherapy-associated IDA - not routine |
TYPE 2 - MEGALOBLASTIC ANEMIA
A. VITAMIN B12 DEFICIENCY
Parenteral B12 (Standard Treatment)
| Preparation | Dose | Route | Schedule |
|---|---|---|---|
| Hydroxocobalamin (preferred) | 1000 µg | IM | Daily × 7 days → Weekly × 4 weeks → Monthly lifelong |
| Cyanocobalamin | 1000 µg | IM | Same schedule |
Why IM?
- Pernicious anemia / post-gastrectomy = no intrinsic factor = oral B12 not absorbed via normal pathway
- IM bypasses the need for intrinsic factor completely
Oral B12 (High Dose)
| Indication | Dose | Route | Duration |
|---|---|---|---|
| Dietary deficiency only (veganism) | 1000-2000 µg OD | Oral | Lifelong (or until diet corrected) |
| Unable to tolerate injections | 1000 µg OD | Oral | Lifelong - passive absorption (1% absorbed without IF) |
Monitoring Response to B12 Treatment
| Timepoint | Response |
|---|---|
| 48-72 hours | Subjective improvement in wellbeing |
| Day 5-7 | Reticulocytosis (peak at day 5-10) |
| Week 2 | Hb starts rising |
| Week 6-8 | Hb normalizes |
| Months 3-6 | Neurological improvement (if early) |
| Not reversible if | Neurological damage present > 6 months |
Neurological Response:
- Sensory symptoms often improve first
- Motor and posterior column signs may partially or fully recover
- If no improvement in neurology after 3-6 months → likely permanent damage
Important Precautions
| Precaution | Reason |
|---|---|
| Never give folate alone without correcting B12 | Folate corrects anemia but worsens or unmasks neurological damage from B12 deficiency |
| Check potassium when starting treatment | Rapid cell proliferation consumes potassium → hypokalemia → arrhythmia (especially in elderly) |
| Give folic acid too | B12 and folate work together; combined deficiency is common |
| Lifelong treatment in pernicious anemia/gastrectomy | The cause (no intrinsic factor) cannot be corrected |
B. FOLATE DEFICIENCY
| Drug | Dose | Route | Duration |
|---|---|---|---|
| Folic acid | 5 mg OD | Oral | 4 months (to replenish stores) |
| Folic acid (prophylaxis - pregnancy) | 400-500 µg (0.4-0.5 mg) OD | Oral | From conception to 12 weeks gestation |
| Folic acid (high-risk pregnancy - previous NTD, epilepsy, diabetes) | 5 mg OD | Oral | From 3 months before conception to 12 weeks |
| Folic acid (hemolytic anemia - ongoing rapid RBC turnover) | 5 mg OD | Oral | Lifelong |
| Folinic acid (leucovorin) | Variable | IV/IM | Methotrexate toxicity (rescue therapy) |
Treat the cause:
- Stop offending drugs (methotrexate - switch if possible; phenytoin - liaise with neurology)
- Alcohol abstinence
- Treat malabsorption
TYPE 3 - HEMOLYTIC ANEMIA
Treatment depends on the specific type of hemolysis.
A. G6PD DEFICIENCY (Drug/Oxidant-Induced)
| Step | Action |
|---|---|
| 1. Remove trigger | Stop offending drug (primaquine, dapsone, sulfonamides, nitrofurantoin) immediately |
| 2. IV fluids | Aggressive hydration to protect kidneys from hemoglobin precipitation → acute tubular necrosis |
| 3. Monitor renal function | Daily urea, creatinine, urine output |
| 4. Transfusion | Packed RBCs if Hb < 7 or hemodynamically compromised |
| 5. Folic acid | 5 mg OD to support erythropoiesis |
| 6. Monitor Hb | Rises spontaneously once trigger removed (self-limiting) |
| 7. Patient education | Lifelong avoidance of oxidant triggers; genetic counselling |
Drugs to avoid in G6PD deficiency:
Primaquine, dapsone, nitrofurantoin, sulfonamides, rasburicase, high-dose aspirin, methylene blue, fava beans, naphthalene (mothballs)
B. AUTOIMMUNE HEMOLYTIC ANEMIA (AIHA)
Warm AIHA (IgG - Most Common)
| Line | Treatment | Dose | Notes |
|---|---|---|---|
| 1st line | Prednisolone | 1 mg/kg/day oral | 60-80% respond; taper over 3-6 months once Hb stabilizes |
| 2nd line | Rituximab | 375 mg/m² IV weekly × 4 | Anti-CD20; for steroid-refractory/relapsed cases |
| 2nd line | Splenectomy | Surgical | Removes site of RBC destruction; 60-70% long-term remission |
| 3rd line | Azathioprine | 1-2 mg/kg/day | Steroid-sparing agent |
| 3rd line | Mycophenolate mofetil | 500-1000 mg BD | Steroid-sparing |
| Supportive | Transfusion | Cross-match difficult in AIHA | Use least-incompatible blood; life-threatening cases only |
| Folate | 5 mg OD | Oral | All hemolytic anemias |
Cold Agglutinin Disease (IgM)
| Treatment | Notes |
|---|---|
| Keep patient warm | IgM antibody activates at low temperatures - cold avoidance critical |
| Treat underlying cause | Mycoplasma pneumonia → azithromycin; EBV → supportive; Lymphoma → chemotherapy |
| Rituximab | First-line for symptomatic primary cold agglutinin disease |
| Steroids NOT effective | Unlike warm AIHA |
| Avoid splenectomy | Hemolysis in cold AIHA is primarily intravascular (complement), not splenic |
| Sutimlimab (C1s inhibitor) | New approved therapy for primary cold agglutinin disease (2022) |
C. HEREDITARY SPHEROCYTOSIS
| Severity | Treatment |
|---|---|
| Mild | Folic acid 5 mg OD (lifelong - high RBC turnover); monitor Hb; no splenectomy |
| Moderate | Folic acid; consider splenectomy in adulthood (>6 years age) |
| Severe (Hb < 8 persistently) | Splenectomy - removes primary site of destruction; corrects hemolysis in 90% |
| Aplastic crisis (parvovirus B19) | Transfusion + supportive; IV immunoglobulin in severe cases |
Pre-splenectomy vaccinations (must give ≥2 weeks before):
- Pneumococcal vaccine (PCV13 + PPSV23)
- Meningococcal vaccine
- Haemophilus influenzae type B vaccine
- Annual influenza vaccine
Post-splenectomy:
- Daily prophylactic penicillin V (250 mg BD) - lifelong or minimum 2-5 years
- Risk of overwhelming post-splenectomy infection (OPSI) - especially encapsulated organisms
D. SICKLE CELL DISEASE
Chronic Management
| Drug | Dose | Mechanism | Indication |
|---|---|---|---|
| Hydroxyurea (Hydroxycarbamide) | 15-35 mg/kg/day oral | Increases HbF production → reduces sickling | All moderate-severe SCD; reduces crises by 50% |
| Voxelotor | 1500 mg OD oral | Inhibits HbS polymerization | Approved for SCD anemia; increases Hb |
| Crizanlizumab | 5 mg/kg IV | Anti-P-selectin antibody; prevents vaso-occlusion | Reduces frequency of painful crises |
| L-glutamine | 15 g BD oral | Reduces oxidative stress | Adjunct; reduces acute complications |
| Folic acid | 5 mg OD | Supports erythropoiesis | Lifelong |
| Penicillin V | 125-250 mg BD | OPSI prophylaxis | All children with SCD from 2 months old |
| Pneumococcal + meningococcal vaccines | Per schedule | Prevent encapsulated organism infections | All SCD patients |
Acute Painful Crisis
| Treatment | Detail |
|---|---|
| Analgesia | Mild: paracetamol + NSAIDs / Moderate: tramadol / Severe: IV morphine (0.1 mg/kg q2-4h) |
| IV fluids | 1.5× maintenance (rehydration reduces sickling) |
| Oxygen | Only if SpO2 < 95% (not routine) |
| Transfusion | For acute chest syndrome, stroke, Hb < 5, priapism |
| Exchange transfusion | Stroke, acute chest syndrome (reduces HbS% to <30%) |
| Incentive spirometry | Prevents acute chest syndrome during painful crisis |
Curative Treatment
| Option | Notes |
|---|---|
| Allogeneic stem cell transplantation (HSCT) | Curative; best in children with matched sibling donor; 90%+ cure rate in appropriate candidates |
| Gene therapy (Betibeglogene - Zynteglo; Exagamglogene - Casgevy) | Recently approved; introduces functional beta-globin or corrects HBB gene via CRISPR |
E. THALASSEMIA
Beta-Thalassemia Major (Cooley's Anemia)
| Treatment | Detail |
|---|---|
| Regular blood transfusions | Every 3-4 weeks; maintain pre-transfusion Hb > 9-10 g/dL |
| Iron chelation (mandatory after 10-20 transfusions or ferritin >1000) | Deferasirox 20-40 mg/kg/day oral (Exjade) - FIRST LINE; OR Desferrioxamine 40 mg/kg SC infusion over 8-12 hours, 5-7 nights/week; OR Deferiprone 75 mg/kg/day oral (3 divided doses) - better for cardiac iron |
| Folic acid | 5 mg OD |
| Splenectomy | If hypersplenism causing transfusion requirement >200-250 mL/kg/year |
| Allogeneic HSCT | Curative; best results in young patients (Class I Pesaro) with matched sibling; 90% overall survival |
| Luspatercept (Reblozyl) | 1 mg/kg SC every 3 weeks; reduces transfusion burden in non-transfusion-dependent and transfusion-dependent thalassemia |
| Gene therapy | Betibeglogene (Zynteglo) - approved for beta-thalassemia; provides functional beta-globin |
F. PAROXYSMAL NOCTURNAL HEMOGLOBINURIA (PNH)
| Drug | Mechanism | Dose |
|---|---|---|
| Eculizumab (Soliris) | Anti-C5 complement inhibitor; prevents terminal complement-mediated hemolysis | 600 mg IV weekly × 4 → 900 mg every 2 weeks - lifelong |
| Ravulizumab (Ultomiris) | Long-acting anti-C5; same mechanism | Every 8 weeks IV (convenient dosing) |
| Iptacopan (Fabhalta) | Factor B inhibitor (oral); approved 2023; targets proximal complement | 200 mg BD oral |
| Anticoagulation | Warfarin or LMWH for thrombosis (major cause of death in PNH) | As indicated |
| HSCT | Curative; reserved for severe aplastic anemia component or refractory disease | |
| Meningococcal vaccination | Mandatory before eculizumab (blocks C5 → risk of meningococcal infection) |
TYPE 4 - APLASTIC ANEMIA
TREATMENT ALGORITHM
Confirmed Aplastic Anemia
|
Severity Assessment
|
---------------
| |
Severe/ Moderate
Very Severe |
| Watch and wait
| + Supportive
Age ≤ 40 care
+ Matched |
Sibling? If worsens →
| treat as severe
YES → HSCT
NO → Immunosuppression
A. SUPPORTIVE CARE (ALL PATIENTS)
| Treatment | Indication | Detail |
|---|---|---|
| Packed RBC transfusion | Hb < 7 or symptomatic | Irradiated, leukodepleted blood only |
| Platelet transfusion | Plt < 10,000 OR plt < 20,000 with bleeding | Single donor platelets preferred |
| G-CSF | ANC < 500/µL | 5 µg/kg/day SC; stimulates neutrophil recovery |
| Broad-spectrum antibiotics | Fever + neutropenia | Piperacillin-tazobactam IV ± antifungal (voriconazole/caspofungin) |
| Antifungal | Persistent fever despite antibiotics | Voriconazole or amphotericin B |
| Reverse barrier nursing | All patients | Infection prevention |
| Oestrogen / Tranexamic acid | Menorrhagia (females) | Suppress menstruation to reduce blood loss |
| Avoid NSAIDs | All patients | Worsen platelet function |
B. DEFINITIVE TREATMENT
1. Allogeneic Hematopoietic Stem Cell Transplantation (HSCT)
Indication: Severe/very severe aplastic anemia in patients ≤40 years with HLA-matched sibling donor
| Detail | Information |
|---|---|
| Conditioning regimen | Cyclophosphamide + ATG + Fludarabine (myeloablative) |
| Success rate | 70-90% long-term survival with matched sibling |
| Matched unrelated donor (MUD) | Used if no sibling match; 60-70% survival; more GVHD risk |
| Pre-transplant | Minimize transfusions to reduce allosensitization |
| GVHD prophylaxis | Cyclosporine + methotrexate |
| Outcome | Best in young patients, early transplant, fewer pre-transplant transfusions |
2. Immunosuppressive Therapy (IST)
Indication: Severe/very severe aplastic anemia without matched sibling OR age >40 OR medically unfit for HSCT
| Drug | Dose | Route | Duration |
|---|---|---|---|
| Anti-thymocyte globulin (horse-ATG / Atgam) | 40 mg/kg/day × 4 days | IV infusion | Given once |
| Cyclosporine A | 5 mg/kg/day in 2 divided doses | Oral | 6-12 months; taper slowly |
| Eltrombopag (Promacta) | Start 150 mg OD; titrate to 300 mg | Oral | Combined with ATG+CSA - improves response rates |
| Prednisolone | 1 mg/kg/day | Oral | During ATG (× 4 weeks) - prevents serum sickness |
| G-CSF | 5 µg/kg/day | SC | During and after ATG |
Response assessment at 3-6 months:
- Complete response: Hb normal, ANC >1000, plt >100,000
- Partial response: No longer dependent on transfusions
- No response: Consider 2nd course of ATG, HSCT with unrelated donor, or eltrombopag continuation
3. Eltrombopag (Promacta) - Thrombopoietin Receptor Agonist
| Feature | Detail |
|---|---|
| Mechanism | Stimulates megakaryocyte + hematopoietic stem cell proliferation |
| Current role | Combined with ATG+CSA as first-line IST (improves trilineage response from 30% to 58%) |
| Dose | 150 mg OD (Asian patients: 75 mg OD) |
| Monotherapy | For relapsed/refractory aplastic anemia |
4. Pure Red Cell Aplasia (PRCA)
| Cause | Treatment |
|---|---|
| Thymoma | Thymectomy (corrects PRCA in 30%) + cyclosporine |
| Parvovirus B19 in immunocompromised | IV immunoglobulin (IVIG) 0.4 g/kg/day × 5 days |
| CLL-associated | Treat underlying CLL |
| EPO-antibody associated | Stop EPO; immunosuppression (cyclosporine); HSCT |
| Idiopathic | Cyclosporine; prednisolone; IVIG |
TYPE 5 - ANEMIA OF CHRONIC DISEASE (ACD)
| Priority | Treatment |
|---|---|
| First and foremost | Treat the underlying disease (TB, RA, malignancy, HIV) |
| Iron supplementation | Only if concurrent IDA confirmed (ferritin < 30 + low transferrin saturation) - otherwise, iron is harmful (already trapped, may worsen disease) |
| Erythropoiesis-stimulating agents (ESAs) | Epoetin alfa 40,000 IU SC weekly OR darbepoetin 500 µg SC every 3 weeks; indicated in CKD and cancer chemotherapy-associated anemia; target Hb 10-12 g/dL |
| IV iron + ESA | In CKD on dialysis - combination more effective than ESA alone |
| Transfusion | Hb < 7 or symptomatic - as bridge while treating cause |
TYPE 6 - ANEMIA OF CKD
| Treatment | Drug | Dose | Notes |
|---|---|---|---|
| ESA therapy | Epoetin alfa (Eprex) | 50-300 IU/kg SC/IV 3×/week | Target Hb 10-11.5 g/dL (not >13 - thrombosis risk) |
| Darbepoetin alfa (Aranesp) | 0.45 µg/kg SC/IV weekly or 0.75 µg/kg every 2 weeks | Longer-acting | |
| Roxadustat (HIF-PHI) | 50-200 mg oral TDS | New oral drug; activates endogenous EPO production; approved in India/EU/China | |
| IV iron | Iron sucrose (Venofer) | 100-200 mg IV each dialysis session | Maintains iron for ESA response; ferritin target 200-500 µg/L |
| Treat secondary causes | B12, folate deficiency | As per deficiency | Correct any combined deficiency |
| Transfusion | pRBCs | As needed | Avoid in pre-transplant patients (allosensitization) |
TYPE 7 - MYELOPHTHISIC / MARROW INFILTRATION ANEMIA
| Treatment | Detail |
|---|---|
| Treat underlying cause | Chemotherapy for leukemia/lymphoma/myeloma; hormonal/targeted therapy for metastatic carcinoma |
| Transfusion | Supportive - pRBCs for symptomatic anemia |
| G-CSF | If neutropenia from marrow failure |
| ESA | For chemotherapy-associated anemia |
| Thalidomide / Ruxolitinib | Myelofibrosis (ruxolitinib = JAK1/2 inhibitor - reduces splenomegaly, improves anemia) |
| HSCT | Myelofibrosis - only curative option |
BLOOD TRANSFUSION - GENERAL GUIDELINES
Indications
| Setting | Transfusion Threshold |
|---|---|
| General symptomatic patients | Hb < 7 g/dL |
| Cardiac disease, elderly | Hb < 8 g/dL |
| Active bleeding/hemodynamic instability | Regardless of Hb - clinical decision |
| Pre-operative | Hb < 8 (major surgery); Hb < 10 (cardiac surgery) |
| Thalassemia major | Maintain pre-transfusion Hb > 9-10 g/dL |
| Aplastic anemia | Hb < 7 (irradiated, leukodepleted only) |
| Sickle cell crisis | Hb < 5 or acute chest syndrome/stroke |
| Pregnancy | Hb < 7 (or < 8 with symptoms) |
Types of Blood Products
| Product | Volume | Hb Rise | Indication |
|---|---|---|---|
| Packed RBCs (pRBCs) | 250-350 mL/unit | ~1 g/dL per unit | Anemia |
| Platelets | 250 mL/unit | Raises plt by ~25,000-30,000/unit | Thrombocytopenia with bleeding |
| Fresh Frozen Plasma (FFP) | 250 mL/unit | No Hb effect | Coagulopathy, DIC |
| Cryoprecipitate | 15-20 mL/unit | No Hb effect | Fibrinogen deficiency, von Willebrand disease |
| Whole blood | 450 mL/unit | ~1 g/dL per unit | Acute massive hemorrhage |
SUMMARY TABLE - TREATMENT BY TYPE
| Anemia Type | First-Line Treatment | Curative Option |
|---|---|---|
| IDA | Oral ferrous sulfate + treat cause | Treat underlying cause |
| B12 deficiency | IM hydroxocobalamin monthly lifelong | Treat cause (if dietary) |
| Folate deficiency | Oral folic acid 5 mg × 4 months | Correct cause, stop offending drug |
| G6PD (acute) | Stop trigger + IV fluids + supportive | Avoid triggers lifelong |
| Warm AIHA | Prednisolone 1 mg/kg | Splenectomy / Rituximab |
| Cold AIHA | Keep warm + Rituximab | Treat underlying cause |
| Hereditary spherocytosis | Folic acid ± splenectomy | Splenectomy |
| Sickle cell disease | Hydroxyurea + folic acid + penicillin V | HSCT / Gene therapy |
| Thalassemia major | Transfusions + iron chelation | HSCT / Gene therapy |
| PNH | Eculizumab / Ravulizumab | HSCT |
| Aplastic (severe, ≤40, sibling) | Allogeneic HSCT | HSCT |
| Aplastic (no donor / >40) | ATG + Cyclosporine + Eltrombopag | Unrelated donor HSCT |
| Anemia of chronic disease | Treat underlying disease + ESA | Cure underlying disease |
| CKD anemia | ESA + IV iron | Renal transplant |
| Myelophthisic | Treat primary disease + transfusions | Treat primary disease |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.